- Modern approach to treatment of CIN and micro-invasive

Содержание
- 2. Hans Hinselman Colposcopy, 1924 George Pappanicolaou Cytology, 1945
- 3. Cervical cancer has become detectable and curable disease.
- 4. Recently, however, significant controversy has arisen over several aspects of the diagnosis and management of cervical
- 5. There is no dispute about the need to treat CIN 3 and few would argue that
- 6. These two grades of CIN (CIN 2 and CIN 3) are referred to as high-grade lesions
- 7. In the spectrum of cervical pathology the line between premalignant and benign lesions may be drawn
- 8. L-SIL High proportion of women affected Low risk of progression Significant regression may occur
- 9. Management of CIN 1 (L-SIL) Conservative Active
- 10. Management of L-SIL Close observation with cytologic and possibly colposcopic follow-up, without active treatment is the
- 14. Expectant management of CIN 1 is not totally without some risk...
- 15. ……. because of the: potential for a high-grade lesion to develop during follow-up already existing high-grade
- 18. If large lesions or persistent lesions are present or if the patient is at risk for
- 20. Active management of women with CIN 1 is recommended in the following cases: Unsatisfactory colposcopy Large,
- 21. Women with biopsy confirmed H-SIL (CIN 2 and 3) have significant risk of disease progression to
- 24. The expectant management of CIN 2 and 3 with repeat cytology and colposcopy is not acceptable
- 27. Destruction or Excision ?
- 28. Management of HSIL excision recommended cold-knife laser conization LLETZ
- 29. Excision is necessary in: Unsatisfactory examination Large lesions Recurrent disease
- 33. Unless there are other compelling reasons for performing a hysterectomy, this procedure is considered unacceptable as
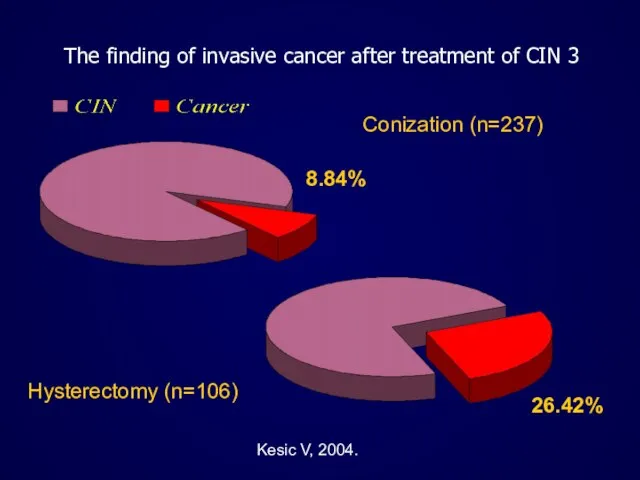
- 34. The finding of invasive cancer after treatment of CIN 3 Conization (n=237) 8.84% Hysterectomy (n=106) 26.42%
- 39. Vesna Kesic Institute of Obstetrics and Gynecology Clinical Center of Serbia International Scientific Conference Prevention of
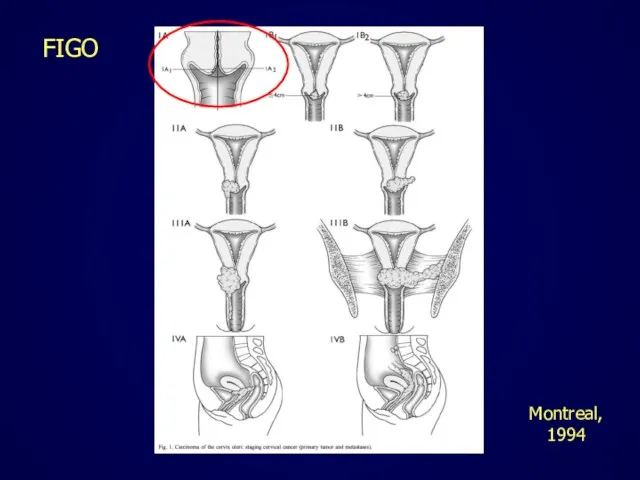
- 40. Treatment of cervical cancer is affected by the stage of the disease.
- 41. FIGO Montreal, 1994
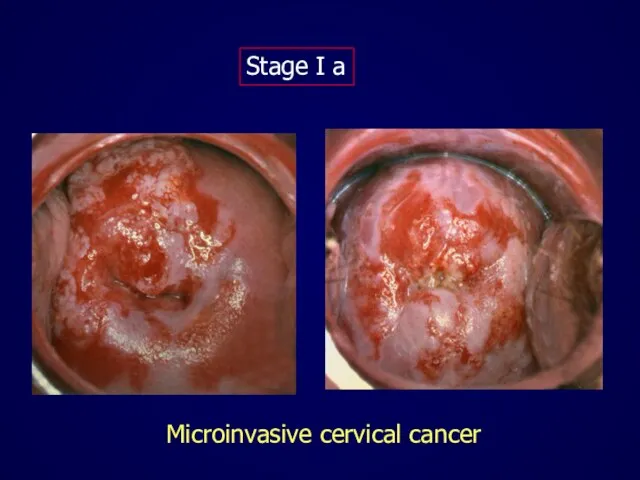
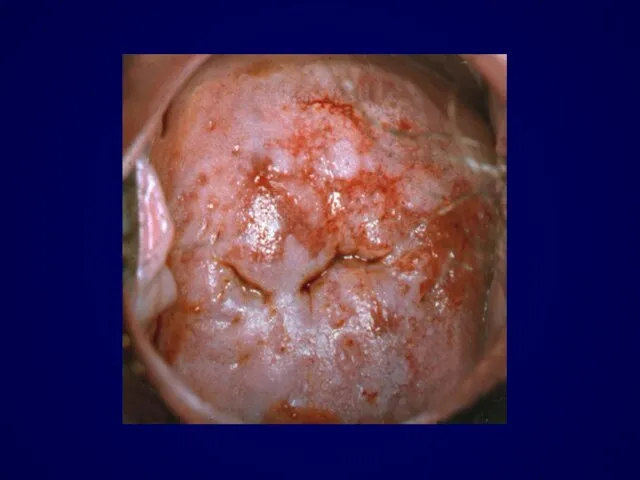
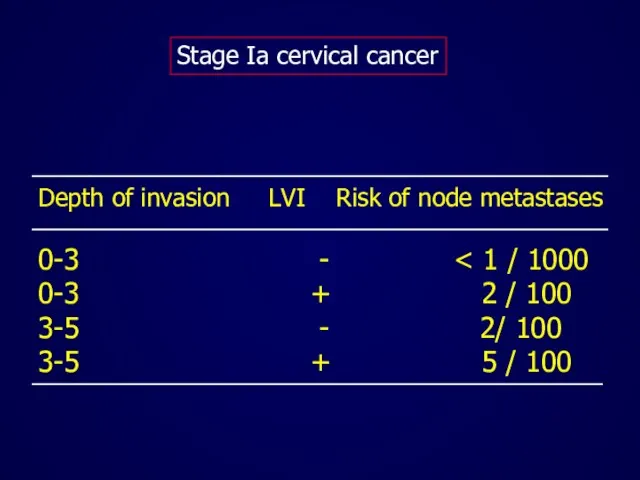
- 42. Microinvasive cervical cancer Stage I a
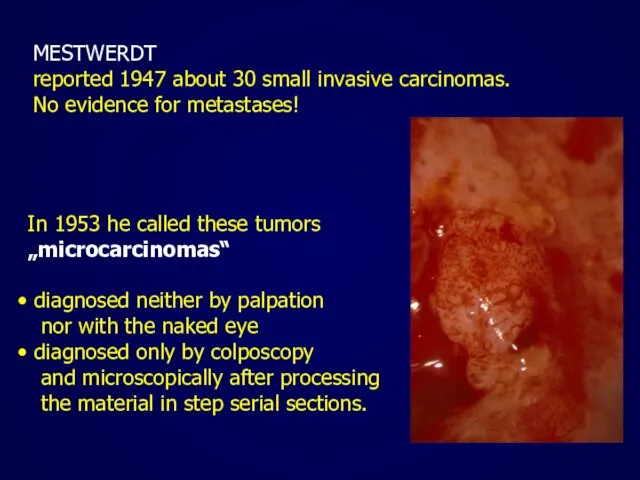
- 44. MESTWERDT reported 1947 about 30 small invasive carcinomas. No evidence for metastases! In 1953 he called
- 45. Stage l a 1: Measured stromal invasion of not > 3.0 mm in depth and extension
- 46. Were the microinvasive lesion and its preinvasive components removed in their entirety? What are the dimensions
- 47. The excision margins should be free of CIN and invasive disease !
- 48. If the invasive lesion is excised but CIN extends to the excision margin then a repeat
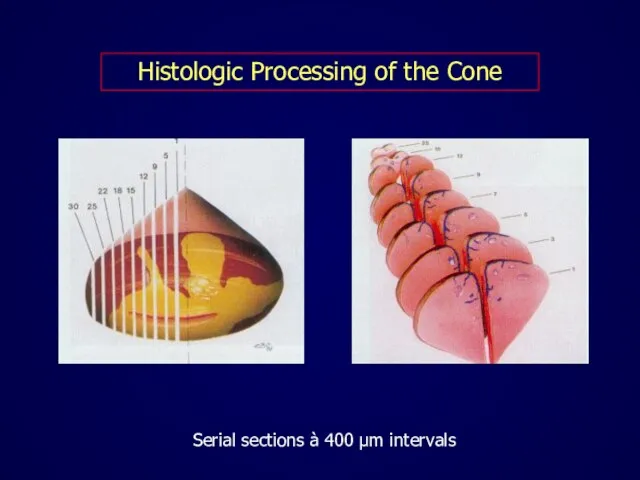
- 49. Histologic Processing of the Cone Serial sections à 400 μm intervals
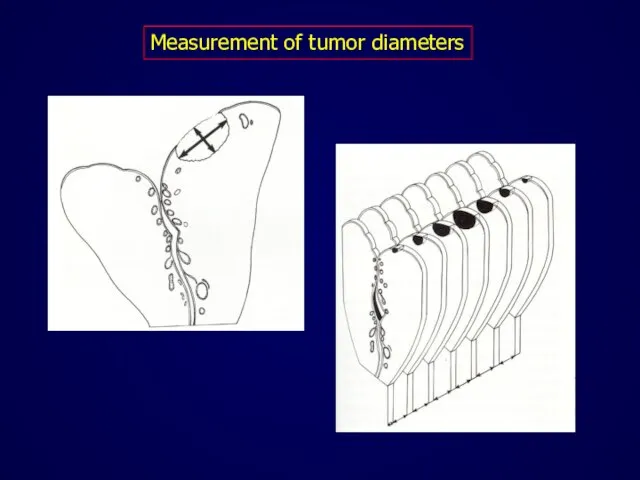
- 50. Measurement of tumor diameters
- 51. Ideally, the management of microinvasive cancer Stage Ia should be planned in cooperation with an experienced
- 52. Unfavourable prognostic criteria for microinvasive carcinoma include Deeper stromal invasion Capillary-like space involvement Poor differentiation Confluent
- 53. Depth of invasion LVI Risk of node metastases 0-3 - 0-3 + 2 / 100 3-5
- 54. Each patient with microinvasive cancer should be evaluated individually !
- 55. If distant spread is very unlikely, simple but complete excision of the lesion suffices. If it
- 56. The reasons of conservative surgery in microinvasive cervical cancer To preserve fertility To prevent the potential
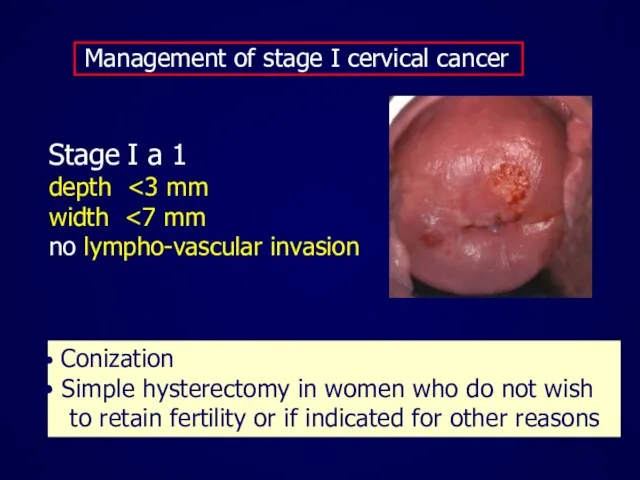
- 57. Management of stage I cervical cancer Stage I a 1 depth width no lympho-vascular invasion Conization
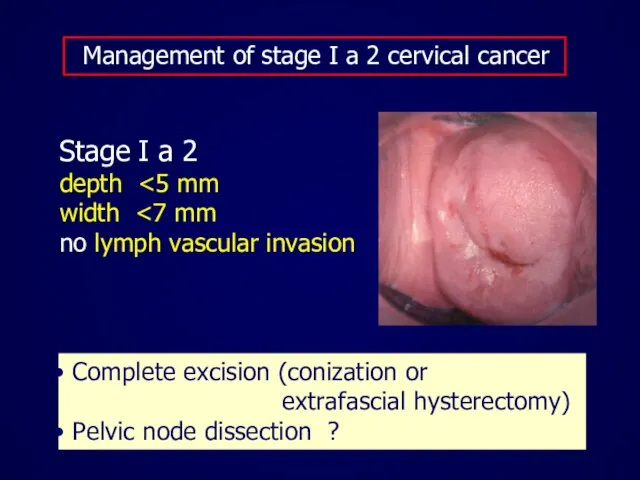
- 58. Management of stage I a 2 cervical cancer Stage I a 2 depth width no lymph
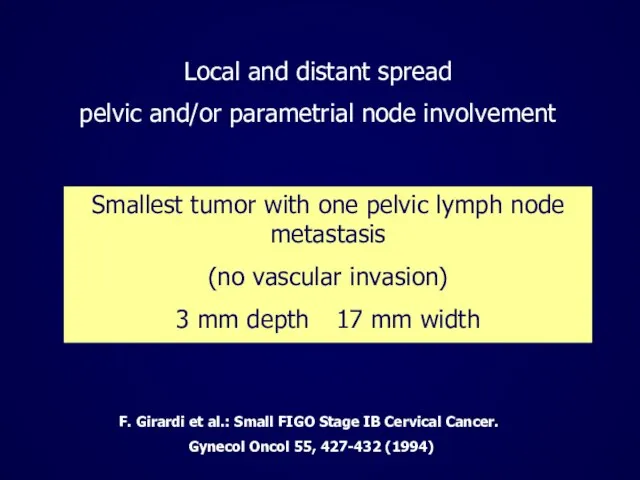
- 59. Smallest tumor with one pelvic lymph node metastasis (no vascular invasion) 3 mm depth 17 mm
- 61. Treatment options for stage I a with lympho-vasular invasion Modified radical hysterectomy (stage Ia1) or radical
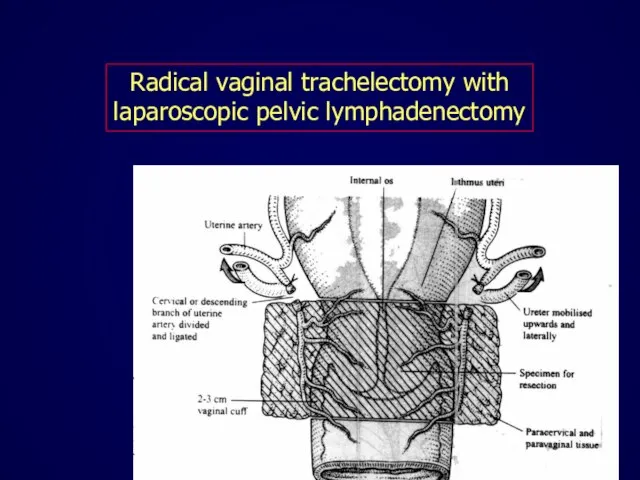
- 62. Radical vaginal trachelectomy with laparoscopic pelvic lymphadenectomy
- 63. Recurrence rates after trachelectomy are comparable to radical hysterectomy (aproximately 4%) Plante et al. Gynecol Oncol.
- 64. Radical trachelectomy Successful pregnancy in 26.5% cases Plante et al. Gynecol Oncol. 2004 ;94:614-23
- 65. Prerequisites for trachelectomy Strong fertility desire Patient Tumor No lymphovascular invasion Negative lymphnodes Favorable histology Length
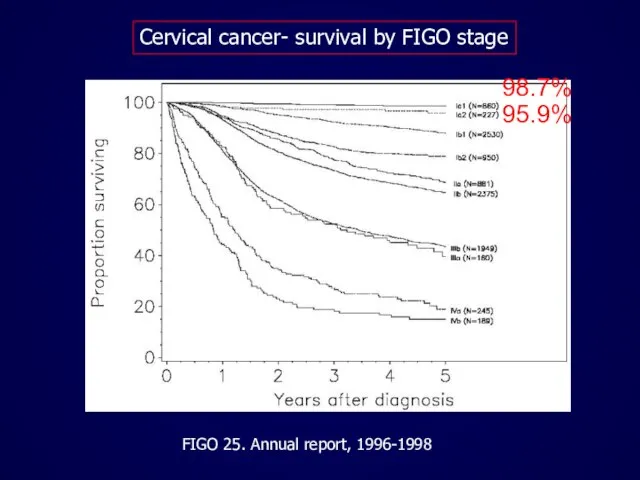
- 66. Cervical cancer- survival by FIGO stage FIGO 25. Annual report, 1996-1998 98.7% 95.9%
- 68. Скачать презентацию
Слайд 3Cervical cancer has become detectable
and curable disease.
Cervical cancer has become detectable
and curable disease.
Слайд 4Recently, however,
significant controversy
has arisen over several aspects of
the diagnosis and
Recently, however,
significant controversy
has arisen over several aspects of
the diagnosis and
Слайд 5There is no dispute about the need
to treat CIN 3
and few would
There is no dispute about the need
to treat CIN 3
and few would
Слайд 6These two grades of CIN (CIN 2 and CIN 3)
are referred
These two grades of CIN (CIN 2 and CIN 3)
are referred
Слайд 7In the spectrum of cervical pathology
the line between premalignant and benign lesions
may
In the spectrum of cervical pathology
the line between premalignant and benign lesions
may
Слайд 8L-SIL
High proportion of women affected
Low risk of progression
Significant regression
L-SIL
High proportion of women affected
Low risk of progression
Significant regression
Слайд 9Management of CIN 1 (L-SIL)
Conservative
Active
Management of CIN 1 (L-SIL)
Conservative
Active
Слайд 10Management of L-SIL
Close observation with cytologic
and possibly colposcopic follow-up,
without active
Management of L-SIL
Close observation with cytologic
and possibly colposcopic follow-up,
without active



Слайд 14Expectant management of CIN 1
is not totally without some risk...
Expectant management of CIN 1
is not totally without some risk...
Слайд 15……. because of the:
potential for a high-grade lesion
to develop
……. because of the:
potential for a high-grade lesion
to develop


Слайд 18If large lesions or persistent lesions
are present or if the patient
If large lesions or persistent lesions
are present or if the patient

Слайд 20Active management of women with CIN 1 is recommended in the following
Active management of women with CIN 1 is recommended in the following
Слайд 21Women with biopsy confirmed
H-SIL (CIN 2 and 3)
have significant risk
Women with biopsy confirmed
H-SIL (CIN 2 and 3)
have significant risk


Слайд 24The expectant management of CIN 2 and 3
with repeat cytology and
The expectant management of CIN 2 and 3
with repeat cytology and

Слайд 27Destruction or Excision ?
Destruction or Excision ?
Слайд 28Management of HSIL
excision recommended
cold-knife
laser conization
LLETZ
Management of HSIL
excision recommended
cold-knife
laser conization
LLETZ
Слайд 29 Excision is necessary in:
Unsatisfactory examination
Large lesions
Recurrent disease
Excision is necessary in:
Unsatisfactory examination
Large lesions
Recurrent disease


Слайд 33Unless there are other compelling
reasons for performing a hysterectomy,
this procedure
Unless there are other compelling
reasons for performing a hysterectomy,
this procedure
Слайд 34The finding of invasive cancer after treatment of CIN 3
Conization (n=237)
8.84%
Hysterectomy (n=106)
26.42%
Kesic
The finding of invasive cancer after treatment of CIN 3
Conization (n=237)
8.84%
Hysterectomy (n=106)
26.42%
Kesic



Слайд 39Vesna Kesic
Institute of Obstetrics and Gynecology
Clinical Center of Serbia
International Scientific Conference
Prevention of
Vesna Kesic
Institute of Obstetrics and Gynecology
Clinical Center of Serbia
International Scientific Conference
Prevention of

Слайд 40Treatment of cervical cancer is affected
by the stage of the disease.
Treatment of cervical cancer is affected
by the stage of the disease.
Слайд 41FIGO
Montreal,
1994
FIGO
Montreal,
1994
Слайд 42Microinvasive cervical cancer
Stage I a
Microinvasive cervical cancer
Stage I a
Слайд 44MESTWERDT
reported 1947 about 30 small invasive carcinomas.
No evidence for metastases!
In 1953
MESTWERDT
reported 1947 about 30 small invasive carcinomas.
No evidence for metastases!
In 1953
Слайд 45Stage l a 1:
Measured stromal invasion of not > 3.0 mm in
Stage l a 1:
Measured stromal invasion of not > 3.0 mm in
Слайд 46Were the microinvasive lesion and its
preinvasive components removed in their
entirety?
What are the
Were the microinvasive lesion and its
preinvasive components removed in their
entirety?
What are the
Слайд 47The excision margins should be free
of CIN and invasive disease !
The excision margins should be free
of CIN and invasive disease !
Слайд 48If the invasive lesion is excised
but CIN extends to the excision
If the invasive lesion is excised
but CIN extends to the excision
Слайд 49Histologic Processing of the Cone
Serial sections à 400 μm intervals
Histologic Processing of the Cone
Serial sections à 400 μm intervals
Слайд 50Measurement of tumor diameters
Measurement of tumor diameters
Слайд 51Ideally, the management of
microinvasive cancer Stage Ia
should be planned in
Ideally, the management of
microinvasive cancer Stage Ia
should be planned in
Слайд 52 Unfavourable prognostic criteria
for microinvasive carcinoma include
Deeper stromal invasion
Capillary-like
Unfavourable prognostic criteria
for microinvasive carcinoma include
Deeper stromal invasion
Capillary-like
Слайд 53
Depth of invasion LVI Risk of node metastases
0-3 - < 1
Depth of invasion LVI Risk of node metastases
0-3 - < 1
Слайд 54Each patient with microinvasive cancer
should be evaluated
individually !
Each patient with microinvasive cancer
should be evaluated
individually !
Слайд 55If distant spread is very unlikely,
simple but complete excision of the lesion
suffices.
If
If distant spread is very unlikely,
simple but complete excision of the lesion
suffices.
If
Слайд 56The reasons of conservative surgery in
microinvasive cervical cancer
To preserve fertility
To
The reasons of conservative surgery in
microinvasive cervical cancer
To preserve fertility
To
Слайд 57 Management of stage I cervical cancer
Stage I a 1
depth <3
Management of stage I cervical cancer
Stage I a 1
depth <3
Слайд 58 Management of stage I a 2 cervical cancer
Stage I a 2
Management of stage I a 2 cervical cancer
Stage I a 2
Слайд 59Smallest tumor with one pelvic lymph node metastasis
(no vascular invasion)
3
Smallest tumor with one pelvic lymph node metastasis
(no vascular invasion)
3

Слайд 61 Treatment options for stage I a
with lympho-vasular invasion
Modified radical
Treatment options for stage I a
with lympho-vasular invasion
Modified radical
Слайд 62Radical vaginal trachelectomy with
laparoscopic pelvic lymphadenectomy
Radical vaginal trachelectomy with
laparoscopic pelvic lymphadenectomy
Слайд 63Recurrence rates after trachelectomy
are comparable
to radical hysterectomy (aproximately 4%)
Plante et al.
Recurrence rates after trachelectomy
are comparable
to radical hysterectomy (aproximately 4%)
Plante et al.
Слайд 64 Radical trachelectomy
Successful pregnancy in 26.5% cases
Plante et al. Gynecol Oncol.
Radical trachelectomy
Successful pregnancy in 26.5% cases
Plante et al. Gynecol Oncol.
Слайд 65Prerequisites for trachelectomy
Strong fertility desire
Patient < 40 years
Tumor
Prerequisites for trachelectomy
Strong fertility desire
Patient < 40 years
Tumor
Слайд 66Cervical cancer- survival by FIGO stage
FIGO 25. Annual report, 1996-1998
98.7%
95.9%
Cervical cancer- survival by FIGO stage
FIGO 25. Annual report, 1996-1998
98.7%
95.9%
 Памятка для приезжающих в Ростовскую область из других регионов России
Памятка для приезжающих в Ростовскую область из других регионов России На примере Реабилитационного Центра «Новая Жизнь» (Ленинградская область, Россия) Докладчик: Алексей Фомичев
На примере Реабилитационного Центра «Новая Жизнь» (Ленинградская область, Россия) Докладчик: Алексей Фомичев Развитие побега из почки
Развитие побега из почки Тема 1.3. Меры таможенного контроля и их применение
Тема 1.3. Меры таможенного контроля и их применение Норри или камбоджийский бамбуковый поезд
Норри или камбоджийский бамбуковый поезд Собирающие линзы
Собирающие линзы Аппарат «Астер»
Аппарат «Астер» КРОВЬ И КРОВООБРАЩЕНИЕ
КРОВЬ И КРОВООБРАЩЕНИЕ «Использование информационно-коммуникационных технологий как ресурс активизации познавательного интереса обучающихся на урока
«Использование информационно-коммуникационных технологий как ресурс активизации познавательного интереса обучающихся на урока КОГДА ЛЮБОВЬ В ДЕФИЦИТЕ
КОГДА ЛЮБОВЬ В ДЕФИЦИТЕ Отчёт проверки герметичности контуров корпуса морозильного ларя BEST, сер №0771919032
Отчёт проверки герметичности контуров корпуса морозильного ларя BEST, сер №0771919032 The life of presidents and kings
The life of presidents and kings  Права ребёнка
Права ребёнка Bem-Aventurados os Aflitos Evangelho Segundo o Espiritismo Cap. V
Bem-Aventurados os Aflitos Evangelho Segundo o Espiritismo Cap. V Сера
Сера Причастия действительные и страдательные
Причастия действительные и страдательные Maynor_prezentatsia_1-2_chasti
Maynor_prezentatsia_1-2_chasti Модуль D1: Планирование рабочего процесса. Проект Теркин-club
Модуль D1: Планирование рабочего процесса. Проект Теркин-club Руководство
Руководство В9. Грамматическая основа
В9. Грамматическая основа Методы удаления волос. Рынок эпиляторов
Методы удаления волос. Рынок эпиляторов Антибиотики Грипп
Антибиотики Грипп Если не лениться , можно многого добиться
Если не лениться , можно многого добиться Нюрнбергский процесс
Нюрнбергский процесс Эффективность социальной рекламы
Эффективность социальной рекламы Прохождение военной службы по призыву
Прохождение военной службы по призыву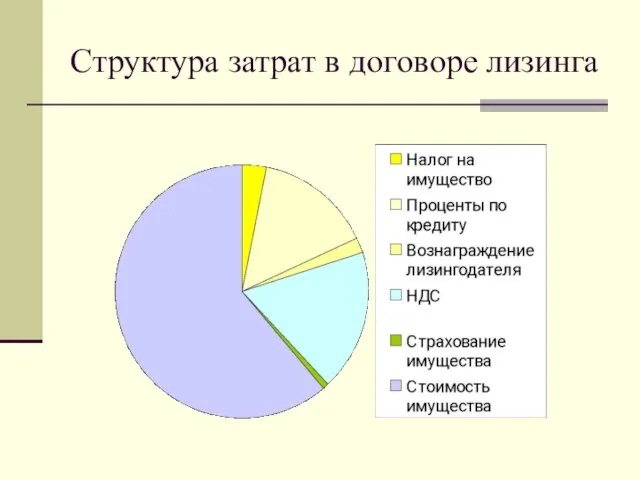 Структура затрат в договоре лизинга
Структура затрат в договоре лизинга Натюрморт из инструментов
Натюрморт из инструментов