- Histolytica

Содержание
- 4. Anaerobic parasitic amoebozoan, part of the genus Entamoeba.[1] Predominantly infecting humans and other primates causing amoebiasis,
- 7. It was thought that 10% of the world population was infected, but these figures predate the
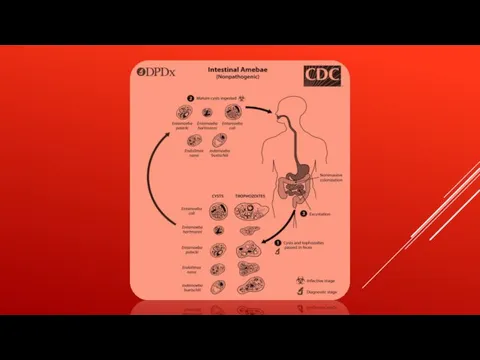
- 9. TRANSMISSION The active (trophozoite) stage exists only in the host and in fresh loose feces; cysts
- 11. The cysts are readily killed by heat and by freezing temperatures, and survive for only a
- 14. Symptoms can include fulminating dysentery, bloody diarrhea, weight loss, fatigue, abdominal pain, and amoeboma. The amoeba
- 16. RISK FACTORS Poor sanitary conditions are known to increase the risk of contracting amebiasis E. histolytica.[8]
- 18. PATHOGEN INTERACTION E. histolytica may modulate the virulence of certain human viruses and is itself a
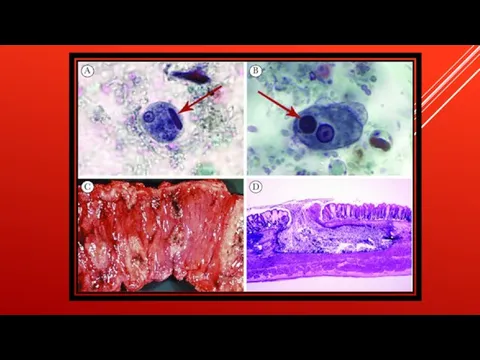
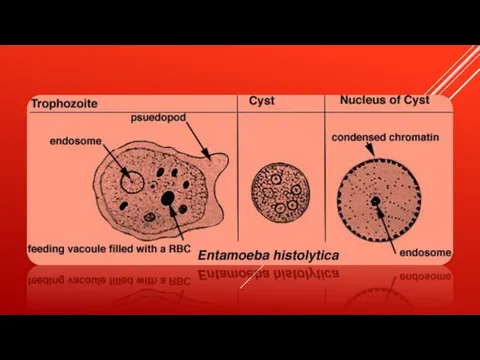
- 19. DIAGNOSIS Diagnosis is confirmed by microscopic examination for trophozoites or cysts in fresh or suitably preserved
- 21. Скачать презентацию

Слайд 4 Anaerobic parasitic amoebozoan, part of the genus Entamoeba.[1] Predominantly infecting humans and other primates causing amoebiasis, E. histolytica is estimated
Anaerobic parasitic amoebozoan, part of the genus Entamoeba.[1] Predominantly infecting humans and other primates causing amoebiasis, E. histolytica is estimated
![Anaerobic parasitic amoebozoan, part of the genus Entamoeba.[1] Predominantly infecting humans and](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/914432/slide-3.jpg)

Слайд 7
It was thought that 10% of the world population was infected, but
It was thought that 10% of the world population was infected, but
Слайд 9TRANSMISSION
The active (trophozoite) stage exists only in the host and in fresh
TRANSMISSION
The active (trophozoite) stage exists only in the host and in fresh

Слайд 11The cysts are readily killed by heat and by freezing temperatures, and
The cysts are readily killed by heat and by freezing temperatures, and

Слайд 14Symptoms can include fulminating dysentery, bloody diarrhea, weight loss, fatigue, abdominal pain,
Symptoms can include fulminating dysentery, bloody diarrhea, weight loss, fatigue, abdominal pain,
Слайд 16RISK FACTORS
Poor sanitary conditions are known to increase the risk of contracting
RISK FACTORS
Poor sanitary conditions are known to increase the risk of contracting

Слайд 18PATHOGEN INTERACTION
E. histolytica may modulate the virulence of certain human viruses and is
PATHOGEN INTERACTION
E. histolytica may modulate the virulence of certain human viruses and is
Слайд 19DIAGNOSIS
Diagnosis is confirmed by microscopic examination for trophozoites or cysts in fresh
DIAGNOSIS
Diagnosis is confirmed by microscopic examination for trophozoites or cysts in fresh
 Халықтың денсаулығының аймақтық ерекшеліктері
Халықтың денсаулығының аймақтық ерекшеліктері проект рабочего места для мастера маникюра
проект рабочего места для мастера маникюра Расстройства, связанные с недостатком глюкокортикоидов
Расстройства, связанные с недостатком глюкокортикоидов Формы и методы работы образовательной организации по повышению мотивации рационального питания (медицинский аспект)
Формы и методы работы образовательной организации по повышению мотивации рационального питания (медицинский аспект) Общая фармакология
Общая фармакология Преимплантационная генетическая диагностика
Преимплантационная генетическая диагностика Врачебная деятельность М.Я. Мудрова
Врачебная деятельность М.Я. Мудрова Фармацевтикалық көмек тұжырымдамасы
Фармацевтикалық көмек тұжырымдамасы Радиобиологические основы лучевой терапии
Радиобиологические основы лучевой терапии Лапароскопическая аппендэктомия
Лапароскопическая аппендэктомия Студенческий медицинский отряд Астра
Студенческий медицинский отряд Астра Neisseria meningitidis
Neisseria meningitidis Синдром Прадера-Вилли
Синдром Прадера-Вилли Туберкулёз и его профилактика
Туберкулёз и его профилактика Аллена - Мастерса синдром
Аллена - Мастерса синдром Наследственные заболевания с расстройствами движения
Наследственные заболевания с расстройствами движения Инфекционные заболевания кожи, вызванные вирусом папилломы человека. Лечение в условия косметологического кабинета
Инфекционные заболевания кожи, вызванные вирусом папилломы человека. Лечение в условия косметологического кабинета Определение соотношения патогенных микроорганизмов десневого кармана в норме и при пародонтите
Определение соотношения патогенных микроорганизмов десневого кармана в норме и при пародонтите Приемы развития координации и ритмизации движений
Приемы развития координации и ритмизации движений Анатомия и физиология женской репродуктивной системы
Анатомия и физиология женской репродуктивной системы Терапиялық стоматологиядағы жедел-жәрдем кажет ететін жағдайлар
Терапиялық стоматологиядағы жедел-жәрдем кажет ететін жағдайлар Антигистаминные средства
Антигистаминные средства Общие вопросы клинической трансфузиологии
Общие вопросы клинической трансфузиологии Паротит (свинка)
Паротит (свинка) Причины возникновения нарушений речи
Причины возникновения нарушений речи Пневмония у пожилых
Пневмония у пожилых Осложнённые формы олигофрении
Осложнённые формы олигофрении Bacteria-binding polymers: a novel way to reduce bacterial load in infection
Bacteria-binding polymers: a novel way to reduce bacterial load in infection