- Diagnosis and treatment of поп-ulcerative dyspepsia syndrome

Содержание
- 2. Dyspepsia syndrome is determined as pain or discomfort localized in the epigastric area closer to the
- 3. Patients' complaints on admission corresponding to the complex of symptoms in gastric dyspepsia: pains in the
- 4. A complex of symptoms in dyspepsia syndrome is to be distinguished from the one in gastroesophageal
- 5. Depending on the causes triggering dyspeptic disorders, there is organic and functional (non-ulcerative) dyspepsia.
- 6. Organic dyspepsia is recognized if the following markers are highlighted: esophageal disease: reflux- esophagitis gastric disease:
- 7. If to exclude the diseases mentioned after a through examination, the patients (in case the dyspeptic
- 8. Classification of functional dyspepsia. According to A. Smout et al. (1992) - according to intestinal motility:
- 9. According to N. Talley (1991), M. von Oytryve et al. (1993) - ulcerative-like variant; - refluxoid
- 10. In 20-69% of patients with ulcerative-like variant the duodeno-gastric reflux, delayed evacuation from the stomach, and
- 11. Clinical variation of non-ulcerative dyspepsia. Depending on the either symptoms predominated in the clinical presentation of
- 12. Clinical characteristics of various non-ulcerative dyspepsias Ulcerative-like type Pains localized in the epigastric area Pains subside
- 13. Dyskinetic type Early saturation Feeling of repletion in the epigastria area after the meals Nausea Upper
- 14. If the symptoms presented in patients do not correspond with the underlined variants, then the symptoms
- 15. Etiology and pathogenesis Chronic gastritis usually associated with pyloric helicobacterium (H. pylori), used to be recognized
- 16. Chronic gastritis associated with H. pylori is frequently revealed in patients with non-ulcerative dyspepsia syndrome. H.
- 17. The recent findings have also exposed the lack in distinction concerning the hydrochloric acid secretion in
- 18. Gastric and duodenal motility disorder proved to be the chief pathogenetic factors of non-ulcerative dyspepsia syndrome.
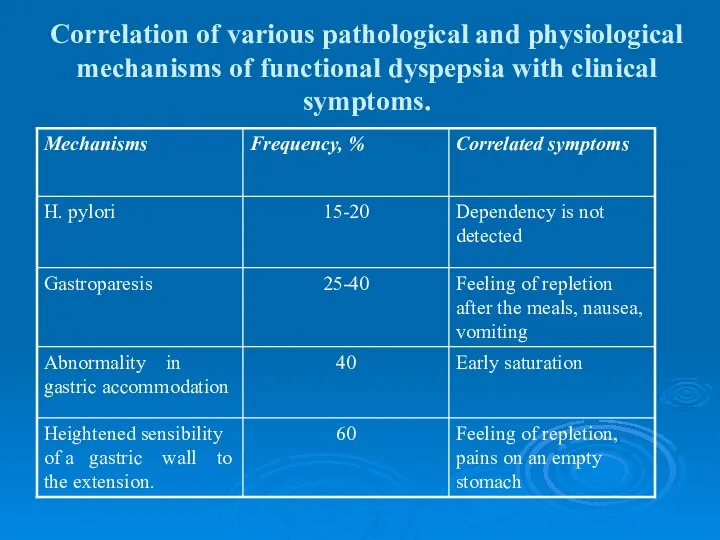
- 19. Correlation of various pathological and physiological mechanisms of functional dyspepsia with clinical symptoms.
- 20. Gastric accommodation disorder (accommodation is determined here as capability of the fundic part of the stomach
- 21. Gastric accommodation disorder (accommodation is determined here as capability of the fundic part of the stomach
- 22. If stomach evacuates the food well, the cause for the dyspeptic complaints is a heightened sensibility
- 23. Diagnosis and differential diagnosis. A complex of symptoms in non-ulcerative dyspepsia is of no specific ground,
- 24. It is essential to take into account secondary motility derangement of the upper parts of the
- 25. The syndrome of gastric dyspepsia in ulcerative disease characterizes with response on food, seasonal character of
- 26. stomach ulcer The diagnostical method of stomach ulcer is an X-ray examination. But in some cases,
- 27. Stomach cancer Stomach cancer is manifested by gastric dyspepsia, which characterizes with persistence and progression. The
- 28. chronic cholecystitis Dyspeptic complaints have a more frequent occurrence during the chronic cholecystitis development. Vomiting is
- 29. During the period of exacerbation, patients complain of nausea, bitter taste, eructation with bitter. Due to
- 30. pancreatic dyspepsia is expressed in exacerbation or severe course of the disease. It is manifested by:
- 31. Gastric dyspepsia in chronic gastritis is characterized with the dependency on diet violence. It is presented
- 32. As the disease progresses, patients with chronic gastritis have tendency to hyposecretion and reduction in acidity
- 33. Antral gastritis, gastroduodenitis may resemble ulcerative disease of the duodenum in their clinical manifestations. The disease
- 34. Gastroesophageal reflux disease is a chronic recurrence conditioned by retrograde entrance of food mass into esophagus.
- 35. Pains in the epigastrium associated or not with the food taken may occur quite often. Vomiting
- 36. Methods of differential diagnosis applied in functional dyspepsia. Esophagogastroduodenoscopy X-ray examination Ultrasonography Intragastric and intraesophageal monitoring
- 37. Clinical and biomedical blood tests, as well as ultrasound investigations of the abdomen, gastroduodenoscopy and X-ray
- 38. It is supposed to be important to take alarm symptoms or «red flags» into account while
- 39. Alarm symptoms are characterized as follows: fever anemia dysphagy leukocytosis visible admixture accelerated ESR blood in
- 40. Treatment. The treatment procedures are to be complex and include not only drug administration, but also
- 41. Antacidic and antisecretory drugs (H2-blockers and blockers of proton pump) are indicated in ulcerative-like variant of
- 42. Some patients (about 20-25%) may express positive response to anti-helicobacterial eradication therapy. The treatment may have
- 43. Eradication therapy T. Omeprasoli 20 mg 2 t. a day T. Clarithromycini 500 mg 2 t.
- 44. The basic means of patients' treatment of a developing dyskinetic variant is supposed to be prokinetic
- 45. The use of metodopramide (especially long-term one) may cause untoward and side effects in a great
- 46. European Motilium investigations in non-ulcerative dyspepsia treatment at doses of 5-20 mg 3-4 times a day
- 47. Итомед (Itomed) итоприда гидрохлорид 50 мг 3 раза в день side effects: -лейкопения, тромбоцитопения, гинекомастия, гиперпролактинемия;
- 48. Cyzapride (propulside, coordinacs) attracts much attention. This drug is quite effective in functional dyspepsia (in 60-90%>
- 50. Скачать презентацию
Слайд 3Patients' complaints on admission corresponding to the complex of symptoms in gastric
Patients' complaints on admission corresponding to the complex of symptoms in gastric
Слайд 4A complex of symptoms in dyspepsia syndrome is to be distinguished from
A complex of symptoms in dyspepsia syndrome is to be distinguished from
Слайд 5Depending on the causes triggering dyspeptic disorders, there is organic and functional
Depending on the causes triggering dyspeptic disorders, there is organic and functional
Слайд 6Organic dyspepsia is recognized if the following markers are highlighted:
esophageal disease: reflux-
Organic dyspepsia is recognized if the following markers are highlighted:
esophageal disease: reflux-
Слайд 7If to exclude the diseases mentioned after a through examination, the patients
If to exclude the diseases mentioned after a through examination, the patients
Слайд 8Classification of functional dyspepsia.
According to A. Smout et al. (1992)
- according
Classification of functional dyspepsia.
According to A. Smout et al. (1992)
- according
Слайд 9According to N. Talley (1991), M. von Oytryve et al. (1993)
- ulcerative-like
According to N. Talley (1991), M. von Oytryve et al. (1993)
- ulcerative-like
Слайд 10 In 20-69% of patients with ulcerative-like variant the duodeno-gastric reflux, delayed
In 20-69% of patients with ulcerative-like variant the duodeno-gastric reflux, delayed
Слайд 11Clinical variation of non-ulcerative dyspepsia.
Depending on the either symptoms predominated in the
Clinical variation of non-ulcerative dyspepsia.
Depending on the either symptoms predominated in the
Слайд 12Clinical characteristics of various non-ulcerative dyspepsias
Ulcerative-like type
Pains localized in the epigastric
Clinical characteristics of various non-ulcerative dyspepsias
Ulcerative-like type
Pains localized in the epigastric
Слайд 13Dyskinetic type
Early saturation
Feeling of repletion in the epigastria area after the meals
Nausea
Upper
Dyskinetic type
Early saturation
Feeling of repletion in the epigastria area after the meals
Nausea
Upper
Слайд 14If the symptoms presented in patients do not correspond with the underlined
If the symptoms presented in patients do not correspond with the underlined
Слайд 15Etiology and pathogenesis
Chronic gastritis usually associated with pyloric helicobacterium (H. pylori),
Etiology and pathogenesis
Chronic gastritis usually associated with pyloric helicobacterium (H. pylori),
Слайд 16Chronic gastritis associated with H. pylori is frequently revealed in patients with
Chronic gastritis associated with H. pylori is frequently revealed in patients with
Слайд 17The recent findings have also exposed the lack in distinction concerning the
The recent findings have also exposed the lack in distinction concerning the
Слайд 18Gastric and duodenal motility disorder proved to be the chief pathogenetic factors
Gastric and duodenal motility disorder proved to be the chief pathogenetic factors
Слайд 19Correlation of various pathological and physiological mechanisms of functional dyspepsia with clinical
Correlation of various pathological and physiological mechanisms of functional dyspepsia with clinical
Слайд 20Gastric accommodation disorder (accommodation is determined here as capability of the fundic
Gastric accommodation disorder (accommodation is determined here as capability of the fundic
Слайд 21Gastric accommodation disorder (accommodation is determined here as capability of the fundic
Gastric accommodation disorder (accommodation is determined here as capability of the fundic
Слайд 22If stomach evacuates the food well, the cause for the dyspeptic complaints
If stomach evacuates the food well, the cause for the dyspeptic complaints
Слайд 23Diagnosis and differential diagnosis.
A complex of symptoms in non-ulcerative dyspepsia is of
Diagnosis and differential diagnosis.
A complex of symptoms in non-ulcerative dyspepsia is of
Слайд 24It is essential to take into account secondary motility derangement of the
It is essential to take into account secondary motility derangement of the
Слайд 25The syndrome of gastric dyspepsia in ulcerative disease characterizes with response on
The syndrome of gastric dyspepsia in ulcerative disease characterizes with response on
Слайд 26stomach ulcer
The diagnostical method of stomach ulcer is an X-ray examination. But
stomach ulcer
The diagnostical method of stomach ulcer is an X-ray examination. But
Слайд 27Stomach cancer
Stomach cancer is manifested by gastric dyspepsia, which characterizes with persistence
Stomach cancer
Stomach cancer is manifested by gastric dyspepsia, which characterizes with persistence
Слайд 28chronic cholecystitis
Dyspeptic complaints have a more frequent occurrence during the chronic cholecystitis
chronic cholecystitis
Dyspeptic complaints have a more frequent occurrence during the chronic cholecystitis
Слайд 29During the period of exacerbation, patients complain of nausea, bitter taste, eructation
During the period of exacerbation, patients complain of nausea, bitter taste, eructation
Слайд 30pancreatic dyspepsia
is expressed in exacerbation or severe course of the disease. It
pancreatic dyspepsia
is expressed in exacerbation or severe course of the disease. It
Слайд 31Gastric dyspepsia in chronic gastritis
is characterized with the dependency on diet violence.
Gastric dyspepsia in chronic gastritis
is characterized with the dependency on diet violence.
Слайд 32As the disease progresses, patients with chronic gastritis have tendency to hyposecretion
As the disease progresses, patients with chronic gastritis have tendency to hyposecretion
Слайд 33Antral gastritis, gastroduodenitis may resemble ulcerative disease of the duodenum in their
Antral gastritis, gastroduodenitis may resemble ulcerative disease of the duodenum in their
Слайд 34Gastroesophageal reflux disease
is a chronic recurrence conditioned by retrograde entrance of
Gastroesophageal reflux disease
is a chronic recurrence conditioned by retrograde entrance of
Слайд 35Pains in the epigastrium associated or not with the food taken may
Pains in the epigastrium associated or not with the food taken may
Слайд 36Methods of differential diagnosis applied in functional dyspepsia.
Esophagogastroduodenoscopy
X-ray examination
Ultrasonography
Intragastric and intraesophageal monitoring
Methods of differential diagnosis applied in functional dyspepsia.
Esophagogastroduodenoscopy
X-ray examination
Ultrasonography
Intragastric and intraesophageal monitoring
Слайд 37Clinical and biomedical blood tests, as well as ultrasound investigations of the
Clinical and biomedical blood tests, as well as ultrasound investigations of the
Слайд 38It is supposed to be important to take alarm symptoms or «red
It is supposed to be important to take alarm symptoms or «red
Слайд 39Alarm symptoms are characterized as follows:
fever
anemia
dysphagy
leukocytosis
visible admixture
accelerated ESR
blood in feces
dyspepsia symptoms occurred
Alarm symptoms are characterized as follows:
fever
anemia
dysphagy
leukocytosis
visible admixture
accelerated ESR
blood in feces
dyspepsia symptoms occurred
Слайд 40Treatment.
The treatment procedures are to be complex and include not only drug
Treatment.
The treatment procedures are to be complex and include not only drug
Слайд 41Antacidic and antisecretory drugs (H2-blockers and blockers of proton pump) are indicated
Antacidic and antisecretory drugs (H2-blockers and blockers of proton pump) are indicated
Слайд 42Some patients (about 20-25%) may express positive response to anti-helicobacterial eradication therapy.
Some patients (about 20-25%) may express positive response to anti-helicobacterial eradication therapy.
Слайд 43Eradication therapy
T. Omeprasoli 20 mg 2 t. a day
T. Clarithromycini 500 mg
Eradication therapy
T. Omeprasoli 20 mg 2 t. a day
T. Clarithromycini 500 mg
Слайд 44The basic means of patients' treatment of a developing dyskinetic variant is
The basic means of patients' treatment of a developing dyskinetic variant is

Слайд 45The use of metodopramide (especially long-term one) may cause untoward and side
The use of metodopramide (especially long-term one) may cause untoward and side
Слайд 46European Motilium investigations in non-ulcerative dyspepsia treatment at doses of 5-20 mg
European Motilium investigations in non-ulcerative dyspepsia treatment at doses of 5-20 mg
Слайд 47Итомед (Itomed)
итоприда гидрохлорид
50 мг 3 раза в день
side effects:
-лейкопения,
Итомед (Itomed)
итоприда гидрохлорид
50 мг 3 раза в день
side effects:
-лейкопения,
Слайд 48Cyzapride (propulside, coordinacs) attracts much attention. This drug is quite effective in
Cyzapride (propulside, coordinacs) attracts much attention. This drug is quite effective in
 Жизнь и деятельность Н.И. Пирогова
Жизнь и деятельность Н.И. Пирогова Особенности питания в послеоперационном периоде при различных вмешательствах
Особенности питания в послеоперационном периоде при различных вмешательствах Кондуктивные нарушения слуха
Кондуктивные нарушения слуха Тест баланс Берга. Риск падения
Тест баланс Берга. Риск падения Вирусные диареи
Вирусные диареи Первая помощь при кровотечениях
Первая помощь при кровотечениях Нанесение границ каркаса бюгельного протеза
Нанесение границ каркаса бюгельного протеза Кинетический тренажер для глаз
Кинетический тренажер для глаз Причины ООК. Типы ООК
Причины ООК. Типы ООК Заболевания прямой кишки
Заболевания прямой кишки Вакансии в Мурманской областной детской клинической больнице
Вакансии в Мурманской областной детской клинической больнице Основы ортодонтии для сотрудников
Основы ортодонтии для сотрудников Биохимические механизмы развития патологий тканей полости рта
Биохимические механизмы развития патологий тканей полости рта Острый респираторный дистресс-синдром
Острый респираторный дистресс-синдром Лекарственный препараты из группы антибиотиков алициклической, ароматической, гетероциклической и гликозидной структуры
Лекарственный препараты из группы антибиотиков алициклической, ароматической, гетероциклической и гликозидной структуры Центральные парезы и параличи
Центральные парезы и параличи Клинический случай. Медуллобластома мозжечка и IV желудочка, с метастазированием по оболочкам спинного мозга
Клинический случай. Медуллобластома мозжечка и IV желудочка, с метастазированием по оболочкам спинного мозга Экспресс-тестирование групп крови человека
Экспресс-тестирование групп крови человека Бронхиальная астма. Заболеваемость и смертность
Бронхиальная астма. Заболеваемость и смертность Сестринская деятельность при остром бронхите у детей
Сестринская деятельность при остром бронхите у детей Гнойное поражение кожи пиодермия
Гнойное поражение кожи пиодермия Диагностическая анатомия большеберцового нерва
Диагностическая анатомия большеберцового нерва Сестринский уход за пациентами с бронхиальной астмой
Сестринский уход за пациентами с бронхиальной астмой Анализ ассортимента и наличия лекарственных средств группы макролидов в Республике Беларусь
Анализ ассортимента и наличия лекарственных средств группы макролидов в Республике Беларусь Внешние признаки гипотироза
Внешние признаки гипотироза Центральный понтинный миелинолиз
Центральный понтинный миелинолиз Хирургические методы лечения слюнных свищей
Хирургические методы лечения слюнных свищей Узлы в хирургии
Узлы в хирургии