- FEATURES OF DRUGS ACTION DURING PREGNANCY

Содержание
- 2. Drug use in pregnancy Drugs can be harmful for the unborn child!!! THE PLACENTA Drugs pass
- 3. Drug use in pregnancy effects of toxic drugs • malformation • growth retardation • fetal death
- 4. Drug use in pregnancy Use of drugs in pregnancy is not always wrong Some examples: •
- 5. Drug use in pregnancy Toxic chemicals and irradiation can damage Oocytes: • all female germ cells
- 6. Drug use in pregnancy Is damaged sperm teratogenic? • Spermatozoa are continuously produced • Damaged spermatozoa
- 7. Drug use in pregnancy The first trimester (day 8 – end of month 2) Is the
- 8. Drug use in pregnancy drugs have effects in newborn • avoid CNS depressants floppy infant syndrome
- 9. Drug use in pregnancy spontaneous malformations (=unknown origin) 2-4 % Additional risk from drugs is small
- 10. Drug use in pregnancy Risk classification (FDA) Category A: Controlled studies in women fail to demonstrate
- 11. Drug use in pregnancy Category B: Either animal reproduction studies have not demonstrated a fetal risk
- 12. Drug use in pregnancy Category C: Either studies in animals have revealed adverse effects on the
- 13. Drug use in pregnancy Category D: There is positive evidence of human fetal risk, but the
- 14. Drug use in pregnancy Category X: Studies in animals or human beings have demonstrated fetal abnormalities,
- 15. Anti-infectives Penicillins Cephalosporins Carbapenems Fluoroquinolones Macrolides Aminoglycosides Sulfonamides Miscellaneous Antibiotics Antivirals Antiretrovirals Antifungals
- 16. Penicillins Category B in pregnancy Cross the placenta easily and rapidly Concentrations equal maternal levels Lactation
- 17. Cephalosporins Category B in pregnancy Cross the placenta during pregnancy Some reports of increased anomalies with
- 18. Carbapenems (ertapenem, imipenem, meropenem) Category B/C/B in pregnancy Likely cross the placenta Very little human data
- 19. Fluoroquinolones Pregnancy Category C Not recommended in pregnancy Cartilage damage in animals Safer alternatives usually exist
- 20. Macrolides (azithromycin, clarithromycin, erythromycin) Pregnancy Categories B/C/B Cross the placenta in low amounts Limited data with
- 21. Aminoglycosides (amikacin, gentamicin, tobramycin) Pregnancy Category C Rapidly cross placenta Enter amniotic fluid through fetal circulation
- 22. Sulfonamides Pregnancy Category C Readily cross the placenta Concerns of use at term Lactation Excreted into
- 23. Tetracyclines (doxycycline, minocycline, tetracycline) Pregnancy Category D Can cause problems with teeth and bone and other
- 24. Miscellaneous Antibiotics Aztreonam Pregnancy Category B, likely safe in pregnancy, little human data Lactation – Compatible
- 25. Miscellaneous Antibiotics Linezolid Pregnancy Category C, no human data available Lactation – unknown, myelosuppression in animals
- 26. Miscellaneous Antibiotics Nitrofurantoin Pregnancy Category B, possible hemolytic anemia with use at term Lactation – Compatible,
- 27. Miscellaneous Antibiotics Vancomycin Pregnancy Category B, compatible Lactation – likely compatible, not absorbed
- 28. Antivirals (acyclovir, famciclovir, valacyclovir) Pregnancy Category B Acyclovir and valacyclovir readily cross the placenta Can be
- 29. Antiretrovirals/NRTI (abacavir, didanosine (ddI), emtricitabine (FTC)) Pregnancy Categories C/B/B Maternal benefit usually outweighs fetal risk Cross
- 30. Antiretrovirals/NRTI (lamuvidine (3TC), stavudine (d4T)) Pregnancy Category C Maternal benefit usually outweighs fetal risk Cross the
- 31. Antiretrovirals/NRTI (tenofivir, zalcitabine (ddC), zidovudine (AZT)) Pregnancy Category B/C/C Maternal benefit usually outweighs fetal risk Cross
- 32. Antiretrovirals/NNRTI (delavirdine, efavirenz, nevirapine) Pregnancy Category C Maternal risk usually outweighs fetal risk Likely cross into
- 33. Antiretrovirals/PI Pregnancy Category B/C Maternal benefit usually outweighs fetal risk Likely cross the placenta All PIs
- 34. Antiretrovirals/Fusion Inhibitor (enfuvirtide) Pregnancy Category B Maternal benefit usually outweighs fetal risk Very large molecule (4492
- 35. Antifungals/Azoles (fluconazole, itraconazole, ketoconazole, posaconazole, voriconazole) Pregnancy Categories C/C/C/D/D Likely cross placenta Fluconazole > 400mg/day seems
- 36. Antifungals/Azoles (fluconazole, itraconazole, ketoconazole, posaconazole, voriconazole) Lactation Fluconazole is compatible per AAP Itraconazole could concentrate in
- 37. Antifungals/Echinocandins (anidulofungin, caspofungin, micafungin) Pregnancy Category C No data with anidulofungin No human data with caspofungin,
- 38. Antifungals/Polyenes Amphotericin B Pregnancy Category B, compatible, lipid complexes also compatible Lactation – no data available
- 39. Migraine Headache Therapy Triptans Ergots Butalbital Caffeine Dichloralphenazone Isometheptene
- 40. Triptans (5-HT1 agonists) Pregnancy Category C Limited human data exists, sumatriptan has been associated with VSDs
- 41. Triptans (5-HT1 agonists) Lactation Cross into breastmilk and may concentrate No reports of human lactation with
- 42. Ergots (Dihydroergotamine, ergotamine) Pregnancy Category X Oxytocic properties could cause IUGR by vascular disruption or increased
- 43. Butalbital and Caffeine Butalbital Pregnancy Category C, can see neonatal withdrawal symptoms with long-term use Lactation
- 44. Dichloralphenazone and Isometheptene (Midrin) Dichloralphenazone Pregnancy Category B Lactation – similar agent considered compatible Isometheptene Pregnancy
- 45. Safe Drug Administration in children Administration of drugs during the first year of life can be
- 46. The Neonate – birth to 4 weeks
- 47. Neonate - Absorption Two major factors affect the absorption of drugs pH dependent passive diffusion Gastric
- 48. Gastric pH Gastric pH (6-8) is directly related to the presence of amniotic fluid in the
- 49. Gastric pH in premature infant In the premature infants, gastric pH may remain elevated due to
- 50. Delayed Absorption in neonate Prolonged emptying is seen in premature infant In the neonatal period the
- 51. Absorption from skin and muscle in neonate Percutaneous absorption may be drastically increased due to immature
- 52. Distribution drugs in children Distribution of drugs within the body is influenced by the amount and
- 53. Total Body Water 85 % in pre-term infant 78% in neonate 60% at 1 year 64
- 54. Metabolism in infants Hepatic enzyme activity and plasma / tissue esterase activity are both reduced during
- 55. Neonate Renal Excretion Renal Excretion At birth, glomerular function is more advanced that tubular function this
- 56. Infant – 5 weeks to 1 year
- 57. Infant - Absorption Low acidity in stomach until around 2 years of age Gastric emptying still
- 58. Absorption - IM Injected drugs are often erratically absorbed because of variability in muscle mass amount
- 59. Absorption - transdermal May be enhanced in young children because the stratum corneum is thin and
- 60. Absorption – transrectal Transrectal is dependent on placement of the drug within the rectal cavity Good
- 61. Absorption - lungs Varies less by physiologic parameters and more by reliability of the delivery device
- 62. Meds via mask
- 63. Infant - Distribution Protein-binding capacity reaches adult values within 10 to 12 months Higher doses (mg
- 64. Infant – Hepatic Metabolism Complete maturation of the liver develops by one year Cytochrome P-450 enzyme
- 65. Infant – Renal Excretion Renal elimination depends on plasma protein binding, renal blood flow, GFR and
- 66. Drug Dosing Dosing in children less than 12 years is always of function of age, body
- 67. Child – 1 to 12 years
- 69. Скачать презентацию
Слайд 3Drug use in pregnancy
effects of toxic drugs
• malformation
• growth retardation
• fetal death
•
Drug use in pregnancy
effects of toxic drugs
• malformation
• growth retardation
• fetal death
•
Слайд 4Drug use in pregnancy
Use of drugs in pregnancy is not always wrong
Some
Drug use in pregnancy
Use of drugs in pregnancy is not always wrong
Some
Слайд 5Drug use in pregnancy
Toxic chemicals and irradiation can damage
Oocytes:
• all female germ
Drug use in pregnancy
Toxic chemicals and irradiation can damage
Oocytes:
• all female germ
Слайд 6Drug use in pregnancy
Is damaged sperm teratogenic?
• Spermatozoa are continuously produced
• Damaged
Drug use in pregnancy
Is damaged sperm teratogenic?
• Spermatozoa are continuously produced
• Damaged
Слайд 7Drug use in pregnancy
The first trimester (day 8 – end of month
Drug use in pregnancy
The first trimester (day 8 – end of month
Слайд 8Drug use in pregnancy
drugs have effects in newborn
• avoid CNS depressants
floppy infant
Drug use in pregnancy
drugs have effects in newborn
• avoid CNS depressants
floppy infant
Слайд 9Drug use in pregnancy
spontaneous malformations (=unknown origin)
2-4 %
Additional risk from drugs is
Drug use in pregnancy
spontaneous malformations (=unknown origin)
2-4 %
Additional risk from drugs is
Слайд 10Drug use in pregnancy
Risk classification (FDA)
Category A:
Controlled studies in women fail to
Drug use in pregnancy
Risk classification (FDA)
Category A:
Controlled studies in women fail to
Слайд 11Drug use in pregnancy
Category B:
Either animal reproduction studies have not
demonstrated a fetal
Drug use in pregnancy
Category B:
Either animal reproduction studies have not
demonstrated a fetal
Слайд 12Drug use in pregnancy
Category C:
Either studies in animals have revealed adverse
effects on
Drug use in pregnancy
Category C:
Either studies in animals have revealed adverse
effects on
Слайд 13Drug use in pregnancy
Category D:
There is positive evidence of human fetal risk,
but
Drug use in pregnancy
Category D:
There is positive evidence of human fetal risk,
but
Слайд 14Drug use in pregnancy
Category X:
Studies in animals or human beings have
demonstrated fetal
Drug use in pregnancy
Category X:
Studies in animals or human beings have
demonstrated fetal
Слайд 15Anti-infectives
Penicillins
Cephalosporins
Carbapenems
Fluoroquinolones
Macrolides
Aminoglycosides
Sulfonamides
Miscellaneous Antibiotics
Antivirals
Antiretrovirals
Antifungals
Anti-infectives
Penicillins
Cephalosporins
Carbapenems
Fluoroquinolones
Macrolides
Aminoglycosides
Sulfonamides
Miscellaneous Antibiotics
Antivirals
Antiretrovirals
Antifungals
Слайд 16Penicillins
Category B in pregnancy
Cross the placenta easily and rapidly
Concentrations equal maternal levels
Lactation
Crosses
Penicillins
Category B in pregnancy
Cross the placenta easily and rapidly
Concentrations equal maternal levels
Lactation
Crosses
Слайд 17Cephalosporins
Category B in pregnancy
Cross the placenta during pregnancy
Some reports of increased anomalies
Cephalosporins
Category B in pregnancy
Cross the placenta during pregnancy
Some reports of increased anomalies
Слайд 18Carbapenems
(ertapenem, imipenem, meropenem)
Category B/C/B in pregnancy
Likely cross the placenta
Very little human data
Lactation
Carbapenems
(ertapenem, imipenem, meropenem)
Category B/C/B in pregnancy
Likely cross the placenta
Very little human data
Lactation
Слайд 19
Fluoroquinolones
Pregnancy Category C
Not recommended in pregnancy
Cartilage damage in animals
Safer alternatives usually exist
Lactation
Excreted
Fluoroquinolones
Pregnancy Category C
Not recommended in pregnancy
Cartilage damage in animals
Safer alternatives usually exist
Lactation
Excreted
Слайд 20Macrolides
(azithromycin, clarithromycin, erythromycin)
Pregnancy Categories B/C/B
Cross the placenta in low amounts
Limited data with
Macrolides
(azithromycin, clarithromycin, erythromycin)
Pregnancy Categories B/C/B
Cross the placenta in low amounts
Limited data with
Слайд 21Aminoglycosides
(amikacin, gentamicin, tobramycin)
Pregnancy Category C
Rapidly cross placenta
Enter amniotic fluid through fetal
Aminoglycosides
(amikacin, gentamicin, tobramycin)
Pregnancy Category C
Rapidly cross placenta
Enter amniotic fluid through fetal
Слайд 22Sulfonamides
Pregnancy Category C
Readily cross the placenta
Concerns of use at term
Lactation
Excreted into breastmilk
Sulfonamides
Pregnancy Category C
Readily cross the placenta
Concerns of use at term
Lactation
Excreted into breastmilk
Слайд 23Tetracyclines
(doxycycline, minocycline, tetracycline)
Pregnancy Category D
Can cause problems with teeth and bone
Tetracyclines
(doxycycline, minocycline, tetracycline)
Pregnancy Category D
Can cause problems with teeth and bone
Слайд 24Miscellaneous Antibiotics
Aztreonam
Pregnancy Category B, likely safe in pregnancy, little human data
Lactation –
Miscellaneous Antibiotics
Aztreonam
Pregnancy Category B, likely safe in pregnancy, little human data
Lactation –
Слайд 25Miscellaneous Antibiotics
Linezolid
Pregnancy Category C, no human data available
Lactation – unknown, myelosuppression in
Miscellaneous Antibiotics
Linezolid
Pregnancy Category C, no human data available
Lactation – unknown, myelosuppression in
Слайд 26Miscellaneous Antibiotics
Nitrofurantoin
Pregnancy Category B, possible hemolytic anemia with use at term
Lactation –
Miscellaneous Antibiotics
Nitrofurantoin
Pregnancy Category B, possible hemolytic anemia with use at term
Lactation –
Слайд 27Miscellaneous Antibiotics
Vancomycin
Pregnancy Category B, compatible
Lactation – likely compatible, not absorbed
Miscellaneous Antibiotics
Vancomycin
Pregnancy Category B, compatible
Lactation – likely compatible, not absorbed
Слайд 28Antivirals
(acyclovir, famciclovir, valacyclovir)
Pregnancy Category B
Acyclovir and valacyclovir readily cross the placenta
Can be
Antivirals
(acyclovir, famciclovir, valacyclovir)
Pregnancy Category B
Acyclovir and valacyclovir readily cross the placenta
Can be
Слайд 29Antiretrovirals/NRTI
(abacavir, didanosine (ddI), emtricitabine (FTC))
Pregnancy Categories C/B/B
Maternal benefit usually outweighs fetal
Antiretrovirals/NRTI
(abacavir, didanosine (ddI), emtricitabine (FTC))
Pregnancy Categories C/B/B
Maternal benefit usually outweighs fetal
Слайд 30Antiretrovirals/NRTI
(lamuvidine (3TC), stavudine (d4T))
Pregnancy Category C
Maternal benefit usually outweighs fetal risk
Cross the
Antiretrovirals/NRTI
(lamuvidine (3TC), stavudine (d4T))
Pregnancy Category C
Maternal benefit usually outweighs fetal risk
Cross the
Слайд 31Antiretrovirals/NRTI
(tenofivir, zalcitabine (ddC), zidovudine (AZT))
Pregnancy Category B/C/C
Maternal benefit usually outweighs fetal risk
Cross
Antiretrovirals/NRTI
(tenofivir, zalcitabine (ddC), zidovudine (AZT))
Pregnancy Category B/C/C
Maternal benefit usually outweighs fetal risk
Cross
Слайд 32Antiretrovirals/NNRTI
(delavirdine, efavirenz, nevirapine)
Pregnancy Category C
Maternal risk usually outweighs fetal risk
Likely cross into
Antiretrovirals/NNRTI
(delavirdine, efavirenz, nevirapine)
Pregnancy Category C
Maternal risk usually outweighs fetal risk
Likely cross into
Слайд 33
Antiretrovirals/PI
Pregnancy Category B/C
Maternal benefit usually outweighs fetal risk
Likely cross the placenta
All PIs
Antiretrovirals/PI
Pregnancy Category B/C
Maternal benefit usually outweighs fetal risk
Likely cross the placenta
All PIs
Слайд 34Antiretrovirals/Fusion Inhibitor
(enfuvirtide)
Pregnancy Category B
Maternal benefit usually outweighs fetal risk
Very large molecule
Antiretrovirals/Fusion Inhibitor
(enfuvirtide)
Pregnancy Category B
Maternal benefit usually outweighs fetal risk
Very large molecule
Слайд 35Antifungals/Azoles
(fluconazole, itraconazole, ketoconazole, posaconazole, voriconazole)
Pregnancy Categories C/C/C/D/D
Likely cross placenta
Fluconazole > 400mg/day
Antifungals/Azoles
(fluconazole, itraconazole, ketoconazole, posaconazole, voriconazole)
Pregnancy Categories C/C/C/D/D
Likely cross placenta
Fluconazole > 400mg/day
Слайд 36Antifungals/Azoles
(fluconazole, itraconazole, ketoconazole, posaconazole, voriconazole)
Lactation
Fluconazole is compatible per AAP
Itraconazole could concentrate in
Antifungals/Azoles
(fluconazole, itraconazole, ketoconazole, posaconazole, voriconazole)
Lactation
Fluconazole is compatible per AAP
Itraconazole could concentrate in
Слайд 37Antifungals/Echinocandins
(anidulofungin, caspofungin, micafungin)
Pregnancy Category C
No data with anidulofungin
No human data with caspofungin,
Antifungals/Echinocandins
(anidulofungin, caspofungin, micafungin)
Pregnancy Category C
No data with anidulofungin
No human data with caspofungin,
Слайд 38Antifungals/Polyenes
Amphotericin B
Pregnancy Category B, compatible, lipid complexes also compatible
Lactation – no data
Antifungals/Polyenes
Amphotericin B
Pregnancy Category B, compatible, lipid complexes also compatible
Lactation – no data
Слайд 39Migraine Headache Therapy
Triptans
Ergots
Butalbital
Caffeine
Dichloralphenazone
Isometheptene
Migraine Headache Therapy
Triptans
Ergots
Butalbital
Caffeine
Dichloralphenazone
Isometheptene
Слайд 40Triptans (5-HT1 agonists)
Pregnancy Category C
Limited human data exists, sumatriptan has been associated
Triptans (5-HT1 agonists)
Pregnancy Category C
Limited human data exists, sumatriptan has been associated
Слайд 41Triptans (5-HT1 agonists)
Lactation
Cross into breastmilk and may concentrate
No reports of human lactation
Triptans (5-HT1 agonists)
Lactation
Cross into breastmilk and may concentrate
No reports of human lactation
Слайд 42Ergots
(Dihydroergotamine, ergotamine)
Pregnancy Category X
Oxytocic properties could cause IUGR by vascular disruption or
Ergots
(Dihydroergotamine, ergotamine)
Pregnancy Category X
Oxytocic properties could cause IUGR by vascular disruption or
Слайд 43Butalbital and Caffeine
Butalbital
Pregnancy Category C, can see neonatal withdrawal symptoms with long-term
Butalbital and Caffeine
Butalbital
Pregnancy Category C, can see neonatal withdrawal symptoms with long-term
Слайд 44Dichloralphenazone and Isometheptene (Midrin)
Dichloralphenazone
Pregnancy Category B
Lactation – similar agent considered compatible
Isometheptene
Pregnancy Category
Dichloralphenazone and Isometheptene (Midrin)
Dichloralphenazone
Pregnancy Category B
Lactation – similar agent considered compatible
Isometheptene
Pregnancy Category
Слайд 45
Safe Drug Administration in children
Administration of drugs during the first year of
Safe Drug Administration in children
Administration of drugs during the first year of
Слайд 46The Neonate – birth to 4 weeks
The Neonate – birth to 4 weeks
Слайд 47Neonate - Absorption
Two major factors affect the absorption of drugs
pH dependent passive
Neonate - Absorption
Two major factors affect the absorption of drugs
pH dependent passive
Слайд 48Gastric pH
Gastric pH (6-8) is directly related to the presence of amniotic
Gastric pH
Gastric pH (6-8) is directly related to the presence of amniotic
Слайд 49Gastric pH in premature infant
In the premature infants, gastric pH may remain
Gastric pH in premature infant
In the premature infants, gastric pH may remain
Слайд 50Delayed Absorption in neonate
Prolonged emptying is seen in premature infant
In the neonatal
Delayed Absorption in neonate
Prolonged emptying is seen in premature infant
In the neonatal
Слайд 51Absorption from skin and muscle in neonate
Percutaneous absorption may be drastically increased
Absorption from skin and muscle in neonate
Percutaneous absorption may be drastically increased
Слайд 52Distribution drugs in children
Distribution of drugs within the body is influenced by
Distribution drugs in children
Distribution of drugs within the body is influenced by
Слайд 53Total Body Water
85 % in pre-term infant
78% in neonate
60% at
Total Body Water
85 % in pre-term infant
78% in neonate
60% at

Слайд 54Metabolism in infants
Hepatic enzyme activity and plasma / tissue esterase activity are
Metabolism in infants
Hepatic enzyme activity and plasma / tissue esterase activity are
Слайд 55Neonate Renal Excretion
Renal Excretion
At birth, glomerular function is more advanced that tubular
Neonate Renal Excretion
Renal Excretion
At birth, glomerular function is more advanced that tubular
Слайд 56Infant – 5 weeks to 1 year
Infant – 5 weeks to 1 year
Слайд 57Infant - Absorption
Low acidity in stomach until around 2 years of age
Gastric
Infant - Absorption
Low acidity in stomach until around 2 years of age
Gastric
Слайд 58Absorption - IM
Injected drugs are often erratically absorbed because of variability in
Absorption - IM
Injected drugs are often erratically absorbed because of variability in
Слайд 59Absorption - transdermal
May be enhanced in young children because the stratum corneum
Absorption - transdermal
May be enhanced in young children because the stratum corneum
Слайд 60Absorption – transrectal
Transrectal is dependent on placement of the drug within
Absorption – transrectal
Transrectal is dependent on placement of the drug within
Слайд 61Absorption - lungs
Varies less by physiologic parameters and more by reliability of
Absorption - lungs
Varies less by physiologic parameters and more by reliability of
Слайд 62Meds via mask
Meds via mask
Слайд 63Infant - Distribution
Protein-binding capacity reaches adult values within 10 to 12 months
Higher
Infant - Distribution
Protein-binding capacity reaches adult values within 10 to 12 months
Higher
Слайд 64Infant – Hepatic Metabolism
Complete maturation of the liver develops by one year
Cytochrome
Infant – Hepatic Metabolism
Complete maturation of the liver develops by one year
Cytochrome
Слайд 65Infant – Renal Excretion
Renal elimination depends on plasma protein binding, renal blood
Infant – Renal Excretion
Renal elimination depends on plasma protein binding, renal blood
Слайд 66Drug Dosing
Dosing in children less than 12 years is always of function
Drug Dosing
Dosing in children less than 12 years is always of function
Слайд 67Child – 1 to 12 years
Child – 1 to 12 years
 Funny English
Funny English Презентация на тему Загадки про овощи
Презентация на тему Загадки про овощи  Однокоренные слова
Однокоренные слова Готическое искусство средневековья
Готическое искусство средневековья Північна Америка
Північна Америка 315 Быть может зарёй
315 Быть может зарёй Использование ЭОР при подготовке к олимпиадам и во внеурочной деятельности
Использование ЭОР при подготовке к олимпиадам и во внеурочной деятельности Владислав Бельский Член Правления
Владислав Бельский Член Правления Решение логических задач табличным способом
Решение логических задач табличным способом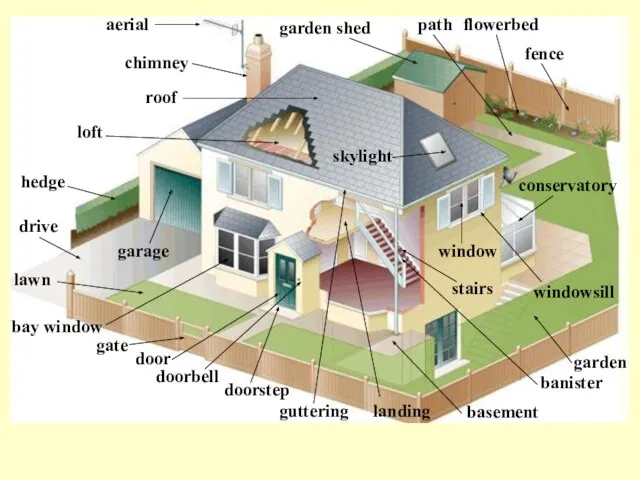 House cottage
House cottage Разработка урока по алгебре в 7 классе
Разработка урока по алгебре в 7 классе Художественная культура второй половины XIX – начала XX века
Художественная культура второй половины XIX – начала XX века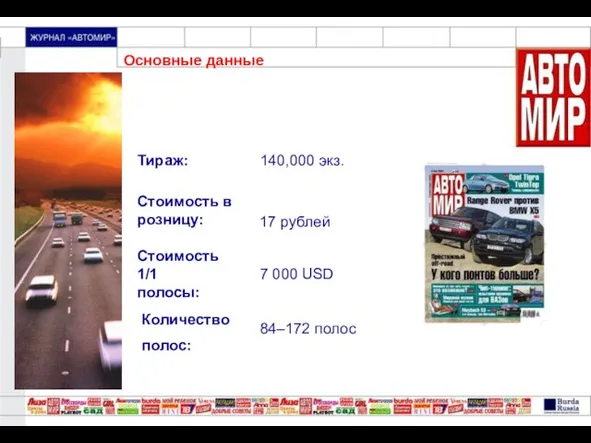 Основные данные
Основные данные Трудности при сварке чугуна
Трудности при сварке чугуна Старинные машины
Старинные машины Групи платників єдиного податку
Групи платників єдиного податку Советы олимпиаднику
Советы олимпиаднику Музыкально-развлекательный, рекламный проект Будьте здоровы, дети Крыма!
Музыкально-развлекательный, рекламный проект Будьте здоровы, дети Крыма! «Волгоград. План города.» версия 2.0 г. Волгоград, 2007
«Волгоград. План города.» версия 2.0 г. Волгоград, 2007 Шарль Перро
Шарль Перро Документальные основы становления и развития системы общественного дошкольного образования
Документальные основы становления и развития системы общественного дошкольного образования Пьер Жане (1859-1947)
Пьер Жане (1859-1947) Экология в русских народных сказках
Экология в русских народных сказках How to Use Lessons Learned at Apple at Your Dealership
How to Use Lessons Learned at Apple at Your Dealership Сказки
Сказки Христианство
Христианство Контрольная работа по теме: Опорно – двигательная система
Контрольная работа по теме: Опорно – двигательная система Военные аспекты международного гуманитарного права
Военные аспекты международного гуманитарного права