- RENAL DISEASE

Содержание
- 2. Acute glomerulonephritis Acute GN is characterized by the abrupt onset of hematuria and proteinuria, often accompanied
- 3. Etiology Infectious Streptococcal Nonstreptococcal postinfectious glomerulonephritis Bacterial Viral Parasitic Noninfectious Multisystem systemic diseases Primary glomerular diseases
- 4. Pathogenesis Previously M-protein of the organism was felt to be responsible for PSGN. Recently, nephritis-associated streptococcal
- 5. Pathology Diffuse endocapillary proliferative changes are found. In postinfectious GN, the glomerulus is hypercellular with marked
- 6. Clinical Manifestations edemas, decreased volume and frequency of urination, systemic hypertension, uremic symptoms, costovertebral tenderness, gross
- 7. Clinical syndromes urinary (haematuria, proteinuria), nephritic (edemas, hypertension, gross haematuria, proteinuria), nephrotic (edemas, proteinuria, hypoproteinemia, hypercholesterolemia),
- 8. Workup Lab Studies: Urinalysis Blood, urea, and nitrogen (BUN); serum creatinine; and serum electrolytes (especially serum
- 9. Imaging Studies: Abdominal ultrasound Assesses renal size Assesses echogenicity of renal cortex Excludes obstruction
- 10. Histologic Findings: Generally, a renal biopsy is not necessary for diagnosis of acute PSGN; however, in
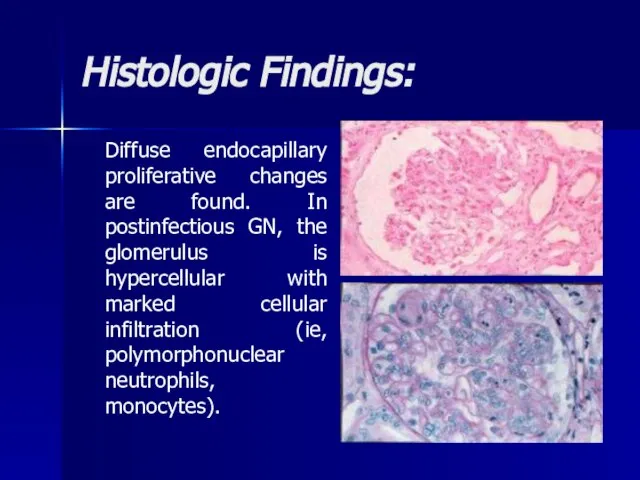
- 11. Histologic Findings: Diffuse endocapillary proliferative changes are found. In postinfectious GN, the glomerulus is hypercellular with
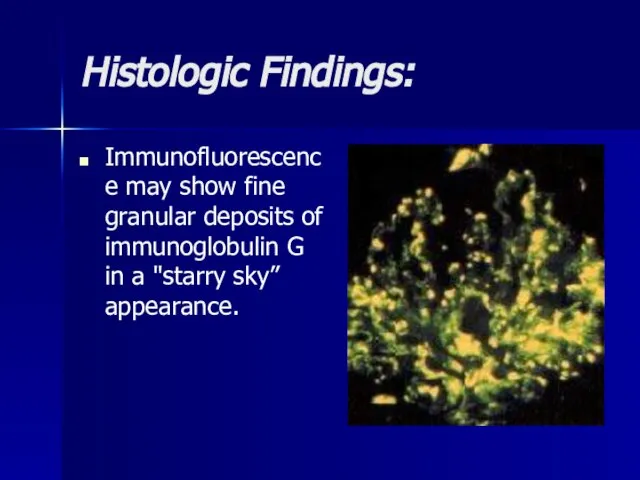
- 12. Histologic Findings: Immunofluorescence may show fine granular deposits of immunoglobulin G in a "starry sky” appearance.
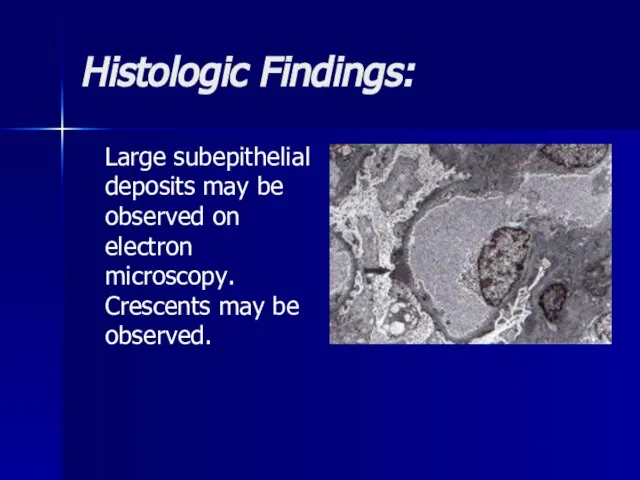
- 13. Histologic Findings: Large subepithelial deposits may be observed on electron microscopy. Crescents may be observed.
- 14. Differentials Crescentic Glomerulonephritis, Crescentic Glomerulonephritis, Diffuse Proliferative Glomerulonephritis, Crescentic Glomerulonephritis, Diffuse Proliferative Glomerulonephritis, Membranoproliferative Glomerulonephritis, Crescentic
- 15. Treatment Treat the underlying infections when acute GN is associated with chronic infections. Antimicrobial therapy Antibiotics
- 16. Prognosis Prognosis of acute PSGN is generally excellent in children. Within a week or so of
- 17. Chronic glomerulonephritis The condition is characterized by irreversible and progressive glomerular and tubulointerstitial fibrosis, ultimately leading
- 18. Etiology Nearly all forms of acute glomerulonephritis have a tendency to progress to chronic glomerulonephritis. The
- 19. Pathogenesis Reduction in nephron mass from the initial injury reduces the GFR. This reduction leads to
- 20. Histologic Findings In early stages, the glomeruli may still show some evidence of the primary disease.
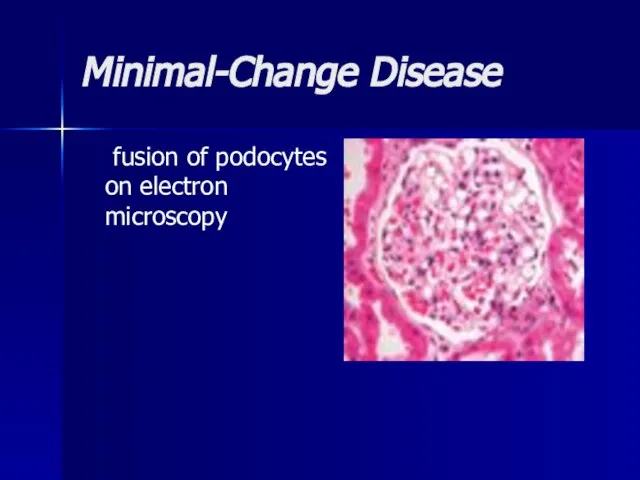
- 21. Minimal-Change Disease fusion of podocytes on electron microscopy
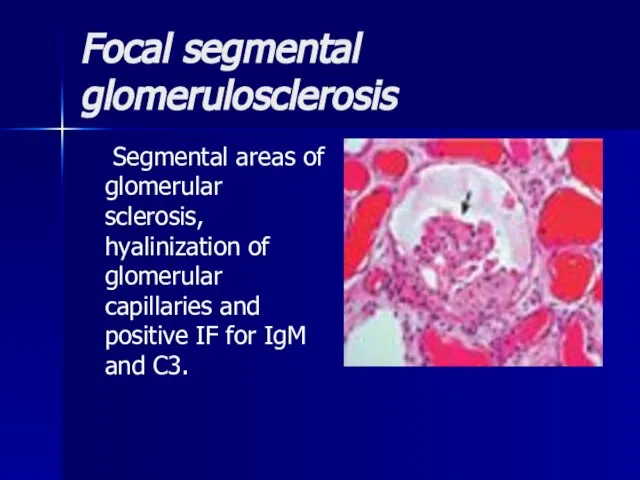
- 22. Focal segmental glomerulosclerosis Segmental areas of glomerular sclerosis, hyalinization of glomerular capillaries and positive IF for
- 23. Mesangiocapillary GN large glomeruli with mesangial proliferation and ‘double’ BM. 2 histological types: type I (subendothelial
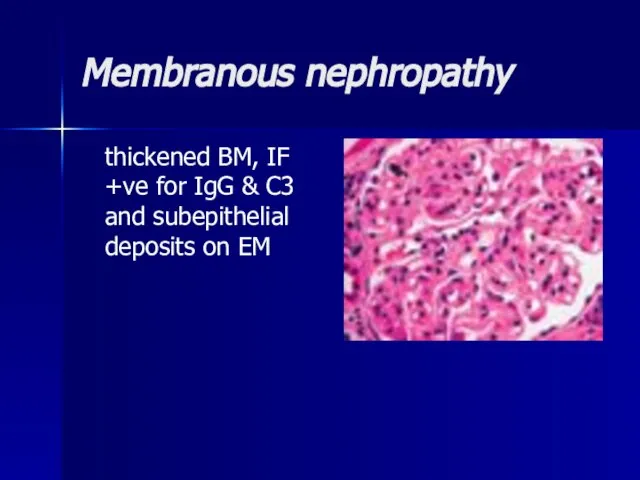
- 24. Membranous nephropathy thickened BM, IF +ve for IgG & C3 and subepithelial deposits on EM
- 25. Mesangial proliferative GN Hypercellularity, mesangial proliferation, inflammatory cell infiltrate, positive IF for IgG and C3 and
- 26. Clinical Manifestations Uremia-specific findings Edemas Hypertension Jugular venous distension (if severe volume overload is present) Pulmonary
- 27. Clinical variants Latent (changes in urine) Hypertensive (increased blood pressure) Hematuric Nephrotic (edemas, proteinuria, hypoproteinemia, hypercholesterolemia),
- 28. Lab Studies Urinalysis Urinary protein excretion CBC count Serum chemistry Serum creatinine and urea nitrogen levels
- 29. Imaging Studies Renal ultrasonogram Obtain a renal ultrasonogram to determine renal size, to assess for the
- 30. Differentials Azotemia Azotemia, Chronic Renal Failure Azotemia, Chronic Renal Failure, Acute Glomerulonephritis, Azotemia, Chronic Renal Failure,
- 31. Treatment The target pressure for patients with proteinuria greater than 1 g/d is less than 125/75
- 32. Treatment Renal osteodystrophy can be managed early by replacing vitamin D and by administering phosphate binders.
- 33. Treatment Minimal change glomerulonephritis (MCGN) Corticosteroids induce remission in >90% of children and 80% of adults
- 34. Treatment Focal segmental glomerulosclerosis Poor response to corticosteroids (10–30%). Cyclophosphamide or ciclosporin (=cylosporin) may be used
- 35. Treatment Mesangiocapillary GN Treatment: None is of proven benefit. Prognosis: 50% develop ESRF.
- 36. Treatment Membranous nephropathy If renal function deteriorates, consider corticosteroids and chlorambucil (Ponticelli regimen). Prognosis: Untreated, 15%
- 37. Treatment Mesangial proliferative GN Antibiotics, diuretics, and antihypertensives as necessary. Dialysis is rarely required. Prognosis: Good.
- 38. Rapidly Progressive Glomerulonephritis Rapidly progressive glomerulonephritis (RPGN) is a disease of the kidney that results in
- 39. Etiology The cause of RPGN is unknown. A genetic predisposition may exist for the development of
- 40. Pathogenesis In the mid 1970s, a group of patients was described who fit the clinical criteria
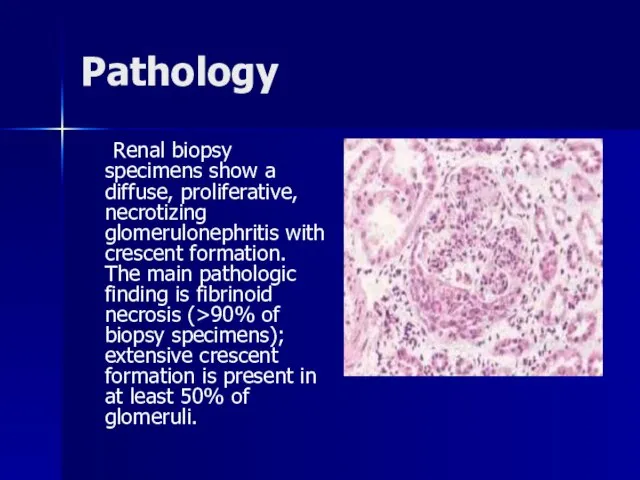
- 41. Pathology Renal biopsy specimens show a diffuse, proliferative, necrotizing glomerulonephritis with crescent formation. The main pathologic
- 42. Classification RPGN is classified pathologically into 3 categories: (1) anti-GBM antibody disease (approximately 3% of cases),
- 43. Clinical Manifestations Symptoms and signs of renal failure, loin pain, haematuria, systemic symptoms (fever, malaise, myalgia,
- 44. Workup: Lab Studies The most important requirement in the diagnosis ofantineutrophil cytoplasmic antibodies (ANCA) ANCA-associated disease
- 45. Differentials Amyloidosis, Amyloidosis, Antiphospholipid Syndrome, Amyloidosis, Antiphospholipid Syndrome, Churg-Strauss Syndrome, Amyloidosis, Antiphospholipid Syndrome, Churg-Strauss Syndrome, Cryoglobulinemia,
- 46. Treatment High-dose corticosteroids; cyclophosphamide ± plasma exchange/ renal transplantation. Prognosis: Poor if initial serum creatinine >600µmol/L.
- 47. Chronic Pyelonephritis Chronic pyelonephritis is renal injury induced by recurrent or persistent renal infection.
- 48. Etiology E. coli is the commonest (>70% in the community and 41% in hospital). Others include
- 49. Pathogenesis It occurs almost exclusively in patients with major anatomic anomalies, including urinary tract obstruction, struvite
- 50. Clinical Manifestations Fever Lethargy Nausea and vomiting Flank pain or dysuria Hypertension
- 51. Workup Lab Studies: Urinalysis Urinalysis results may reveal pyuria. Obtain a urine culture, which often isolates
- 52. Imaging Studies Intravenous urogram Voiding cystourethrogram. Radioisotopic scanning with technetium dimercaptosuccinic acid.
- 53. Imaging Studies Cystoscopy. Renal sonography. CT scan.
- 54. Differentials Azotemia, Azotemia, Chronic Renal Failure, Azotemia, Chronic Renal Failure, Hypertension, Azotemia, Chronic Renal Failure, Hypertension,
- 55. Treatment Medical therapy with antibiotics such as amoxicillin, trimethoprim/sulfamethoxazole (Bactrim), trimethoprim alone, or nitrofurantoin is usually
- 56. Surgical Care The following are indications for surgical therapy: Failure to comply with medical regimen Breakthrough
- 58. Скачать презентацию
Слайд 3Etiology
Infectious
Streptococcal
Nonstreptococcal postinfectious glomerulonephritis
Bacterial
Viral
Parasitic
Noninfectious
Multisystem systemic diseases
Primary glomerular diseases
Etiology
Infectious
Streptococcal
Nonstreptococcal postinfectious glomerulonephritis
Bacterial
Viral
Parasitic
Noninfectious
Multisystem systemic diseases
Primary glomerular diseases
Слайд 4Pathogenesis
Previously M-protein of the organism was felt to be responsible for
Pathogenesis
Previously M-protein of the organism was felt to be responsible for
Слайд 5Pathology
Diffuse endocapillary proliferative changes are found. In postinfectious GN, the glomerulus is
Pathology
Diffuse endocapillary proliferative changes are found. In postinfectious GN, the glomerulus is
Слайд 6Clinical Manifestations
edemas,
decreased volume and frequency of urination,
systemic hypertension,
uremic symptoms,
Clinical Manifestations
edemas,
decreased volume and frequency of urination,
systemic hypertension,
uremic symptoms,
Слайд 7Clinical syndromes
urinary (haematuria, proteinuria),
nephritic (edemas, hypertension, gross haematuria, proteinuria),
nephrotic (edemas, proteinuria,
Clinical syndromes
urinary (haematuria, proteinuria),
nephritic (edemas, hypertension, gross haematuria, proteinuria),
nephrotic (edemas, proteinuria,
Слайд 8Workup
Lab Studies:
Urinalysis
Blood, urea, and nitrogen (BUN); serum creatinine; and
Workup
Lab Studies:
Urinalysis
Blood, urea, and nitrogen (BUN); serum creatinine; and
Слайд 9Imaging Studies:
Abdominal ultrasound
Assesses renal size
Assesses echogenicity of renal cortex
Excludes obstruction
Imaging Studies:
Abdominal ultrasound
Assesses renal size
Assesses echogenicity of renal cortex
Excludes obstruction
Слайд 10Histologic Findings:
Generally, a renal biopsy is not necessary for diagnosis of
Histologic Findings:
Generally, a renal biopsy is not necessary for diagnosis of
Слайд 11Histologic Findings:
Diffuse endocapillary proliferative changes are found. In postinfectious GN, the glomerulus
Histologic Findings:
Diffuse endocapillary proliferative changes are found. In postinfectious GN, the glomerulus
Слайд 12Histologic Findings:
Immunofluorescence may show fine granular deposits of immunoglobulin G in a
Histologic Findings:
Immunofluorescence may show fine granular deposits of immunoglobulin G in a
Слайд 13Histologic Findings:
Large subepithelial deposits may be observed on electron microscopy. Crescents may
Histologic Findings:
Large subepithelial deposits may be observed on electron microscopy. Crescents may
Слайд 14Differentials
Crescentic Glomerulonephritis, Crescentic Glomerulonephritis, Diffuse Proliferative Glomerulonephritis, Crescentic Glomerulonephritis, Diffuse Proliferative Glomerulonephritis,
Differentials
Crescentic Glomerulonephritis, Crescentic Glomerulonephritis, Diffuse Proliferative Glomerulonephritis, Crescentic Glomerulonephritis, Diffuse Proliferative Glomerulonephritis,
Слайд 15Treatment
Treat the underlying infections when acute GN is associated with chronic infections.
Treatment
Treat the underlying infections when acute GN is associated with chronic infections.
Слайд 16Prognosis
Prognosis of acute PSGN is generally excellent in children.
Within a week
Prognosis
Prognosis of acute PSGN is generally excellent in children.
Within a week
Слайд 17Chronic glomerulonephritis
The condition is characterized by irreversible and progressive glomerular and
Chronic glomerulonephritis
The condition is characterized by irreversible and progressive glomerular and
Слайд 18Etiology
Nearly all forms of acute glomerulonephritis have a tendency to progress to chronic glomerulonephritis.
Etiology
Nearly all forms of acute glomerulonephritis have a tendency to progress to chronic glomerulonephritis.
Слайд 19Pathogenesis
Reduction in nephron mass from the initial injury reduces the GFR.
Pathogenesis
Reduction in nephron mass from the initial injury reduces the GFR.
Слайд 20Histologic Findings
In early stages, the glomeruli may still show some evidence of
Histologic Findings
In early stages, the glomeruli may still show some evidence of
Слайд 21Minimal-Change Disease
fusion of podocytes on electron microscopy
Minimal-Change Disease
fusion of podocytes on electron microscopy
Слайд 22Focal segmental glomerulosclerosis
Segmental areas of glomerular sclerosis, hyalinization of glomerular capillaries
Focal segmental glomerulosclerosis
Segmental areas of glomerular sclerosis, hyalinization of glomerular capillaries
Слайд 23Mesangiocapillary GN
large glomeruli with mesangial proliferation and ‘double’ BM. 2 histological types:
Mesangiocapillary GN
large glomeruli with mesangial proliferation and ‘double’ BM. 2 histological types:
Слайд 24Membranous nephropathy
thickened BM, IF +ve for IgG & C3 and subepithelial
Membranous nephropathy
thickened BM, IF +ve for IgG & C3 and subepithelial
Слайд 25Mesangial proliferative GN
Hypercellularity, mesangial proliferation, inflammatory cell infiltrate, positive IF for IgG
Mesangial proliferative GN
Hypercellularity, mesangial proliferation, inflammatory cell infiltrate, positive IF for IgG
Слайд 26Clinical Manifestations
Uremia-specific findings
Edemas
Hypertension
Jugular venous distension (if severe volume overload is
Clinical Manifestations
Uremia-specific findings
Edemas
Hypertension
Jugular venous distension (if severe volume overload is
Слайд 27Clinical variants
Latent (changes in urine)
Hypertensive (increased blood pressure)
Hematuric
Nephrotic (edemas, proteinuria, hypoproteinemia,
Clinical variants
Latent (changes in urine)
Hypertensive (increased blood pressure)
Hematuric
Nephrotic (edemas, proteinuria, hypoproteinemia,
Слайд 28Lab Studies
Urinalysis
Urinary protein excretion
CBC count
Serum chemistry
Serum creatinine and
Lab Studies
Urinalysis
Urinary protein excretion
CBC count
Serum chemistry
Serum creatinine and
Слайд 29Imaging Studies
Renal ultrasonogram
Obtain a renal ultrasonogram to determine renal size, to
Imaging Studies
Renal ultrasonogram
Obtain a renal ultrasonogram to determine renal size, to
Слайд 30Differentials
Azotemia Azotemia, Chronic Renal Failure Azotemia, Chronic Renal Failure, Acute Glomerulonephritis, Azotemia, Chronic Renal
Differentials
Azotemia Azotemia, Chronic Renal Failure Azotemia, Chronic Renal Failure, Acute Glomerulonephritis, Azotemia, Chronic Renal
Слайд 31Treatment
The target pressure for patients with proteinuria greater than 1 g/d is
Treatment
The target pressure for patients with proteinuria greater than 1 g/d is
Слайд 32Treatment
Renal osteodystrophy can be managed early by replacing vitamin D and by
Treatment
Renal osteodystrophy can be managed early by replacing vitamin D and by
Слайд 33Treatment
Minimal change glomerulonephritis (MCGN)
Corticosteroids induce remission in >90% of children and 80%
Treatment
Minimal change glomerulonephritis (MCGN)
Corticosteroids induce remission in >90% of children and 80%
Слайд 34Treatment
Focal segmental glomerulosclerosis
Poor response to corticosteroids (10–30%). Cyclophosphamide or ciclosporin (=cylosporin) may
Treatment
Focal segmental glomerulosclerosis
Poor response to corticosteroids (10–30%). Cyclophosphamide or ciclosporin (=cylosporin) may
Слайд 35Treatment
Mesangiocapillary GN
Treatment: None is of proven benefit.
Prognosis: 50% develop ESRF.
Treatment
Mesangiocapillary GN
Treatment: None is of proven benefit.
Prognosis: 50% develop ESRF.
Слайд 36Treatment
Membranous nephropathy
If renal function deteriorates, consider corticosteroids and chlorambucil (Ponticelli regimen). Prognosis:
Treatment
Membranous nephropathy
If renal function deteriorates, consider corticosteroids and chlorambucil (Ponticelli regimen). Prognosis:
Слайд 37Treatment
Mesangial proliferative GN
Antibiotics, diuretics, and antihypertensives as necessary. Dialysis is rarely required.
Treatment
Mesangial proliferative GN
Antibiotics, diuretics, and antihypertensives as necessary. Dialysis is rarely required.
Слайд 38Rapidly Progressive Glomerulonephritis
Rapidly progressive glomerulonephritis (RPGN) is a disease of the
Rapidly Progressive Glomerulonephritis
Rapidly progressive glomerulonephritis (RPGN) is a disease of the
Слайд 39Etiology
The cause of RPGN is unknown. A genetic predisposition may exist for
Etiology
The cause of RPGN is unknown. A genetic predisposition may exist for
Слайд 40Pathogenesis
In the mid 1970s, a group of patients was described who fit
Pathogenesis
In the mid 1970s, a group of patients was described who fit
Слайд 41Pathology
Renal biopsy specimens show a diffuse, proliferative, necrotizing glomerulonephritis with crescent formation.
Pathology
Renal biopsy specimens show a diffuse, proliferative, necrotizing glomerulonephritis with crescent formation.
Слайд 42Classification
RPGN is classified pathologically into 3 categories:
(1) anti-GBM antibody disease (approximately
Classification
RPGN is classified pathologically into 3 categories:
(1) anti-GBM antibody disease (approximately
Слайд 43Clinical Manifestations
Symptoms and signs of renal failure,
loin pain,
haematuria,
systemic symptoms
Clinical Manifestations
Symptoms and signs of renal failure,
loin pain,
haematuria,
systemic symptoms
Слайд 44Workup: Lab Studies
The most important requirement in the diagnosis ofantineutrophil cytoplasmic antibodies
Workup: Lab Studies
The most important requirement in the diagnosis ofantineutrophil cytoplasmic antibodies
Слайд 45Differentials
Amyloidosis, Amyloidosis, Antiphospholipid Syndrome, Amyloidosis, Antiphospholipid Syndrome, Churg-Strauss Syndrome, Amyloidosis, Antiphospholipid Syndrome,
Differentials
Amyloidosis, Amyloidosis, Antiphospholipid Syndrome, Amyloidosis, Antiphospholipid Syndrome, Churg-Strauss Syndrome, Amyloidosis, Antiphospholipid Syndrome,
Слайд 46Treatment
High-dose corticosteroids; cyclophosphamide ± plasma exchange/ renal transplantation. Prognosis: Poor if initial
Treatment
High-dose corticosteroids; cyclophosphamide ± plasma exchange/ renal transplantation. Prognosis: Poor if initial
Слайд 47Chronic Pyelonephritis
Chronic pyelonephritis is renal injury induced by recurrent or persistent
Chronic Pyelonephritis
Chronic pyelonephritis is renal injury induced by recurrent or persistent
Слайд 48Etiology
E. coli is the commonest (>70% in the community and 41% in
Etiology
E. coli is the commonest (>70% in the community and 41% in
Слайд 49Pathogenesis
It occurs almost exclusively in patients with major anatomic anomalies, including urinary
Pathogenesis
It occurs almost exclusively in patients with major anatomic anomalies, including urinary
Слайд 50Clinical Manifestations
Fever
Lethargy
Nausea and vomiting
Flank pain or dysuria
Hypertension
Clinical Manifestations
Fever
Lethargy
Nausea and vomiting
Flank pain or dysuria
Hypertension
Слайд 51Workup
Lab Studies:
Urinalysis
Urinalysis results may reveal pyuria.
Obtain a urine culture, which often
Workup
Lab Studies:
Urinalysis
Urinalysis results may reveal pyuria.
Obtain a urine culture, which often
Слайд 52Imaging Studies
Intravenous urogram
Voiding cystourethrogram.
Radioisotopic scanning with technetium dimercaptosuccinic acid.
Imaging Studies
Intravenous urogram
Voiding cystourethrogram.
Radioisotopic scanning with technetium dimercaptosuccinic acid.
Слайд 53Imaging Studies
Cystoscopy.
Renal sonography.
CT scan.
Imaging Studies
Cystoscopy.
Renal sonography.
CT scan.
Слайд 54Differentials
Azotemia, Azotemia, Chronic Renal Failure, Azotemia, Chronic Renal Failure, Hypertension, Azotemia, Chronic
Differentials
Azotemia, Azotemia, Chronic Renal Failure, Azotemia, Chronic Renal Failure, Hypertension, Azotemia, Chronic
Слайд 55Treatment
Medical therapy with antibiotics such as amoxicillin, trimethoprim/sulfamethoxazole (Bactrim), trimethoprim alone,
Treatment
Medical therapy with antibiotics such as amoxicillin, trimethoprim/sulfamethoxazole (Bactrim), trimethoprim alone,
Слайд 56Surgical Care
The following are indications for surgical therapy:
Failure to comply with medical
Surgical Care
The following are indications for surgical therapy:
Failure to comply with medical
 Третий закон Ньютона
Третий закон Ньютона Колобок
Колобок Добро пожаловать в Батель
Добро пожаловать в Батель Модульно-рейтинговая технология на уроках информатики в старших классах
Модульно-рейтинговая технология на уроках информатики в старших классах Труд и творчество 6 класс
Труд и творчество 6 класс Когнитивная тревога у спортсменов-стрелков: причины формирования, формы проявления, способы управления
Когнитивная тревога у спортсменов-стрелков: причины формирования, формы проявления, способы управления Терроризм – угроза обществу
Терроризм – угроза обществу Компания «КСТ–«М-3» является ведущим разработчиком программного обеспечения – систем автоматизации деятельности предприятия с 1
Компания «КСТ–«М-3» является ведущим разработчиком программного обеспечения – систем автоматизации деятельности предприятия с 1 Тема коммерческого проекта: Клининговая компания «М-Клининг»
Тема коммерческого проекта: Клининговая компания «М-Клининг» Правовые нормы информационной безопасности
Правовые нормы информационной безопасности Кружок «Юный журналист» Руководитель: Леонтьева Марина Михайловна, педагог дополнительного образования МОУ ДОД «Аликовский рай
Кружок «Юный журналист» Руководитель: Леонтьева Марина Михайловна, педагог дополнительного образования МОУ ДОД «Аликовский рай Создай свою компьютерную сеть
Создай свою компьютерную сеть Актуальные Тарифные планы. Билайн
Актуальные Тарифные планы. Билайн Семья в романе Л. Н. Толстого «Война и мир»
Семья в романе Л. Н. Толстого «Война и мир» Шаблон_презентации_для_питчинга_1
Шаблон_презентации_для_питчинга_1 АНТРОПОСΑΝΘΡΩΠΟΣ _______________________________ электронный архив: от вспомогательного инструмента к творческому проекту ___________________________________.
АНТРОПОСΑΝΘΡΩΠΟΣ _______________________________ электронный архив: от вспомогательного инструмента к творческому проекту ___________________________________. Птицы Мурманской области
Птицы Мурманской области The commonwealth of the Australia
The commonwealth of the Australia Бренд взрывного роста
Бренд взрывного роста Доли и дроби
Доли и дроби Слова, близкие по значению. Синонимы
Слова, близкие по значению. Синонимы Семантико-стилистические обертоны заглавия романа A. Nothomb Antéchrista
Семантико-стилистические обертоны заглавия романа A. Nothomb Antéchrista HPL панели
HPL панели Презентация на тему Сходство человека и человекоподобных обезьян
Презентация на тему Сходство человека и человекоподобных обезьян  История старинного рукоделия. Рельефная металлопластика
История старинного рукоделия. Рельефная металлопластика Автоматическое повторное включение
Автоматическое повторное включение Экологическое загрязнение Брянской области
Экологическое загрязнение Брянской области Организационная структура страховой компании
Организационная структура страховой компании