- Complications of Diabetes Mellitus

Содержание
- 2. Learning objectives 1. Understand why good diabetic control reduces the incidence of long-term complications. 2. Differentiate
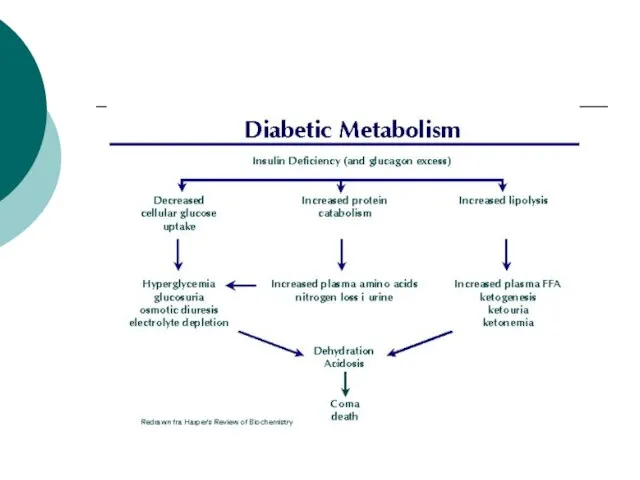
- 3. Diabetes Mellitus Metabolic disease affecting CHO, protein and fat metabolism due to insulin deficiency or inefficiency.
- 5. Complications of diabetes mellitus I. Acute complications: diabetic ketoacidosis hypoglycemia diabetic nonketotic hyperosmolar coma II. Chronic
- 6. Diabetic ketoacidosis (DKA) May be the 1st presentation of type 1 DM. Result from absolute insulin
- 7. Pathophysiology of DKA Ketosis Dehydration Electrolyte imbalance
- 8. Diagnosis of DKA Hyperglycemia Ketonuria and ketonemia Acidosis (PH
- 9. Predisposing factors for DKA Infection Trauma Myocardial Infarction Stroke Surgery Emotional stress
- 10. Clinical presentation of DKA Polyurea and polydepsia. Nausea and vomiting. Anorexia and abdominal pain. Tachycardia. Fruity
- 11. Treatment of DKA Fluid replacement. Insulin therapy for hyperglycemia. Electrolyte correction. Acidosis correction. Treatment of precipitating
- 12. Complication of DKA Cerebral edema Vascular thrombosis Infection M I Acute gastric dilatation Respiratory distress syndrome
- 13. Hypoglycemic coma Hypoglycemia is the most frequent acute complication in type 1 diabetes. Hypoglycemia is the
- 14. Clinical manifestations of hypoglycemia: Autonomic dysfunctions: 1. Hunger 2. Tremor 3. Palpitation 4. Anxiety 5. Pallor
- 15. Neurologic dysfunctions: 1. Impaired thinking 2. Change of mood 3. Irritability 4. Headache 5. Convulsion 6.
- 16. Predisposing factors Missed meal Change in physical activity Alterations or errors in insulin dosage Alcohol ingestion
- 17. Treatment of hypoglycemia In mild cases oral rapidly absorbed carbohydrate In sever cases (comatose patient) iv
- 18. Chronic Complications of DM A. Macrovascular Complications: B. Microvascular Complications:
- 19. Macro-vascular Complications: Ischemic heart diseases. Cerebrovascular diseases. Peripheral vascular diseases. Diabetic patients have a 2 to
- 20. Macro-vascular Complications: Accelerated atherosclerosis involving the aorta and large- and medium-sized arteries. Myocardial infarction, caused by
- 21. Hypertension in DM Type 1 present after several years of DM affects about 30% of patients.
- 22. Dyslipidaemia in DM Most common abnormality is ↓ HDL and ↑ Triglycerides A low HDL is
- 23. Screening for Macrovascular Complications 1. Examine pulses for cardiovascular diseases. 2. Lipogram (lipid profile). 3. ECG.
- 24. Microvascular complications are specific to diabetes and related to longstanding hyperglycaemia. Both Type1 DM and Type2
- 25. Pathophysiology of microvascular disease In diabetes, the microvasculature shows both functional and structural abnormalities. The structural
- 26. The main functional abnormalities include increased capillary permeability, viscosity, and disturbed platelet function. These changes occur
- 27. Platelets from diabetic patients show an exaggerated tendency to aggregate, perhaps mediated by altered prostaglandin metabolism.
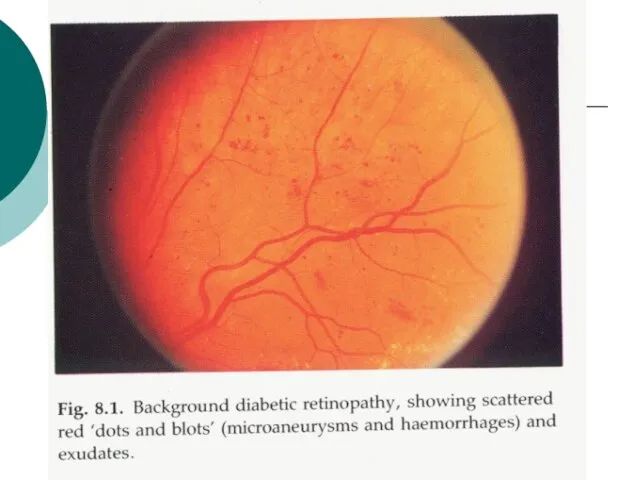
- 28. 1- Diabetic retinopathy * Pathogenesis: Histologically the earliest lesion is thickening of the capillary basement membrane.
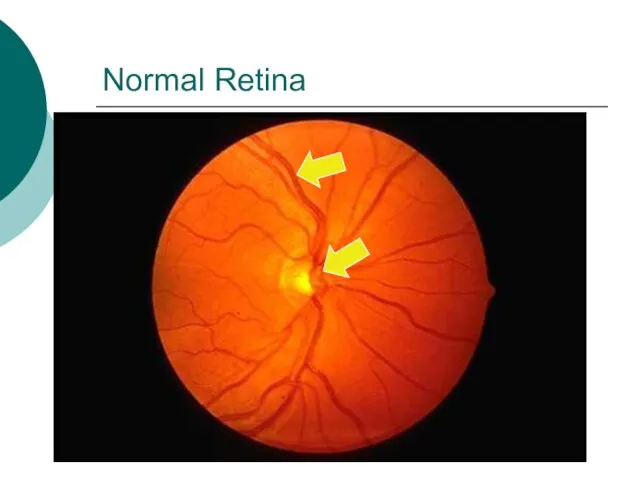
- 29. Normal Retina
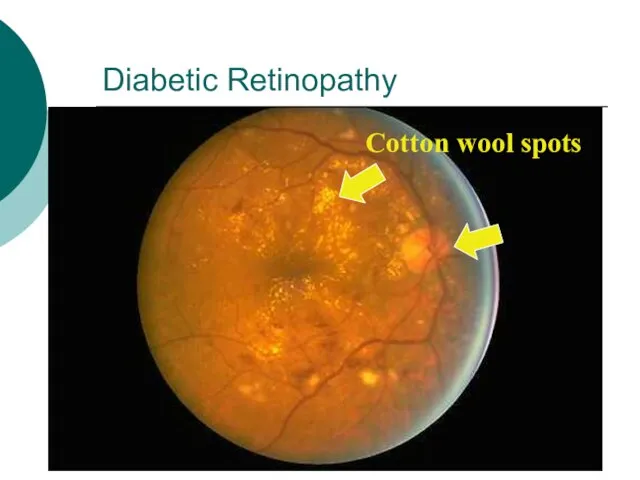
- 31. Diabetic Retinopathy Cotton wool spots
- 32. Other Eye Complications - Cataracts. - Glaucoma - Macular edema. Ischaemic maculopathy. Proliferative retinopathy. Vitreous Bleeding.
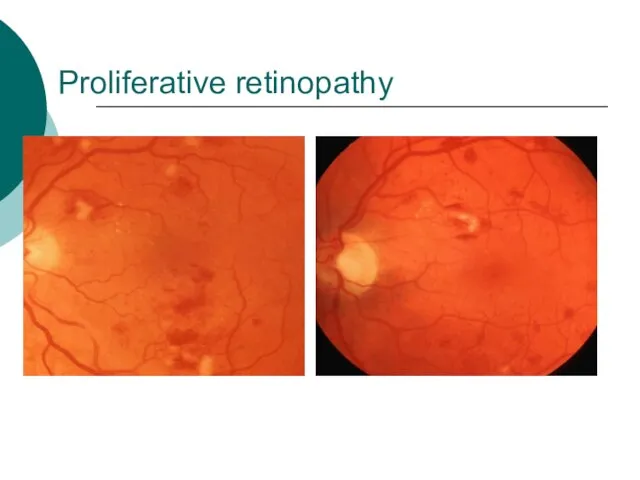
- 33. Proliferative retinopathy
- 34. Vitreous Bleeding
- 35. Rubeosis Iridis
- 36. Proliferative retinopathy. Note the abnormal capillaries and haemorrhages.
- 37. 2- Diabetic Nephropathy (DN) - Diabetic nephropathy is defined by persistent albuminuria (>300 mg/day), decrease glomerular
- 38. Risk factors of DN Duration of DM. Family History of hypertension. Cardiovascular disease, nephropathy. Hyperglycemia. Hypertension.
- 39. Pathogenesis: The glomerular and vascular lesions are linked to hyperglycemia. Nonenzymatic glycosylation to glomerular proteins results
- 40. Pathological pattern of DN Diffuse form (more common): consist of thickining of glomerular basement membrane with
- 41. Diabetic nephropathy • The glomerulus shows sclerotic nodules in the center of the lobules or segments.
- 42. Treatment to prevent progression to DN Glycaemic control. ACE inhibitor . Blood pressure control. Smoking cessation.
- 43. 4. Diabetic Neuropathy 1. Sensorimotor neuropathy. 2. Autonomic neuropathy.
- 44. Sensorimotor Neuropathy Numbness, paresthesias. Feet are mostly affected, hands are seldom affected. Complicated by ulceration (painless),
- 45. Complications of Sensorimotor neuropathy
- 46. Autonomic Neuropathy Postural hypotension. Diabetic diarrhea. Neuropathic bladder. Erectile dysfunction.
- 47. 5. Infections Community acquired pneumonia Acute bacterial cystitis Acute pyelonephritis Pyelonephritis Perinephric abscess Fungal cystitis.
- 48. foot care Patient should check feet daily Wash feet daily Keep toe nails short Protect feet
- 49. Foot ulcer A foot ulcer in a diabetic patient, most probably due to nerve damage. Note
- 50. Diabetic Gangrene – Amp.
- 52. Скачать презентацию
Слайд 2Learning objectives
1. Understand why good diabetic control reduces the incidence of long-term
Learning objectives
1. Understand why good diabetic control reduces the incidence of long-term
Слайд 3Diabetes Mellitus
Metabolic disease affecting CHO, protein and fat metabolism due to insulin
Diabetes Mellitus
Metabolic disease affecting CHO, protein and fat metabolism due to insulin
Слайд 5Complications of diabetes mellitus
I. Acute complications:
diabetic ketoacidosis
hypoglycemia
diabetic nonketotic hyperosmolar coma
II. Chronic complications:
a.
Complications of diabetes mellitus
I. Acute complications:
diabetic ketoacidosis
hypoglycemia
diabetic nonketotic hyperosmolar coma
II. Chronic complications:
a.
Слайд 6Diabetic ketoacidosis (DKA)
May be the 1st presentation of type 1 DM.
Result from
Diabetic ketoacidosis (DKA)
May be the 1st presentation of type 1 DM.
Result from
Слайд 7Pathophysiology of DKA
Ketosis
Dehydration
Electrolyte imbalance
Pathophysiology of DKA
Ketosis
Dehydration
Electrolyte imbalance
Слайд 8Diagnosis of DKA
Hyperglycemia
Ketonuria and ketonemia
Acidosis (PH< 7.3 )
Diagnosis of DKA
Hyperglycemia
Ketonuria and ketonemia
Acidosis (PH< 7.3 )
Слайд 9Predisposing factors for DKA
Infection
Trauma
Myocardial Infarction
Stroke
Surgery
Emotional stress
Predisposing factors for DKA
Infection
Trauma
Myocardial Infarction
Stroke
Surgery
Emotional stress
Слайд 10Clinical presentation of DKA
Polyurea and polydepsia.
Nausea and vomiting.
Anorexia and abdominal pain.
Tachycardia.
Fruity odor
Clinical presentation of DKA
Polyurea and polydepsia.
Nausea and vomiting.
Anorexia and abdominal pain.
Tachycardia.
Fruity odor
Слайд 11Treatment of DKA
Fluid replacement.
Insulin therapy for hyperglycemia.
Electrolyte correction.
Acidosis correction.
Treatment of precipitating
Treatment of DKA
Fluid replacement.
Insulin therapy for hyperglycemia.
Electrolyte correction.
Acidosis correction.
Treatment of precipitating
Слайд 12Complication of DKA
Cerebral edema
Vascular thrombosis
Infection
M I
Acute gastric dilatation
Respiratory distress syndrome
Complication of DKA
Cerebral edema
Vascular thrombosis
Infection
M I
Acute gastric dilatation
Respiratory distress syndrome
Слайд 13 Hypoglycemic coma
Hypoglycemia is the most frequent acute complication in type 1
Hypoglycemic coma
Hypoglycemia is the most frequent acute complication in type 1
Слайд 14Clinical manifestations of hypoglycemia:
Autonomic dysfunctions:
1. Hunger
2. Tremor
3.
Clinical manifestations of hypoglycemia:
Autonomic dysfunctions:
1. Hunger
2. Tremor
3.
Слайд 15Neurologic dysfunctions:
1. Impaired thinking
2. Change of mood
3. Irritability
4.
Neurologic dysfunctions:
1. Impaired thinking
2. Change of mood
3. Irritability
4.
Слайд 16Predisposing factors
Missed meal
Change in physical activity
Alterations or errors in insulin dosage
Alcohol ingestion
Predisposing factors
Missed meal
Change in physical activity
Alterations or errors in insulin dosage
Alcohol ingestion
Слайд 17Treatment of hypoglycemia
In mild cases oral rapidly absorbed carbohydrate
In sever cases (comatose
Treatment of hypoglycemia
In mild cases oral rapidly absorbed carbohydrate
In sever cases (comatose
Слайд 18Chronic Complications of DM
A. Macrovascular Complications:
B. Microvascular Complications:
Chronic Complications of DM
A. Macrovascular Complications:
B. Microvascular Complications:
Слайд 19Macro-vascular Complications:
Ischemic heart diseases.
Cerebrovascular diseases.
Peripheral vascular diseases.
Diabetic patients have a 2
Macro-vascular Complications:
Ischemic heart diseases.
Cerebrovascular diseases.
Peripheral vascular diseases.
Diabetic patients have a 2
Слайд 20Macro-vascular Complications:
Accelerated atherosclerosis involving the aorta and large- and medium-sized arteries.
Myocardial
Macro-vascular Complications:
Accelerated atherosclerosis involving the aorta and large- and medium-sized arteries.
Myocardial
Слайд 21Hypertension in DM
Type 1
present after several years of DM
affects about 30% of
Hypertension in DM
Type 1
present after several years of DM
affects about 30% of
Слайд 22Dyslipidaemia in DM
Most common abnormality is ↓ HDL and ↑ Triglycerides
A low
Dyslipidaemia in DM
Most common abnormality is ↓ HDL and ↑ Triglycerides
A low
Слайд 23Screening for Macrovascular Complications
1. Examine pulses for cardiovascular diseases.
2. Lipogram (lipid profile).
3. ECG.
4. Blood pressure.
Screening for Macrovascular Complications
1. Examine pulses for cardiovascular diseases.
2. Lipogram (lipid profile).
3. ECG.
4. Blood pressure.
Слайд 24Microvascular complications are specific to diabetes and related to longstanding hyperglycaemia.
Both Type1
Microvascular complications are specific to diabetes and related to longstanding hyperglycaemia.
Both Type1
Слайд 25Pathophysiology of microvascular disease
In diabetes, the microvasculature shows both functional and structural
Pathophysiology of microvascular disease
In diabetes, the microvasculature shows both functional and structural
Слайд 26The main functional abnormalities include increased capillary permeability, viscosity, and disturbed platelet
The main functional abnormalities include increased capillary permeability, viscosity, and disturbed platelet
Слайд 27Platelets from diabetic patients show an exaggerated tendency to aggregate, perhaps mediated
Слайд 281- Diabetic retinopathy
* Pathogenesis:
Histologically the earliest lesion is thickening of the
1- Diabetic retinopathy
* Pathogenesis:
Histologically the earliest lesion is thickening of the
Слайд 29Normal Retina
Normal Retina
Слайд 31Diabetic Retinopathy
Cotton wool spots
Diabetic Retinopathy
Cotton wool spots
Слайд 32Other Eye Complications
- Cataracts.
- Glaucoma
- Macular edema.
Ischaemic maculopathy.
Proliferative retinopathy.
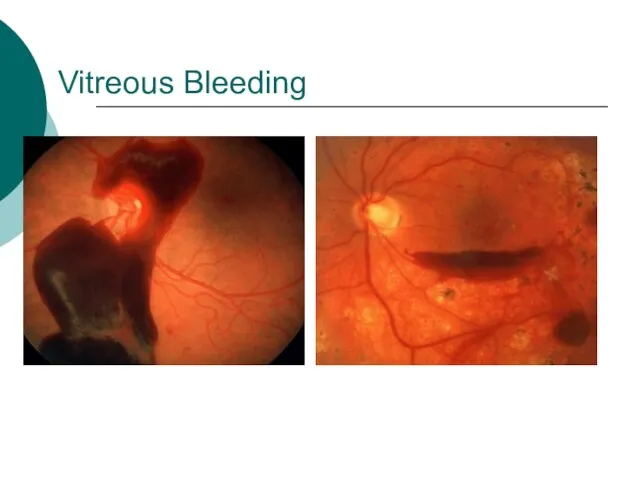
Vitreous Bleeding.
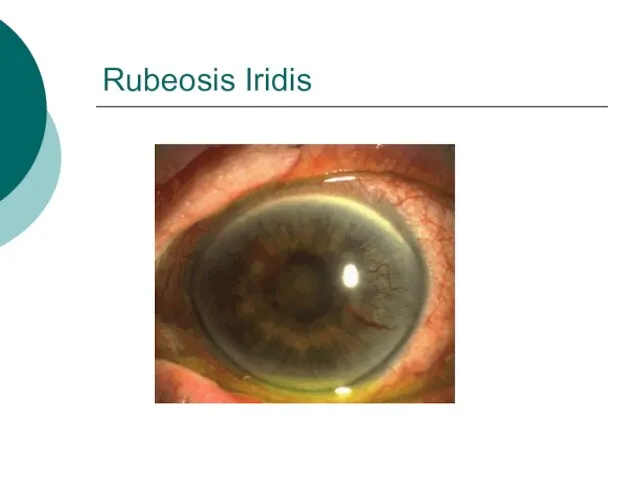
Rubeosis Iridis
Other Eye Complications
- Cataracts.
- Glaucoma
- Macular edema.
Ischaemic maculopathy.
Proliferative retinopathy.
Vitreous Bleeding.
Rubeosis Iridis
Слайд 33Proliferative retinopathy
Proliferative retinopathy
Слайд 34Vitreous Bleeding
Vitreous Bleeding
Слайд 35Rubeosis Iridis
Rubeosis Iridis
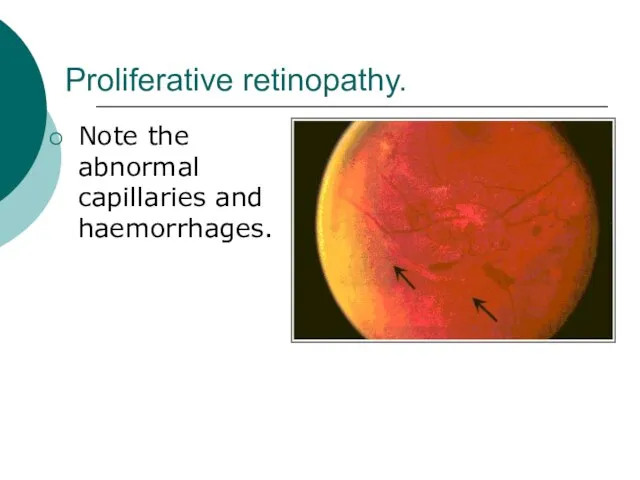
Слайд 36Proliferative retinopathy.
Note the abnormal capillaries and haemorrhages.
Proliferative retinopathy.
Note the abnormal capillaries and haemorrhages.
Слайд 372- Diabetic Nephropathy (DN)
- Diabetic nephropathy is defined by persistent albuminuria (>300
2- Diabetic Nephropathy (DN)
- Diabetic nephropathy is defined by persistent albuminuria (>300
Слайд 38Risk factors of DN
Duration of DM.
Family History of hypertension. Cardiovascular disease, nephropathy.
Hyperglycemia.
Risk factors of DN
Duration of DM.
Family History of hypertension. Cardiovascular disease, nephropathy.
Hyperglycemia.
Слайд 39Pathogenesis:
The glomerular and vascular lesions are linked to hyperglycemia.
Nonenzymatic glycosylation to glomerular
Pathogenesis:
The glomerular and vascular lesions are linked to hyperglycemia.
Nonenzymatic glycosylation to glomerular
Слайд 40Pathological pattern of DN
Diffuse form (more common): consist of thickining of glomerular
Pathological pattern of DN
Diffuse form (more common): consist of thickining of glomerular
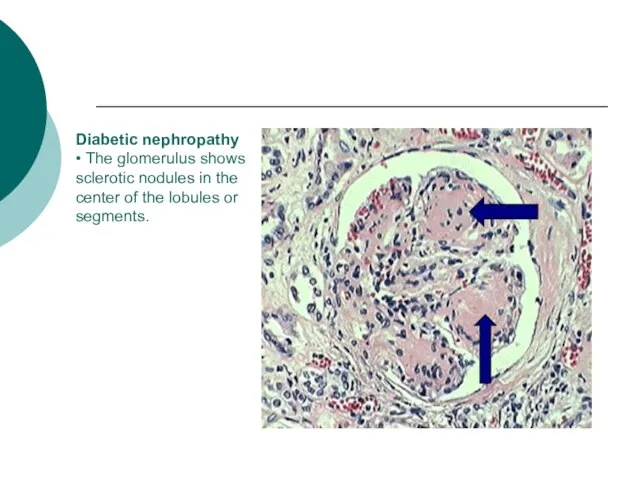
Слайд 41Diabetic nephropathy
• The glomerulus shows sclerotic nodules in the center of the lobules
Diabetic nephropathy • The glomerulus shows sclerotic nodules in the center of the lobules
Слайд 42Treatment to prevent progression to DN
Glycaemic control.
ACE inhibitor .
Blood pressure control.
Smoking cessation.
Proteins
Treatment to prevent progression to DN
Glycaemic control.
ACE inhibitor .
Blood pressure control.
Smoking cessation.
Proteins
Слайд 434. Diabetic Neuropathy
1. Sensorimotor neuropathy.
2. Autonomic neuropathy.
4. Diabetic Neuropathy
1. Sensorimotor neuropathy.
2. Autonomic neuropathy.
Слайд 44Sensorimotor Neuropathy
Numbness, paresthesias.
Feet are mostly affected, hands are seldom affected.
Complicated by ulceration
Sensorimotor Neuropathy
Numbness, paresthesias.
Feet are mostly affected, hands are seldom affected.
Complicated by ulceration
Слайд 45Complications of Sensorimotor neuropathy
Complications of Sensorimotor neuropathy

Слайд 46Autonomic Neuropathy
Postural hypotension.
Diabetic diarrhea.
Neuropathic bladder.
Erectile dysfunction.
Autonomic Neuropathy
Postural hypotension.
Diabetic diarrhea.
Neuropathic bladder.
Erectile dysfunction.
Слайд 475. Infections
Community acquired pneumonia
Acute bacterial cystitis
Acute pyelonephritis
Pyelonephritis
Perinephric abscess
Fungal cystitis.
5. Infections
Community acquired pneumonia
Acute bacterial cystitis
Acute pyelonephritis
Pyelonephritis
Perinephric abscess
Fungal cystitis.
Слайд 48 foot care
Patient should
check feet daily
Wash feet daily
Keep toe nails short
Protect
foot care
Patient should
check feet daily
Wash feet daily
Keep toe nails short
Protect

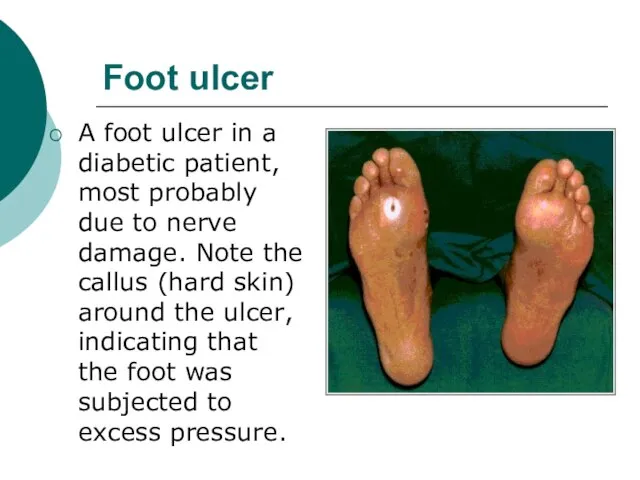
Слайд 49Foot ulcer
A foot ulcer in a diabetic patient, most probably due to
Foot ulcer
A foot ulcer in a diabetic patient, most probably due to
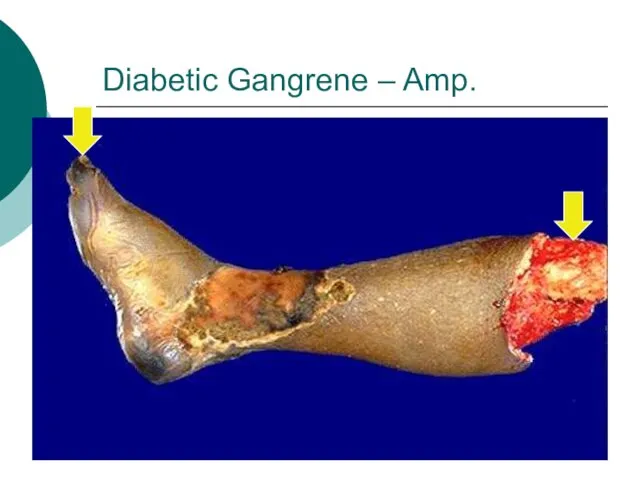
Слайд 50Diabetic Gangrene – Amp.
Diabetic Gangrene – Amp.
 Внедрение в производство беспилотного авиационного комплекса для целей аэрофотосъёмки и организация сервисного предприятия по п
Внедрение в производство беспилотного авиационного комплекса для целей аэрофотосъёмки и организация сервисного предприятия по п Презентация на темуКак зимуют травы, кустарники и деревья
Презентация на темуКак зимуют травы, кустарники и деревья Teaching vocabulary in exam classes
Teaching vocabulary in exam classes Мода и здоровье
Мода и здоровье «Не развив у младшего школьника опыта рефлексии, самоопределения, в основой школе мы получаем целый букет подростковых проблем ни
«Не развив у младшего школьника опыта рефлексии, самоопределения, в основой школе мы получаем целый букет подростковых проблем ни Классификация физических упражнений
Классификация физических упражнений Презентация на тему О жизни и творчестве С. Я. Маршака
Презентация на тему О жизни и творчестве С. Я. Маршака  Презентация на тему Национальный парк Паанаярви
Презентация на тему Национальный парк Паанаярви Презентация на тему Регуляция кислотно-основного равновесия плазмы крови
Презентация на тему Регуляция кислотно-основного равновесия плазмы крови  Карандашова Елена Павловна
Карандашова Елена Павловна Сеть специализированных спортивных магазинов Триал-Спорт
Сеть специализированных спортивных магазинов Триал-Спорт Театр Петрушки
Театр Петрушки Аудирование в формате ЕГЭ
Аудирование в формате ЕГЭ Масс-спектрометрия
Масс-спектрометрия Торговый дом Фарфоровый павильон
Торговый дом Фарфоровый павильон Многообразие карбоновых кислот
Многообразие карбоновых кислот Уральская драматургия
Уральская драматургия Проценты 5 класс
Проценты 5 класс 244115
244115 ИУВР: основа реформирования системы управления водными ресурсамиКеншимов А. К.Кызылорда, 18 октября 2011 года
ИУВР: основа реформирования системы управления водными ресурсамиКеншимов А. К.Кызылорда, 18 октября 2011 года Классный час«О том, как властвовать собой»
Классный час«О том, как властвовать собой» Как быть эффективным при поиске работы
Как быть эффективным при поиске работы Кредитование малого бизнеса в РФ различные оценки кредитоспособности заемщика
Кредитование малого бизнеса в РФ различные оценки кредитоспособности заемщика Аполлон и Дафна
Аполлон и Дафна Народные промыслы. Матрешка
Народные промыслы. Матрешка JavaEE framework structure Components state info and management
JavaEE framework structure Components state info and management Tunti 21
Tunti 21 Українська мова. Завдання
Українська мова. Завдання