- Mucocutaneous Diseases

Содержание
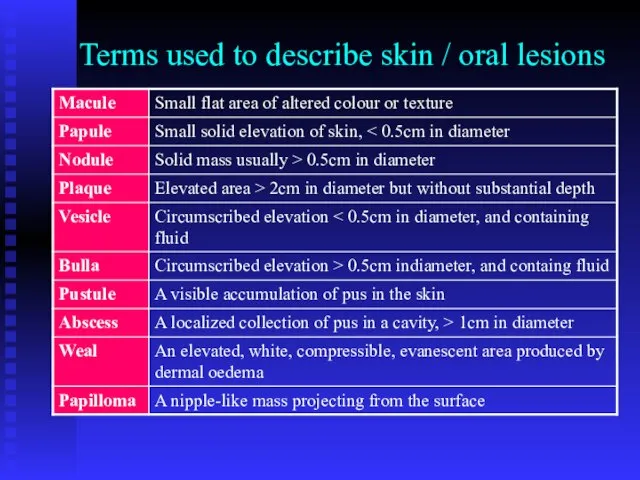
- 2. Terms used to describe skin / oral lesions
- 4. Lichen Planus Aetiology: not clear yet Viral aetiology (HPV-6, 11, 16, 18; HHV 6) Autoimmune disease
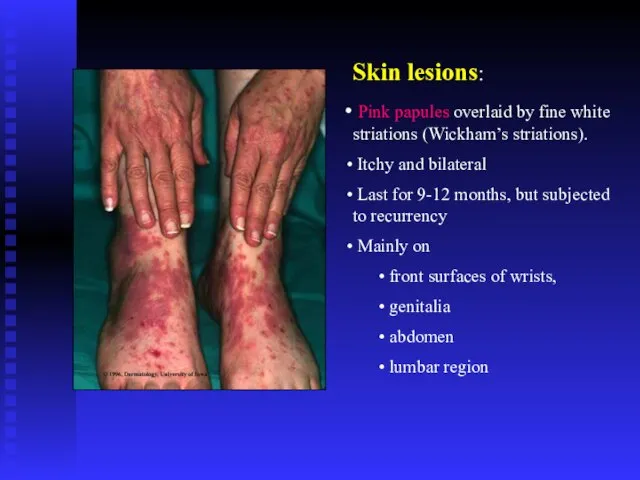
- 5. Skin lesions: Pink papules overlaid by fine white striations (Wickham’s striations). Itchy and bilateral Last for
- 6. Kobner phenomenon
- 7. Bilateral, itchy papules with scaly surface
- 8. Nail lesions: Vertical grooving and destruction of the nails (nails dystrophy).
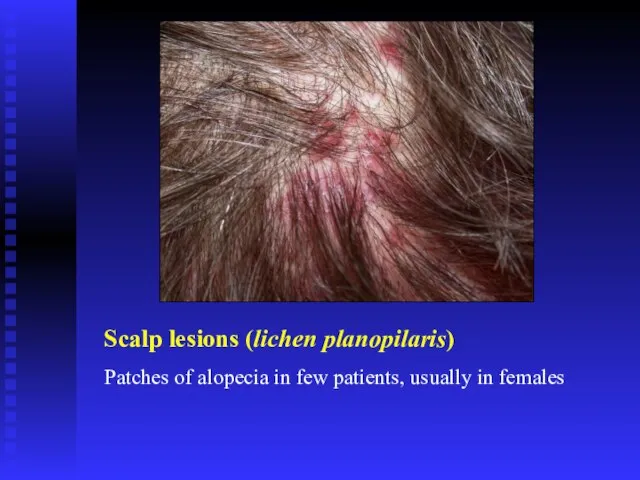
- 9. Scalp lesions (lichen planopilaris) Patches of alopecia in few patients, usually in females
- 10. Oral Lichen Planus Non-erosive Papular Linear Reticular Annular Plaque type Erosive Atrophic Bullous Ulcerative
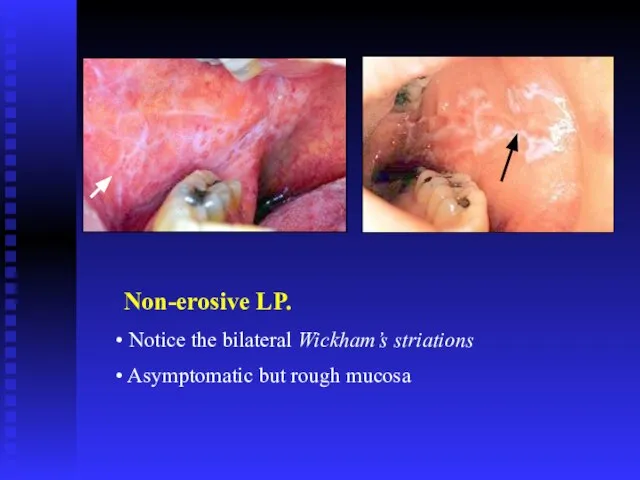
- 11. Non-erosive LP. Notice the bilateral Wickham’s striations Asymptomatic but rough mucosa
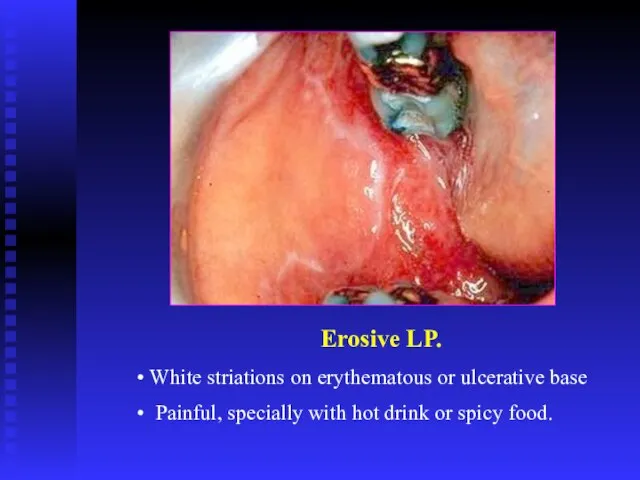
- 14. Erosive LP. White striations on erythematous or ulcerative base Painful, specially with hot drink or spicy
- 16. Non-erosive LP. Plaque type
- 17. Desquamative gingivitis on attached gingiva Is a clinical rather than a pathological entity
- 18. Ulcers
- 19. Oral Lichen Planus Diagnosis: Clinical picture Incisional biopsy DIF & IIF to exclude other diseases Prognosis:
- 20. Histopathology of LP. Epithelial hyperplasia or atrophy Saw teeth appearance of rete ridges Liquifaction degeneration of
- 22. Treatment of OLP Aims of treatment Resolution of oral painful symptoms Resolution of oral mucosal lesions
- 23. Treatment of OLP. Skin lesions Steroid cream Systemic steroids Oral lesions: Minor erosive type Remove trauma
- 24. Treatment of OLP. Oral lesions: Major erosive type High concentration steroid mouth wash Triamcinolone intra-lesional injections
- 25. ?Potentially malignant condition 0.4%-2% per five years observation
- 26. OLP – Patient’s follow up Follow up: Every month till resolution of symptoms Every 6-12 month
- 27. Lichenoid eruption The expression or unmasking of the lichen planus antigen may be induced by: Drugs
- 28. Lichenoid eruption Precipitated by: Non-steroidal anti-inflammatory Antihypertensive drugs (beta-blockers, ACE inhibitors) Oral hypoglycaemic agents (e.g. sulphonylurea)
- 29. Oral lichenoid lesions may be triggered by mechanical trauma (Koebner phenomenon) due to Calculus deposits Sharp
- 31. Pemphigus Auto-immune disease The patients usually between 40-60 years old Racial difference in incidence Most of
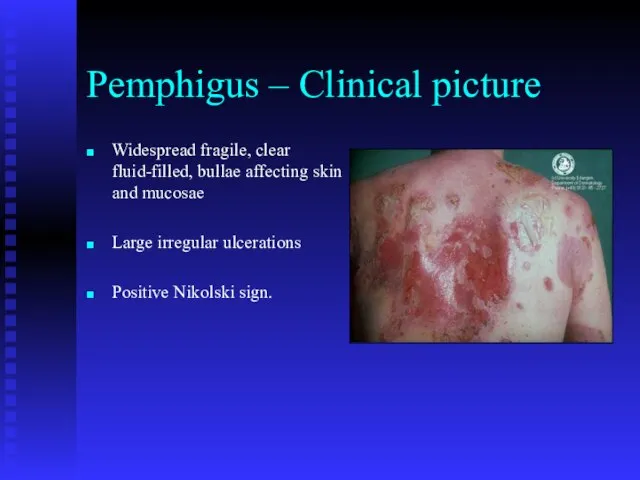
- 33. Pemphigus – Clinical picture Widespread fragile, clear fluid-filled, bullae affecting skin and mucosae Large irregular ulcerations
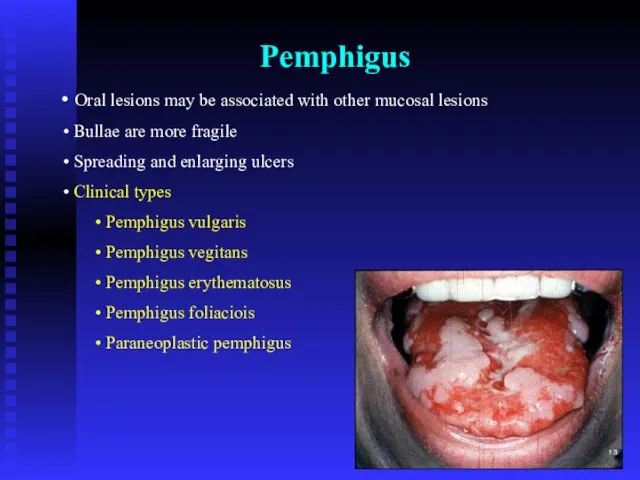
- 34. Pemphigus Oral lesions may be associated with other mucosal lesions Bullae are more fragile Spreading and
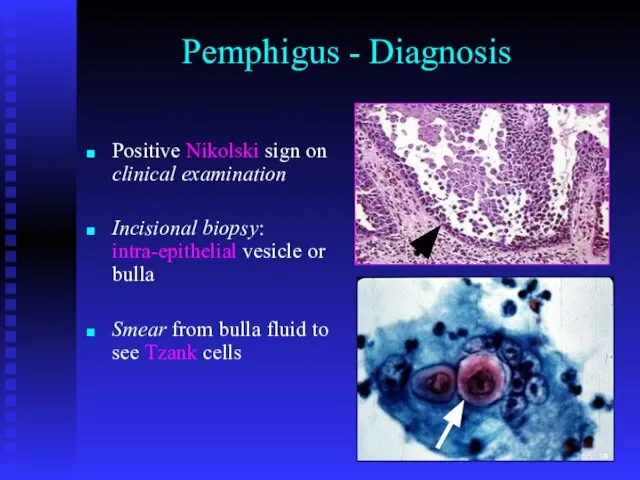
- 38. Pemphigus - Diagnosis Positive Nikolski sign on clinical examination Incisional biopsy: intra-epithelial vesicle or bulla Smear
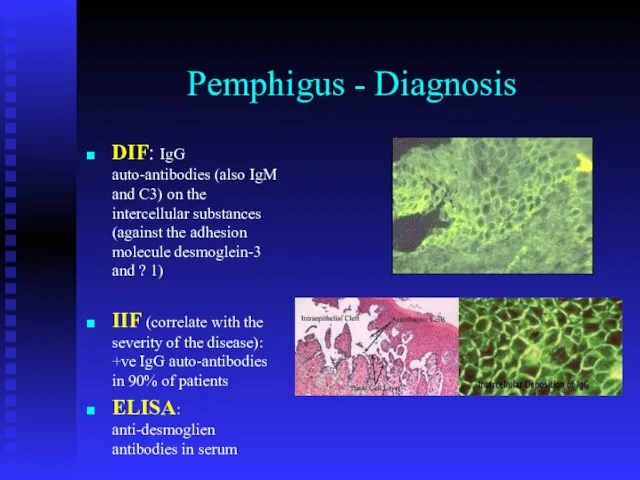
- 39. Pemphigus - Diagnosis DIF: IgG auto-antibodies (also IgM and C3) on the intercellular substances (against the
- 40. Direct & Indirect IF
- 41. Pemphigus - Treatment Multidisplinary Initial treatment with high doses of steroid (100mg prednisolone / day) Patients
- 42. Paraneoplastic pemphigus http://emedicine.medscape.com/article/1064452-overview Anhalt GJ, et al. Paraneoplastic pemphigus. An autoimmune mucocutaneous disease associated with neoplasia.
- 43. Mucosal lesions Oral Erosions and mucositis Resembling SJS Genital Nasal: epistaxis Skin lesions Diffuse erythema Vesiculobullous
- 44. Pemphigoid Auto-immune disease No racial predominance Two basic clinical types: Bullous (generalized) pemhigoid Mucousal (cicatricial) pemhigoid
- 45. Generalized (bullous) pemphigoid Patients > 60 yrs. Old No racial or gender predominance Skin: Starts as
- 46. Mucosal (cicatricial) pemphigoid Patients age: 50-70 yrs. M/F = ~ 1/4 Oral lesions Almost always present,
- 48. Mucosal pemphigoid - Diagnosis Incisional biopsy: sub-epithelial bulla DIF: on perilesional mucosa +ve in 75% of
- 49. Pemphigoid – Treatment This disorder is extremely difficult to treat. Even with optimum control, blisters may
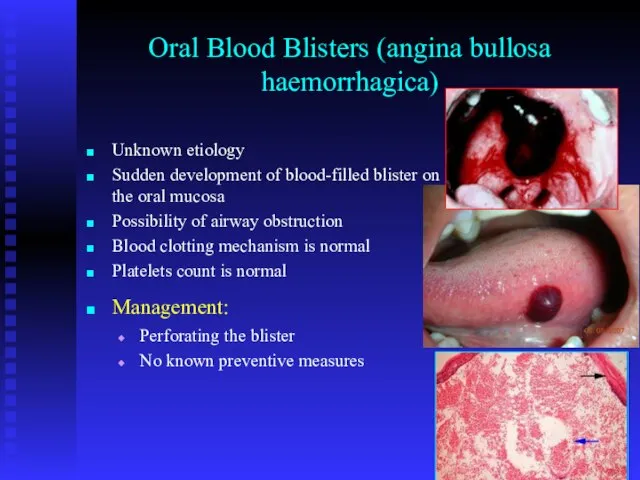
- 50. Oral Blood Blisters (angina bullosa haemorrhagica) Unknown etiology Sudden development of blood-filled blister on the oral
- 51. Erythema multiforme Precipitating factors: Type IV hypersensitivity reaction Viral infections (e.g herpes simplex, mycoplasma) Bacterial infections
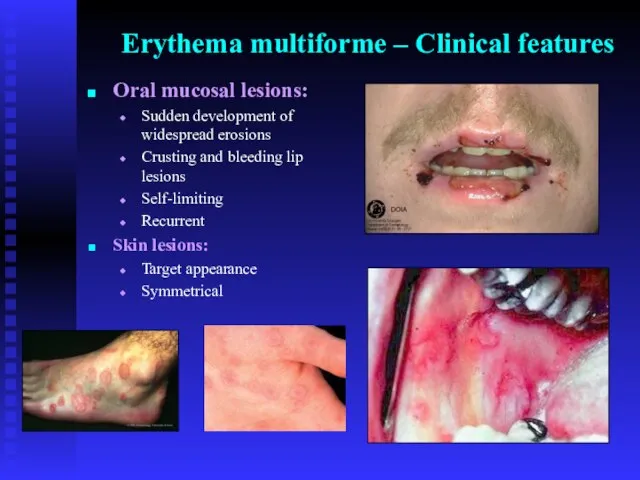
- 52. Erythema multiforme – Clinical features Oral mucosal lesions: Sudden development of widespread erosions Crusting and bleeding
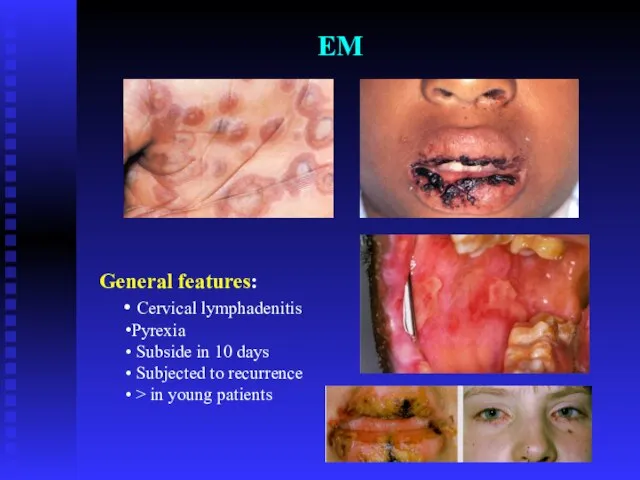
- 53. EM General features: Cervical lymphadenitis Pyrexia Subside in 10 days Subjected to recurrence > in young
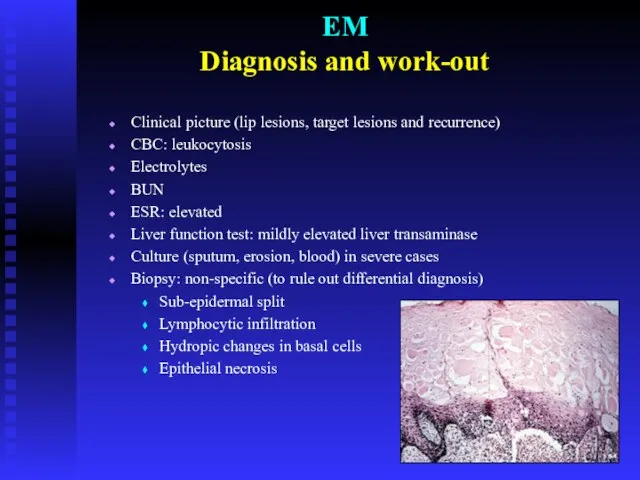
- 55. EM Diagnosis and work-out Clinical picture (lip lesions, target lesions and recurrence) CBC: leukocytosis Electrolytes BUN
- 56. EM Treatment - Management Remove the cause if possible Treat infections Fluid intake and soft diet;
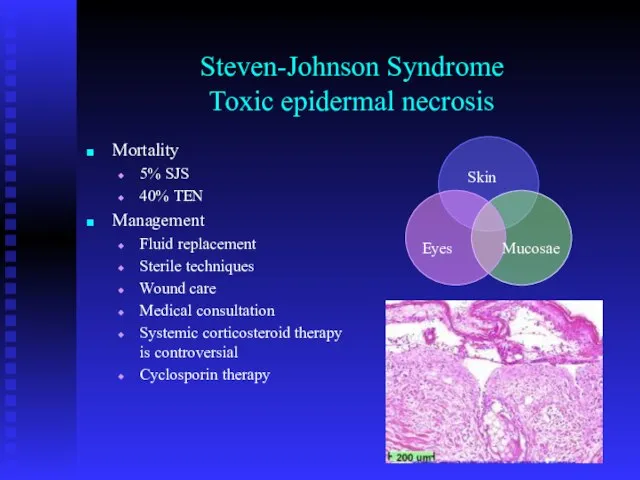
- 57. Steven-Johnson Syndrome Toxic epidermal necrosis Mortality 5% SJS 40% TEN Management Fluid replacement Sterile techniques Wound
- 59. Lupus Erythematosus Autoimmune disease Two main clinical divisions: Discoid lupus erythematosus (DLE) Systemic lupus erythematosus (SLE)
- 60. Lupus Erythematosus – Clinical Features SLE: Skin: erythematous itchy rash (butter fly appearance) Systemic manifestations: arthritis,
- 61. DLE: mainly cutaneous lesions Skin: resemble SLE, symmetrical, heals with scaring Mucosa: superficial erosions and erythematous
- 62. Lupus Erythematosus Diagnosis: IMF: antinuclear antibodies (ANA) +ve in 90% of patients. DMF Biopsy and histopathological
- 63. Prognosis No cure Renal disease is the main morbidity and mortality Thrombocytopenia and hemolytic anemia in
- 65. Скачать презентацию
Слайд 4Lichen Planus
Aetiology: not clear yet
Viral aetiology (HPV-6, 11, 16, 18; HHV 6)
Autoimmune
Lichen Planus
Aetiology: not clear yet
Viral aetiology (HPV-6, 11, 16, 18; HHV 6)
Autoimmune
Слайд 5Skin lesions:
Pink papules overlaid by fine white striations (Wickham’s striations).
Itchy
Skin lesions:
Pink papules overlaid by fine white striations (Wickham’s striations).
Itchy
Слайд 6Kobner phenomenon
Kobner phenomenon

Слайд 7Bilateral, itchy papules with scaly surface
Bilateral, itchy papules with scaly surface

Слайд 8Nail lesions:
Vertical grooving and destruction of the nails (nails dystrophy).
Nail lesions:
Vertical grooving and destruction of the nails (nails dystrophy).

Слайд 9Scalp lesions (lichen planopilaris)
Patches of alopecia in few patients, usually in females
Scalp lesions (lichen planopilaris)
Patches of alopecia in few patients, usually in females
Слайд 10Oral Lichen Planus
Non-erosive
Papular
Linear
Reticular
Annular
Plaque type
Erosive
Atrophic
Bullous
Ulcerative
Oral Lichen Planus
Non-erosive
Papular
Linear
Reticular
Annular
Plaque type
Erosive
Atrophic
Bullous
Ulcerative
Слайд 11Non-erosive LP.
Notice the bilateral Wickham’s striations
Asymptomatic but rough mucosa
Non-erosive LP.
Notice the bilateral Wickham’s striations
Asymptomatic but rough mucosa


Слайд 14Erosive LP.
White striations on erythematous or ulcerative base
Painful, specially with
Erosive LP.
White striations on erythematous or ulcerative base
Painful, specially with

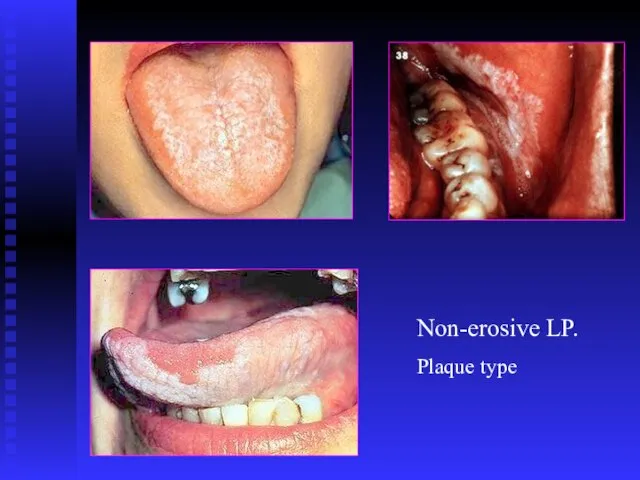
Слайд 16Non-erosive LP.
Plaque type
Non-erosive LP.
Plaque type
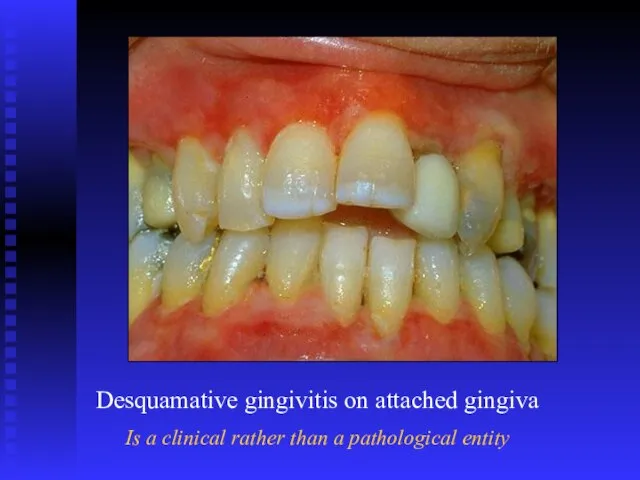
Слайд 17Desquamative gingivitis on attached gingiva
Is a clinical rather than a pathological entity
Desquamative gingivitis on attached gingiva
Is a clinical rather than a pathological entity
Слайд 18Ulcers
Ulcers

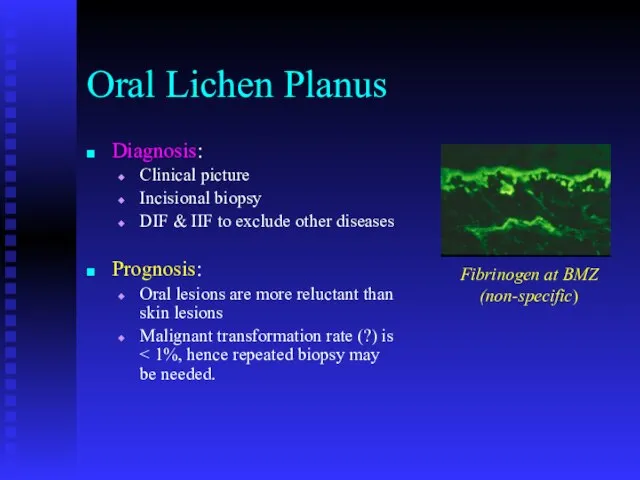
Слайд 19Oral Lichen Planus
Diagnosis:
Clinical picture
Incisional biopsy
DIF & IIF to exclude other diseases
Prognosis:
Oral lesions
Oral Lichen Planus
Diagnosis:
Clinical picture
Incisional biopsy
DIF & IIF to exclude other diseases
Prognosis:
Oral lesions
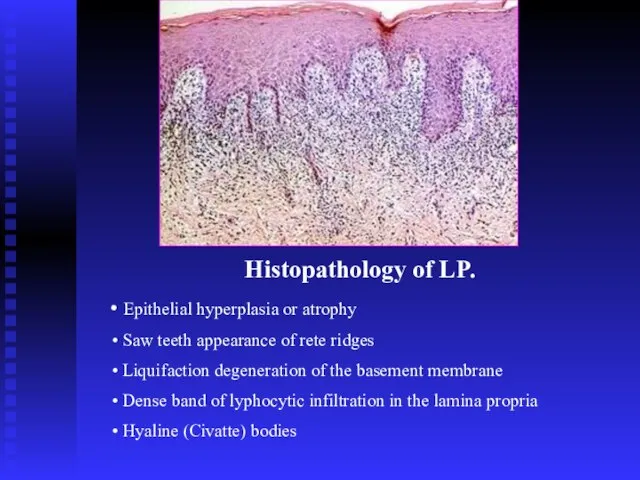
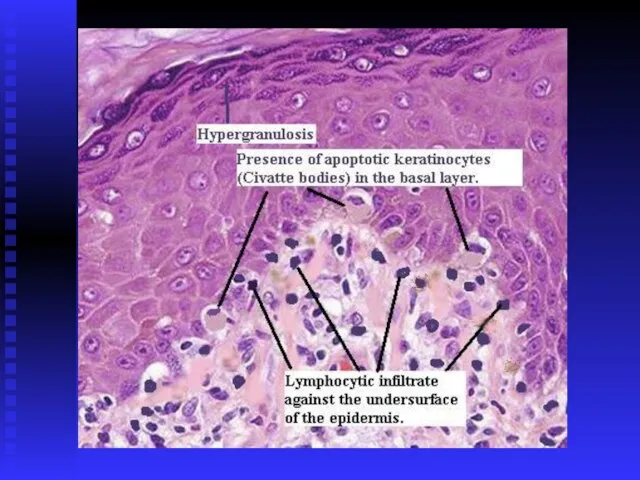
Слайд 20Histopathology of LP.
Epithelial hyperplasia or atrophy
Saw teeth appearance of rete
Histopathology of LP.
Epithelial hyperplasia or atrophy
Saw teeth appearance of rete
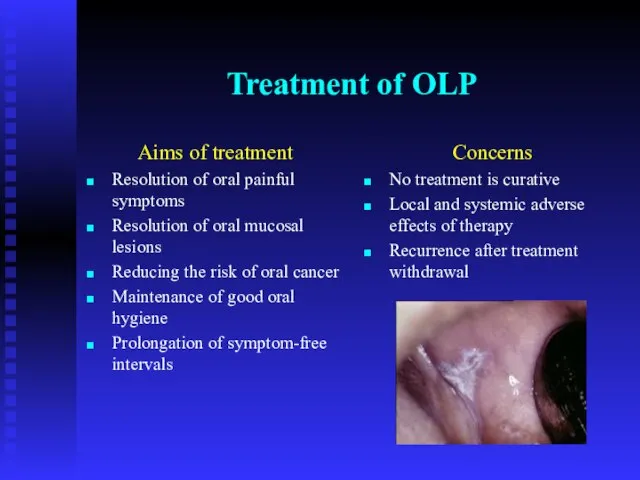
Слайд 22Treatment of OLP
Aims of treatment
Resolution of oral painful symptoms
Resolution of oral mucosal
Treatment of OLP
Aims of treatment
Resolution of oral painful symptoms
Resolution of oral mucosal
Слайд 23Treatment of OLP.
Skin lesions
Steroid cream
Systemic steroids
Oral lesions: Minor erosive type
Remove trauma
Antiseptic mouth
Treatment of OLP.
Skin lesions
Steroid cream
Systemic steroids
Oral lesions: Minor erosive type
Remove trauma
Antiseptic mouth
Слайд 24Treatment of OLP.
Oral lesions: Major erosive type
High concentration steroid mouth wash
Triamcinolone intra-lesional
Treatment of OLP.
Oral lesions: Major erosive type
High concentration steroid mouth wash
Triamcinolone intra-lesional
Слайд 25?Potentially malignant condition
0.4%-2% per five years observation
?Potentially malignant condition
0.4%-2% per five years observation
Слайд 26OLP – Patient’s follow up
Follow up:
Every month till resolution of symptoms
Every 6-12
OLP – Patient’s follow up
Follow up:
Every month till resolution of symptoms
Every 6-12
Слайд 27Lichenoid eruption
The expression or unmasking of the lichen planus antigen may be
Lichenoid eruption
The expression or unmasking of the lichen planus antigen may be
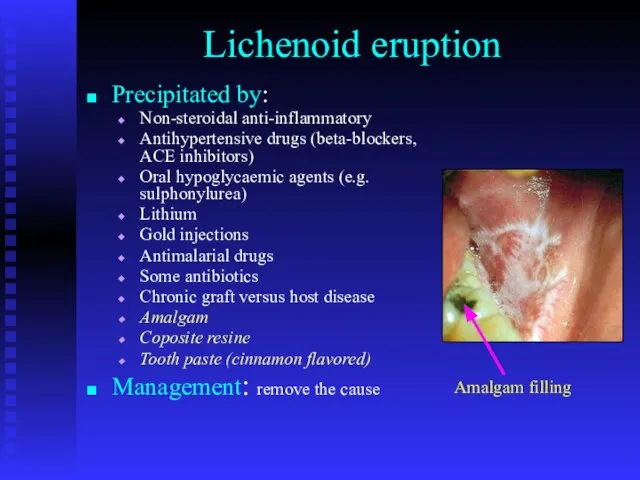
Слайд 28Lichenoid eruption
Precipitated by:
Non-steroidal anti-inflammatory
Antihypertensive drugs (beta-blockers, ACE inhibitors)
Oral hypoglycaemic agents (e.g. sulphonylurea)
Lithium
Gold
Lichenoid eruption
Precipitated by:
Non-steroidal anti-inflammatory
Antihypertensive drugs (beta-blockers, ACE inhibitors)
Oral hypoglycaemic agents (e.g. sulphonylurea)
Lithium
Gold
Слайд 29Oral lichenoid lesions may be triggered by mechanical trauma (Koebner phenomenon) due
Oral lichenoid lesions may be triggered by mechanical trauma (Koebner phenomenon) due

Слайд 31Pemphigus
Auto-immune disease
The patients usually between 40-60 years old
Racial difference in incidence
Most of
Pemphigus
Auto-immune disease
The patients usually between 40-60 years old
Racial difference in incidence
Most of
Слайд 33Pemphigus – Clinical picture
Widespread fragile, clear fluid-filled, bullae affecting skin and mucosae
Large
Pemphigus – Clinical picture
Widespread fragile, clear fluid-filled, bullae affecting skin and mucosae
Large
Слайд 34Pemphigus
Oral lesions may be associated with other mucosal lesions
Bullae are
Pemphigus
Oral lesions may be associated with other mucosal lesions
Bullae are



Слайд 38Pemphigus - Diagnosis
Positive Nikolski sign on clinical examination
Incisional biopsy: intra-epithelial vesicle or
Pemphigus - Diagnosis
Positive Nikolski sign on clinical examination
Incisional biopsy: intra-epithelial vesicle or
Слайд 39Pemphigus - Diagnosis
DIF: IgG auto-antibodies (also IgM and C3) on the intercellular
Pemphigus - Diagnosis
DIF: IgG auto-antibodies (also IgM and C3) on the intercellular
Слайд 40Direct & Indirect IF
Direct & Indirect IF
Слайд 41Pemphigus - Treatment
Multidisplinary
Initial treatment with high doses of steroid (100mg prednisolone /
Pemphigus - Treatment
Multidisplinary
Initial treatment with high doses of steroid (100mg prednisolone /
Слайд 42Paraneoplastic pemphigus
http://emedicine.medscape.com/article/1064452-overview
Anhalt GJ, et al. Paraneoplastic pemphigus. An autoimmune mucocutaneous disease associated with
Paraneoplastic pemphigus
http://emedicine.medscape.com/article/1064452-overview
Anhalt GJ, et al. Paraneoplastic pemphigus. An autoimmune mucocutaneous disease associated with
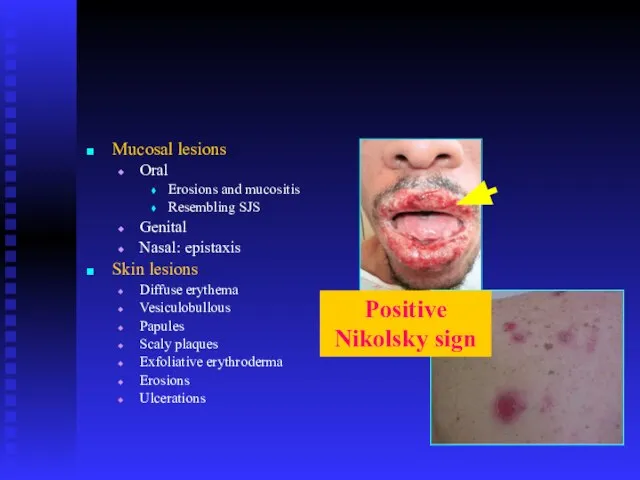
Слайд 43Mucosal lesions
Oral
Erosions and mucositis
Resembling SJS
Genital
Nasal: epistaxis
Skin lesions
Diffuse erythema
Vesiculobullous
Papules
Scaly plaques
Exfoliative erythroderma
Erosions
Ulcerations
Positive Nikolsky
Mucosal lesions
Oral
Erosions and mucositis
Resembling SJS
Genital
Nasal: epistaxis
Skin lesions
Diffuse erythema
Vesiculobullous
Papules
Scaly plaques
Exfoliative erythroderma
Erosions
Ulcerations
Positive Nikolsky
Слайд 44Pemphigoid
Auto-immune disease
No racial predominance
Two basic clinical types:
Bullous (generalized) pemhigoid
Mucousal (cicatricial) pemhigoid
Pemphigoid
Auto-immune disease
No racial predominance
Two basic clinical types:
Bullous (generalized) pemhigoid
Mucousal (cicatricial) pemhigoid
Слайд 45Generalized (bullous) pemphigoid
Patients > 60 yrs. Old
No racial or gender predominance
Skin:
Starts
Generalized (bullous) pemphigoid
Patients > 60 yrs. Old
No racial or gender predominance
Skin:
Starts
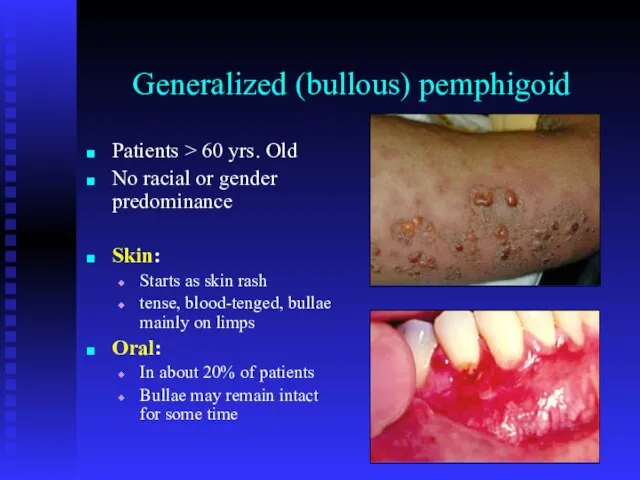
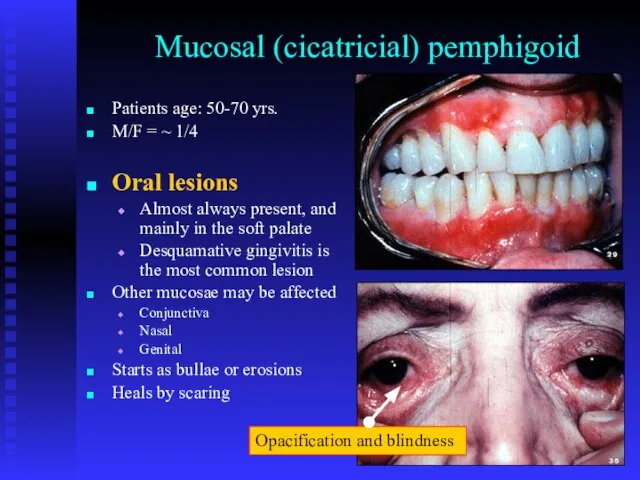
Слайд 46Mucosal (cicatricial) pemphigoid
Patients age: 50-70 yrs.
M/F = ~ 1/4
Oral lesions
Almost always
Mucosal (cicatricial) pemphigoid
Patients age: 50-70 yrs.
M/F = ~ 1/4
Oral lesions
Almost always

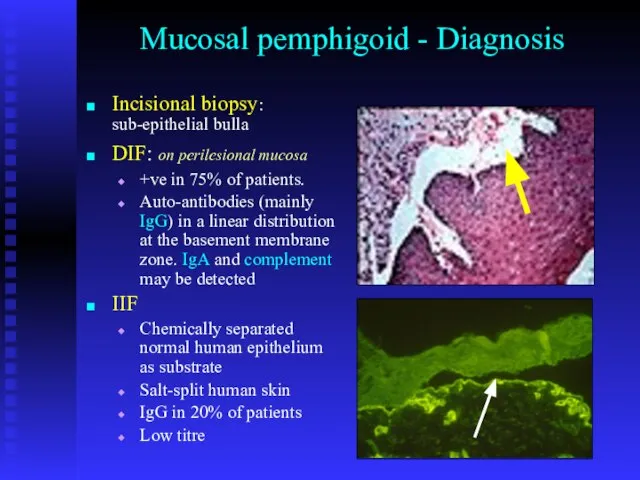
Слайд 48Mucosal pemphigoid - Diagnosis
Incisional biopsy: sub-epithelial bulla
DIF: on perilesional mucosa
+ve in 75%
Mucosal pemphigoid - Diagnosis
Incisional biopsy: sub-epithelial bulla
DIF: on perilesional mucosa
+ve in 75%
Слайд 49Pemphigoid – Treatment
This disorder is extremely difficult to treat. Even with optimum
Pemphigoid – Treatment This disorder is extremely difficult to treat. Even with optimum
Слайд 50Oral Blood Blisters (angina bullosa haemorrhagica)
Unknown etiology
Sudden development of blood-filled blister on
Oral Blood Blisters (angina bullosa haemorrhagica)
Unknown etiology
Sudden development of blood-filled blister on
Слайд 51Erythema multiforme
Precipitating factors: Type IV hypersensitivity reaction
Viral infections (e.g herpes simplex, mycoplasma)
Bacterial
Erythema multiforme
Precipitating factors: Type IV hypersensitivity reaction
Viral infections (e.g herpes simplex, mycoplasma)
Bacterial
Слайд 52Erythema multiforme – Clinical features
Oral mucosal lesions:
Sudden development of widespread erosions
Crusting
Erythema multiforme – Clinical features
Oral mucosal lesions:
Sudden development of widespread erosions
Crusting
Слайд 53EM
General features:
Cervical lymphadenitis
Pyrexia
Subside in 10 days
Subjected to recurrence
>
EM
General features:
Cervical lymphadenitis
Pyrexia
Subside in 10 days
Subjected to recurrence
>

Слайд 55EM
Diagnosis and work-out
Clinical picture (lip lesions, target lesions and recurrence)
CBC: leukocytosis
Electrolytes
BUN
ESR: elevated
Liver
EM
Diagnosis and work-out
Clinical picture (lip lesions, target lesions and recurrence)
CBC: leukocytosis
Electrolytes
BUN
ESR: elevated
Liver
Слайд 56EM
Treatment - Management
Remove the cause if possible
Treat infections
Fluid intake and soft diet;
EM
Treatment - Management
Remove the cause if possible
Treat infections
Fluid intake and soft diet;
Слайд 57Steven-Johnson Syndrome
Toxic epidermal necrosis
Mortality
5% SJS
40% TEN
Management
Fluid replacement
Sterile techniques
Wound care
Medical consultation
Systemic corticosteroid therapy
Steven-Johnson Syndrome
Toxic epidermal necrosis
Mortality
5% SJS
40% TEN
Management
Fluid replacement
Sterile techniques
Wound care
Medical consultation
Systemic corticosteroid therapy

Слайд 59Lupus Erythematosus
Autoimmune disease
Two main clinical divisions:
Discoid lupus erythematosus (DLE)
Systemic lupus erythematosus (SLE)
M:F
Lupus Erythematosus
Autoimmune disease
Two main clinical divisions:
Discoid lupus erythematosus (DLE)
Systemic lupus erythematosus (SLE)
M:F
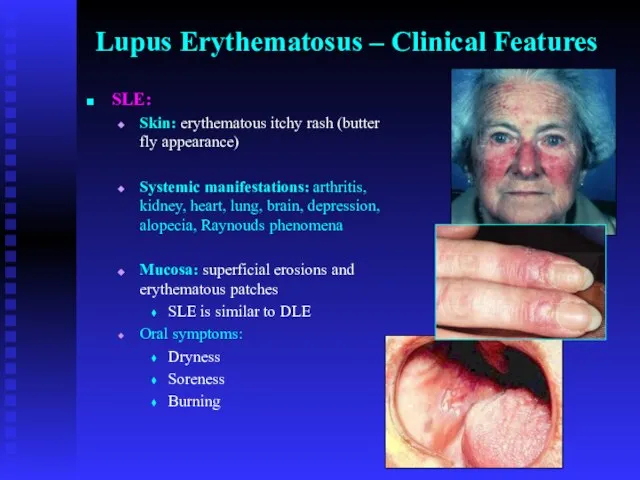
Слайд 60Lupus Erythematosus – Clinical Features
SLE:
Skin: erythematous itchy rash (butter fly appearance)
Systemic manifestations:
Lupus Erythematosus – Clinical Features
SLE:
Skin: erythematous itchy rash (butter fly appearance)
Systemic manifestations:
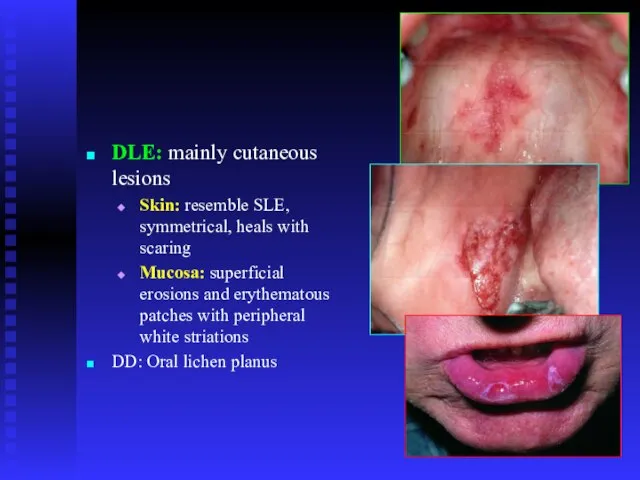
Слайд 61DLE: mainly cutaneous lesions
Skin: resemble SLE, symmetrical, heals with scaring
Mucosa: superficial erosions
DLE: mainly cutaneous lesions
Skin: resemble SLE, symmetrical, heals with scaring
Mucosa: superficial erosions
Слайд 62Lupus Erythematosus
Diagnosis:
IMF: antinuclear antibodies (ANA) +ve in 90% of patients.
DMF
Biopsy and histopathological
Lupus Erythematosus
Diagnosis:
IMF: antinuclear antibodies (ANA) +ve in 90% of patients.
DMF
Biopsy and histopathological
Слайд 63Prognosis
No cure
Renal disease is the main morbidity and mortality
Thrombocytopenia and hemolytic anemia
Prognosis
No cure
Renal disease is the main morbidity and mortality
Thrombocytopenia and hemolytic anemia
 Интеллект
Интеллект  цветой круг
цветой круг Бухгалтерский учет. Источники образования хозяйственных средств
Бухгалтерский учет. Источники образования хозяйственных средств Здоровьесбережение
Здоровьесбережение Презентация на тему Огонь ошибок не прощает
Презентация на тему Огонь ошибок не прощает 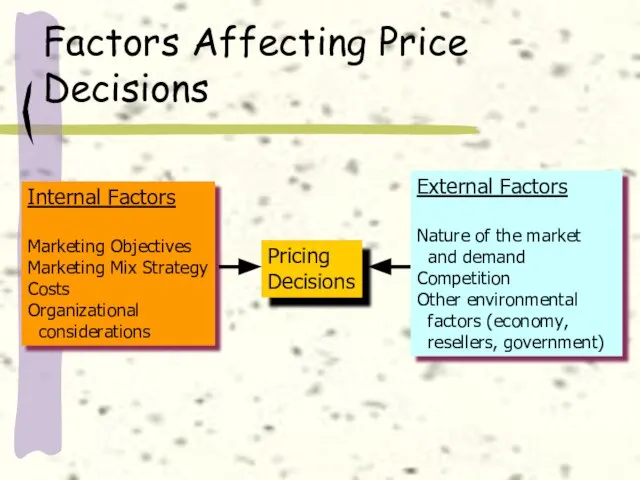 Factors affecting Price
Factors affecting Price Отчет главы городского округа- города Рассказово А.Н.Колмакова о результатах своей деятельности и деятельности администрации гор
Отчет главы городского округа- города Рассказово А.Н.Колмакова о результатах своей деятельности и деятельности администрации гор Детские писатели
Детские писатели Установка XP Professional
Установка XP Professional Презентация на тему Автограф
Презентация на тему Автограф  Урок физики в 9 классе
Урок физики в 9 классе Царства живой природы
Царства живой природы Мировой и российский рынки People as the Platform
Мировой и российский рынки People as the Platform ЭДИСОН ДЕНИСОВ
ЭДИСОН ДЕНИСОВ  ЖК Три Квартала
ЖК Три Квартала История о том, как «планета заболела»
История о том, как «планета заболела» Питание животных
Питание животных Многофункциональное устройство
Многофункциональное устройство Презентация на тему My house (3 класс)
Презентация на тему My house (3 класс) Аутсорсинг в секторе государственных услуг
Аутсорсинг в секторе государственных услуг Специальность: Страховое дело
Специальность: Страховое дело Президент США. Порядок избрания. Полномочия и акты
Президент США. Порядок избрания. Полномочия и акты ABLOY® CONTROL+
ABLOY® CONTROL+ Схема распределения грантов городам-участникам программы Тасис (TCAS) Экологические гранты для муниципалитетов
Схема распределения грантов городам-участникам программы Тасис (TCAS) Экологические гранты для муниципалитетов Презентация на тему Культура и духовная жизнь общества
Презентация на тему Культура и духовная жизнь общества Сечение поверхностей плоскостью. Тело с вырезом
Сечение поверхностей плоскостью. Тело с вырезом Кюри
Кюри Презентация на тему Веселая математическая игра
Презентация на тему Веселая математическая игра