- Management of patients with cardiomegaly and heart failure

Содержание
- 2. Cardiomegaly is a considerable enlargement of the heart from its dilatation and/or hypertrophy, accumulation of waste
- 3. COMMON SIGNS OF CARDIOMEGALY Enlargement of the heart Rhythm and conduction disturbances Physical findings: widened borders
- 4. MAIN CAUSES OF CARDIOMEGALY IHD: atherosclerotic cardiosclerosis, post-infarction cardiosclerosis, ischemic cardiomyopathy, cardiac aneurysm Arterial hypertension Heart
- 5. DIAGNOSIS OF CARDIOMEGALY Interviewing the patient to find out the main complaints: dyspnoea, fatigability, weakness, less
- 6. DIAGNOSIS OF CARDIOMEGALY History. We should specify: consequence of development of heart failure symptoms (left or
- 7. DIAGNOSIS OF CARDIOMEGALY PHYSICAL EXAMINATION: Inspection: cyanosis, acrocyanosis, paleness, ruddiness of cheeks, swollen veins in the
- 8. DIAGNOSIS OF CARDIOMEGALY PHYSICAL EXAMINATION: Percussion: wider vascular bundle, wider borders of heart dullness Auscultation: dull
- 9. DIAGNOSIS OF CARDIOMEGALY LABORATORY FINDINGS: CDC: diagnosis of anaemia, polycythemia (COPD, cyanotic congenital heart defects), leucocytosis
- 10. DIAGNOSIS OF CARDIOMEGALY INSTRUMENTAL INVESTIGATIONS: Chest X-ray (shape of the heart, enlargement of certain chambers, vessels):
- 11. DIAGNOSIS OF CARDIOMEGALY INSTRUMENTAL INVESTIGATIONS: Echocardiography is the most valuable non-invasive methods of diagnosis assesses thoroughly
- 12. MANAGEMENT OF PATIENTS WITH CARDIOMEGALY To confirm cardiomegaly (to determine enlargement of the chambers, dilation or
- 13. MANAGEMENT OF PATIENTS WITH CARDIOMEGALY ASSESSMENT OF FUNCTIONAL SIGNIFICANCE OF CARDIOMEGALY: Symptoms of dyspnoea, weakness, fatigability
- 14. MANAGEMENT OF PATIENTS WITH CARDIOMEGALY PLANNING MANAGEMENT OF THE PATIENT: Prevention: changing lifestyle, treatment of hypertension,
- 15. CARDIOMYOPATHIES (CM) European Society of Cardiology (ESC), 2008 “Cardiomyopathies are structural and functional myocardial diseases in
- 16. CARDIOMYOPATHIES CM phenotypes HCM (hypertrophic CM) DCM (dilated CM) ARVD (arrhythmogenic right ventricular dysplasia) RCM (restrictive
- 17. ESC RECOMMENDATIONS (2008) All CM phenotypes are divided into: Familial (inherited, genetic) Non-identified genetic disorder A
- 18. Non-familial (acquired, non-genetic) Idiopathic A disease subgroup Toxic CM Endocrine CM Alimentary (nutritional) CM (thiamine or
- 19. HYPERTROPHIC CARDIOMYOPATHY Hypertrophic cardiomyopathy is defined by the presence of increased left ventricular (LV) wall thickness
- 20. HYPERTROPHIC CARDIOMYOPATHY 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy HCM is prevalently a
- 21. HYPERTROPHIC CARDIOMYOPATHY HCM is the main cause of sudden cardiac death (SCD) in the young, in
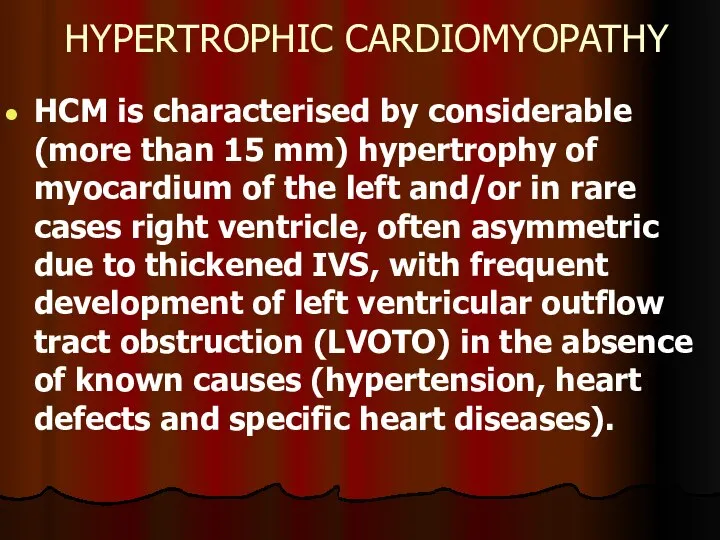
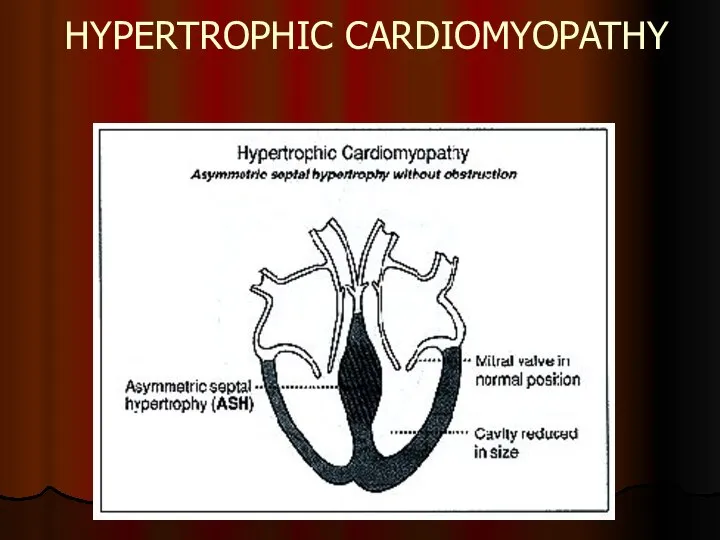
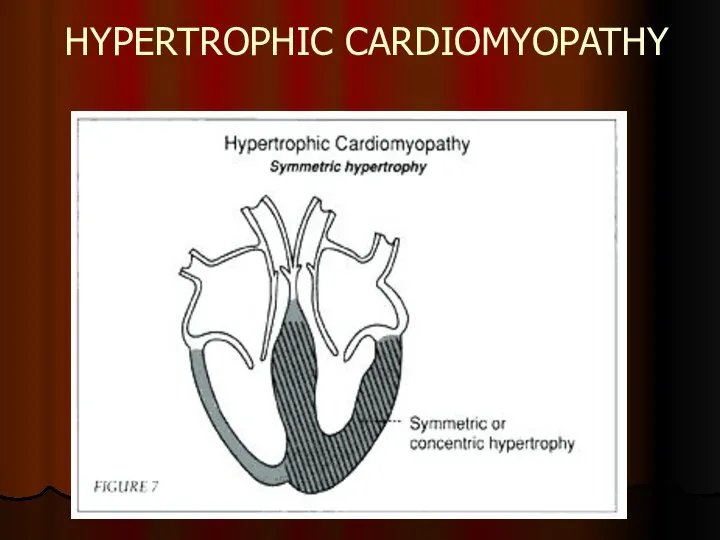
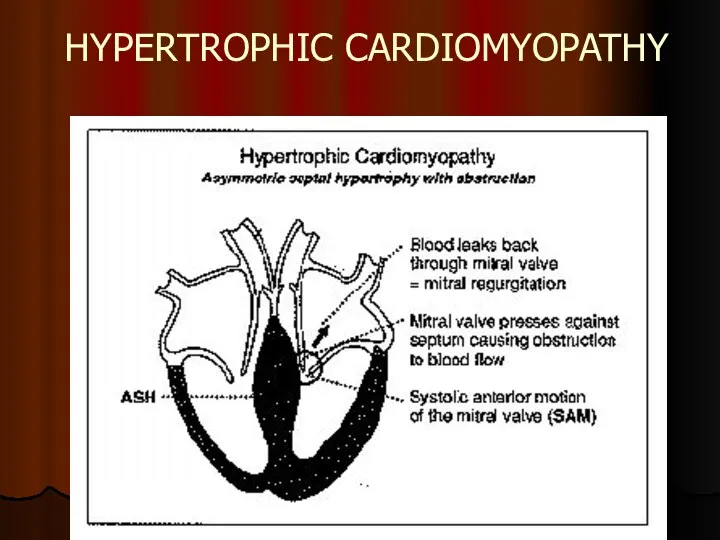
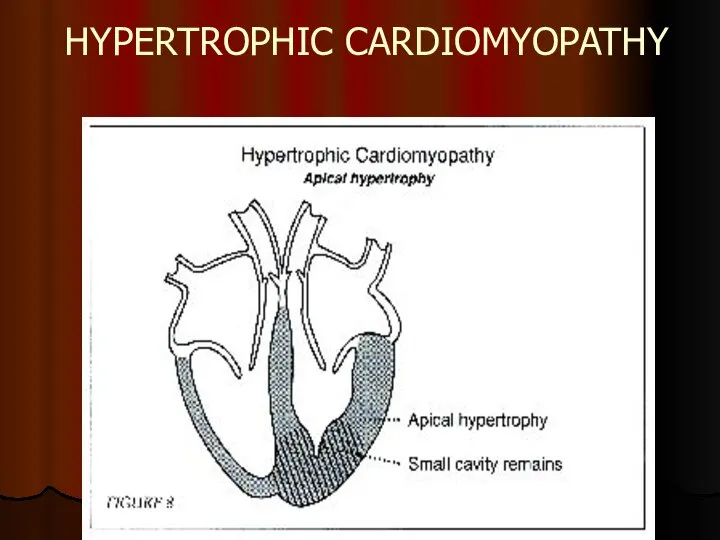
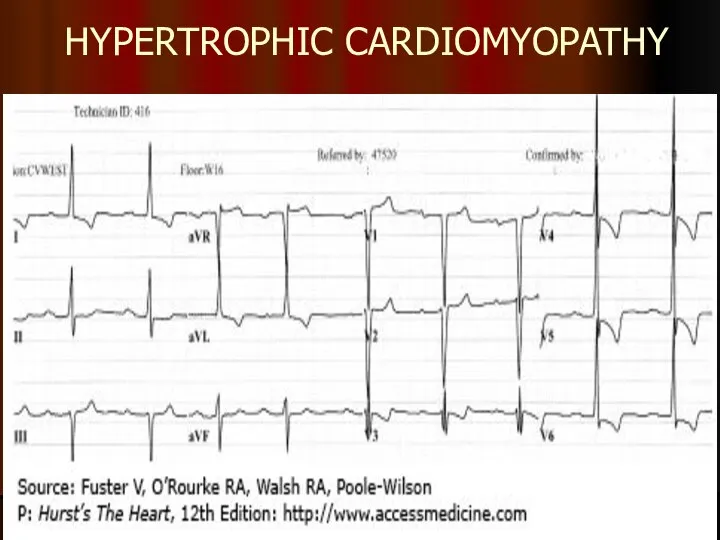
- 22. HYPERTROPHIC CARDIOMYOPATHY HCM is characterised by considerable (more than 15 mm) hypertrophy of myocardium of the
- 23. HYPERTROPHIC CARDIOMYOPATHY
- 24. HYPERTROPHIC CARDIOMYOPATHY
- 25. HYPERTROPHIC CARDIOMYOPATHY
- 26. HYPERTROPHIC CARDIOMYOPATHY
- 27. HYPERTROPHIC CARDIOMYOPATHY Pathogenesis of HCM includes 4 interrelated processes: Left ventricular outflow tract obstruction (LVOTO) Diastolic
- 28. HYPERTROPHIC CARDIOMYOPATHY CLINICAL MANIFESTATION: Asymptomatic course in 25% cases Dyspnoea on exertion (90%), orthopnoea; Angina (70-80%);
- 29. HYPERTROPHIC CARDIOMYOPATHY ON EXAMINATION: intense, raised cardiac impulse shifted slightly to the left double, triple or
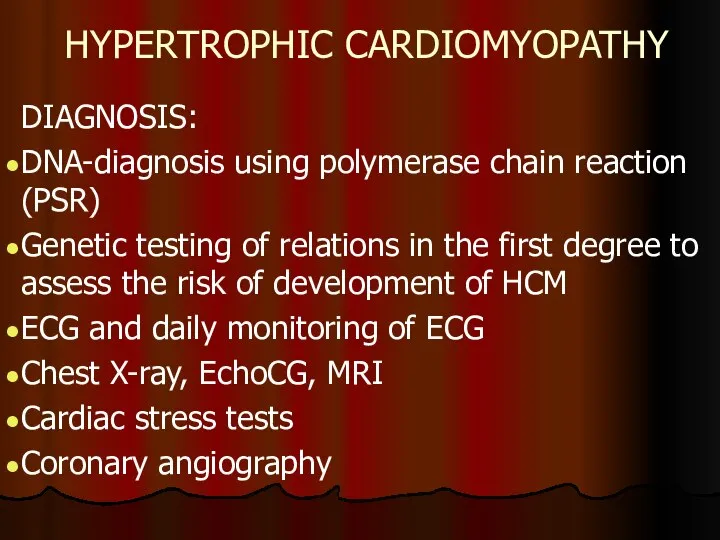
- 30. HYPERTROPHIC CARDIOMYOPATHY DIAGNOSIS: DNA-diagnosis using polymerase chain reaction (PSR) Genetic testing of relations in the first
- 31. HYPERTROPHIC CARDIOMYOPATHY
- 32. HYPERTROPHIC CARDIOMYOPATHY Left ventricular wall or IVS thickness >15 mm
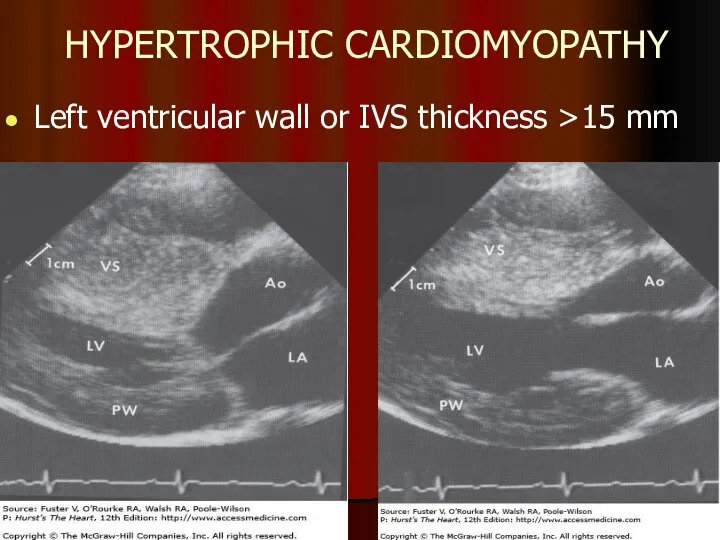
- 33. HYPERTROPHIC CARDIOMYOPATHY MEDICAL TREATMENT: ß-blockers Increase diastolic filling/relaxation of the LV Are first choice in obstructive
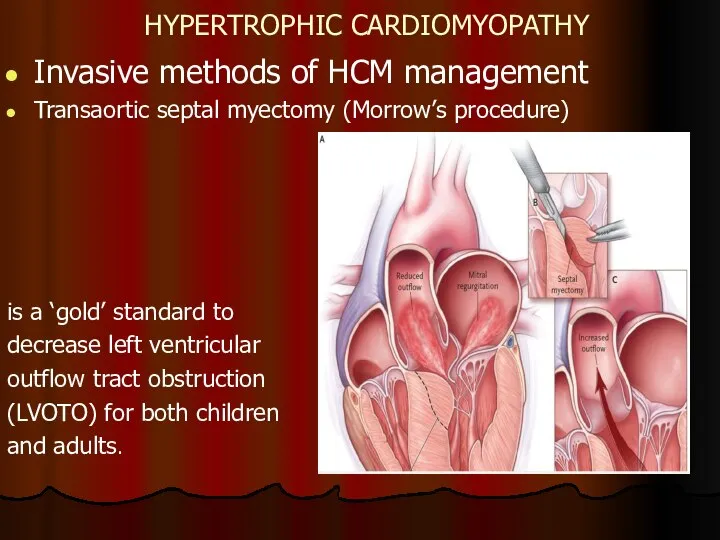
- 34. HYPERTROPHIC CARDIOMYOPATHY Invasive methods of HCM management Transaortic septal myectomy (Morrow’s procedure) is a ‘gold’ standard
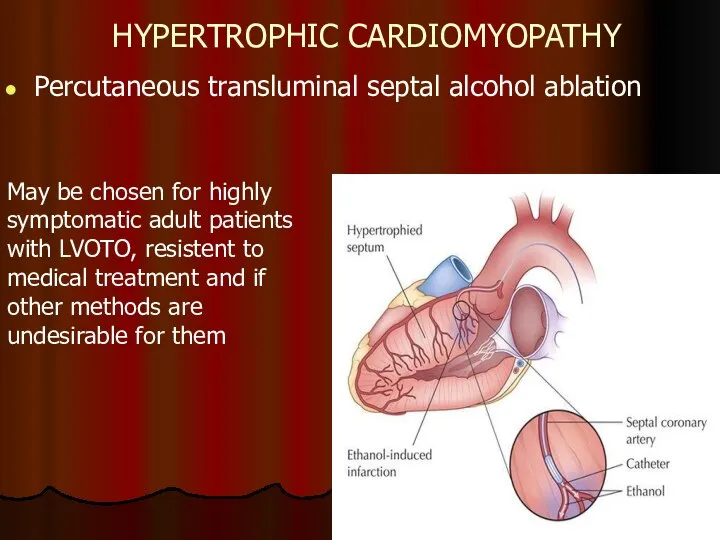
- 35. HYPERTROPHIC CARDIOMYOPATHY Percutaneous transluminal septal alcohol ablation May be chosen for highly symptomatic adult patients with
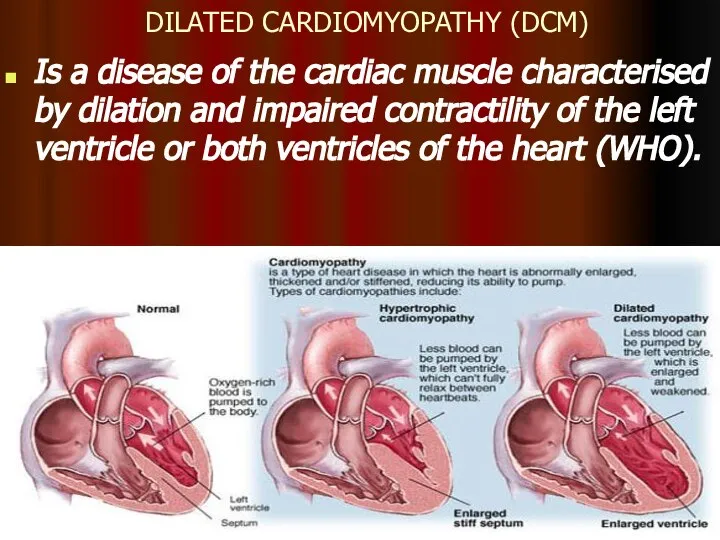
- 36. DILATED CARDIOMYOPATHY (DCM) Is a disease of the cardiac muscle characterised by dilation and impaired contractility
- 37. DILATED CARDIOMYOPATHY Dilated cardiomyopathy is responsible for 9% of all cases of heart failure. Incidence of
- 38. CLINICAL MANIFESTATIONS OF DCM Symptoms: palpitation, syncopes, weakness, dyspnoea, reduced exercise tolerance and sudden cardiac death.
- 39. CLINICAL MANIFESTATIONS OF DCM Physical changes Inspection, palpation: Swollen, pulsating jugular veins Diffuse apical pulse shifted
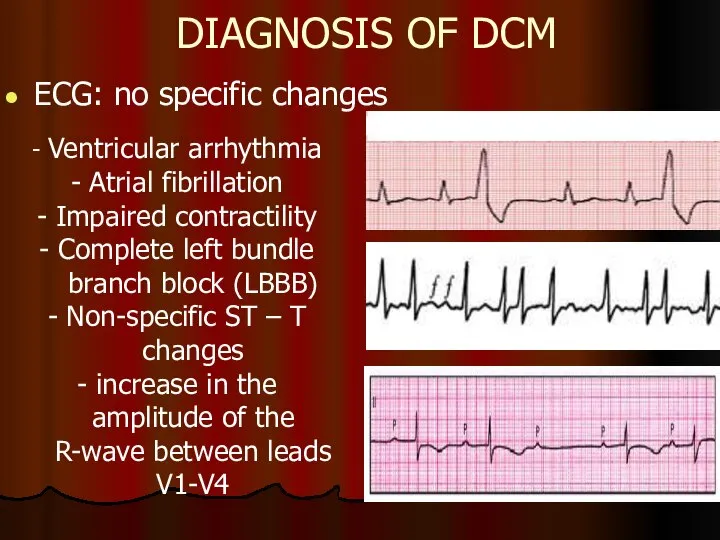
- 40. DIAGNOSIS OF DCM ECG: no specific changes - Ventricular arrhythmia - Atrial fibrillation - Impaired contractility
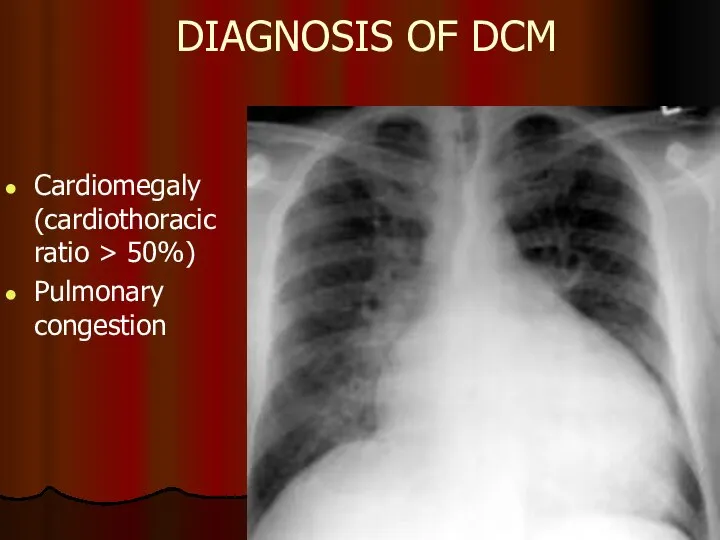
- 41. DIAGNOSIS OF DCM Cardiomegaly (cardiothoracic ratio > 50%) Pulmonary congestion
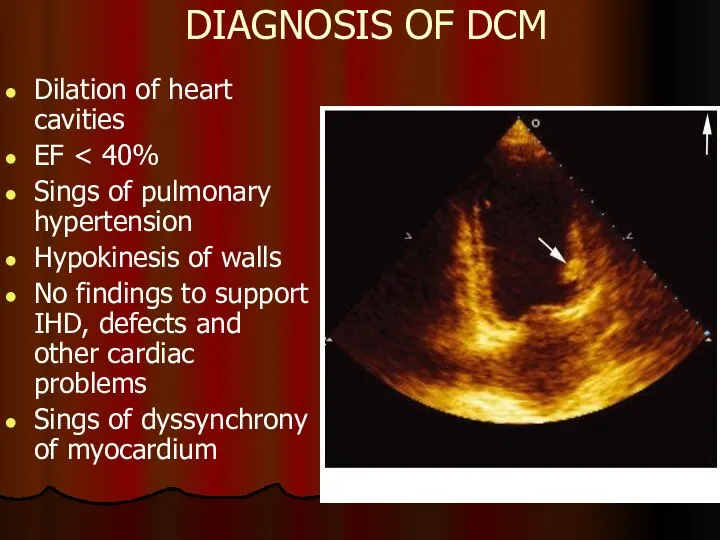
- 42. DIAGNOSIS OF DCM Dilation of heart cavities EF Sings of pulmonary hypertension Hypokinesis of walls No
- 43. DIAGNOSIS OF DCM Radionuclide methods Can be used to assess the size of heart chambers, contractility
- 44. EXCLUSION CRITERIA FOR DCM Systemic arterial hypertension (> 160/100 mm Hg) Ischaemic heart diseases (50% coronary
- 45. MANAGEMENT OF DCM To exclude factors which may worsen dysfunction of myocardium Medical treatment: Management of
- 46. MYOCARDITIS Inflammatory impairment of the heart muscle due to influence (direct or indirect through immune mechanisms)
- 47. ETIOLOGY OF MYOCARDITIS Bacteria Rickettsiae and Spirochaete Viruses Protozoa Fungi Parasitic diseases Deficiencies (hypophosphataemia, hypomagnesemia, hypocalcaemia,
- 48. VIRAL INFECTION IN MYOCARDITIS Coxsackie of A and B groups, ЕСНО, A and B flu, herpes
- 49. MYOCARDITIS THE COURSE OF THE DISEASE Mild: mostly focal, without cavity dilation, systolic dysfunction, potentially dangerous
- 50. DIAGNOSIS OF MYOCARDITIS 1 CRITERIA OF INFLAMMATION, INFECTION: Fatigue, hyperthermia, accelerated ESR, leucocytosis, elevation of C-reactive
- 51. DIAGNOSIS OF MYOCARDITIS 2 CRITERIA OF MYOCARDIAL INVOLVEMENT: Clinical: cardialgia, heart palpitations, irregular heart work, HF
- 52. DIAGNOSIS OF MYOCARDITIS New York Heart Association (NYHA) History of infection confirmed clinically and biochemically or
- 53. MANAGEMENT OF MYOCARDITIS 1 Etiotropic treatment Antibacterial, antiviral, antiparasitic drugs 2 Pathogenic treatment Non-steroidal anti-inflammatory drugs
- 54. HF is a clinical syndrome characterized by typical symptoms (e.g. breathlessness, ankle swelling and fatigue) that
- 55. A state in which the heart cannot provide sufficient cardiac output to satisfy the metabolic needs
- 56. HF – is an imprecise term used to describe the pathological state that develops when the
- 57. CLASSIFICATION Heart failure can be classified in several ways 1 - Acute and chronic HF 2
- 58. ACCF/AHA stages of HF Stage A: At high risk for HF but without structural heart disease
- 59. ESC Guidelines for diagnostic and treatment of acute and chronic HF (2016) Definition of heart failure
- 60. NEW YORK НЕАRT ASSOCIATION (NYHA) FUNCTIONAL CLASSIFICATION OF CHF I class. Patients with cardiac disease but
- 61. MANAGEMENT OF HEART FAILURE (HF) The main purposes: To reduce mortality !!! To relieve HF symptoms
- 62. THE MAIN PRINCIPLES OF HF MANAGEMENT To reveal and exclude triggering factors To normalise cardiac output
- 63. METHODS OF HF MANAGEMENT Non-medical (changing lifestyle) Pharmacotherapy (ACE inhibitors or ARBs, beta-blockers, aldosterone antagonists, diuretics,
- 64. Pharmacotherapy for HF 1 DRUGS PROVED TO BE ABLE TO REDUCE MORBIDITY AND MORTALITY RATES IN
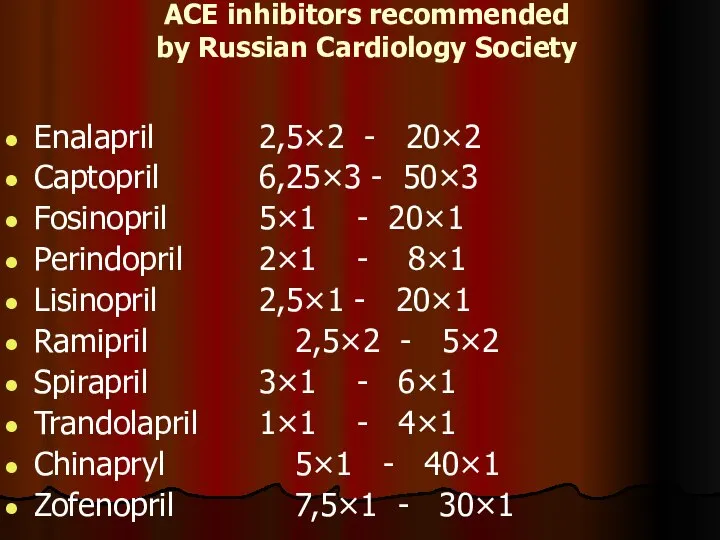
- 65. ACE inhibitors recommended by Russian Cardiology Society Enalapril 2,5×2 - 20×2 Captopril 6,25×3 - 50×3 Fosinopril
- 66. RULES FOR ADMINISTRATION OF ACE INHIBITORS To discontinue active diuretic therapy or to reduce the dosage
- 67. ESC recommendations. ARBs II with proved influence on prognosis Candesartan from 4-8 mg daily to 32
- 68. ESC recommendations. β-blockers with proved influence on prognosis Bisoprolol from 1.25 mg daily to 10 mg
- 69. Peculiarities of taking ß-blockers To all patients with manifestations of CHF due to IHD or DCM,
- 70. ESC recommendations. Aldosterone antagonists Eplerenone from 25 mg daily to 50 mg daily Spironolactone from 25
- 71. ESC recommendations. Aldosterone antagonists Contraindicated: K level >5.0 mmol/L, creatinine >220 mcmol/L, While taking other sparing
- 72. IVABRADIN, a standard medication for CHF management Reviewing European recommendations on HF (2012): Ivabradin should be
- 73. Indications for administration of diuretics: To eliminate clinical symptoms of fluid retention. They contribute to better
- 74. Doses of diuretics during active stage of HF treatment Furosemide from 20–40 mg to 40-240 mg
- 76. Скачать презентацию
Слайд 3COMMON SIGNS OF CARDIOMEGALY
Enlargement of the heart
Rhythm and conduction disturbances
Physical findings:
COMMON SIGNS OF CARDIOMEGALY
Enlargement of the heart
Rhythm and conduction disturbances
Physical findings:
Слайд 4MAIN CAUSES OF CARDIOMEGALY
IHD: atherosclerotic cardiosclerosis, post-infarction cardiosclerosis, ischemic cardiomyopathy, cardiac aneurysm
Arterial
MAIN CAUSES OF CARDIOMEGALY
IHD: atherosclerotic cardiosclerosis, post-infarction cardiosclerosis, ischemic cardiomyopathy, cardiac aneurysm
Arterial
Слайд 5DIAGNOSIS OF CARDIOMEGALY
Interviewing the patient to find out the main complaints: dyspnoea,
DIAGNOSIS OF CARDIOMEGALY
Interviewing the patient to find out the main complaints: dyspnoea,
Слайд 6DIAGNOSIS OF CARDIOMEGALY
History. We should specify: consequence of development of heart failure
DIAGNOSIS OF CARDIOMEGALY
History. We should specify: consequence of development of heart failure
Слайд 7DIAGNOSIS OF CARDIOMEGALY
PHYSICAL EXAMINATION:
Inspection: cyanosis, acrocyanosis, paleness, ruddiness of cheeks, swollen
DIAGNOSIS OF CARDIOMEGALY
PHYSICAL EXAMINATION:
Inspection: cyanosis, acrocyanosis, paleness, ruddiness of cheeks, swollen
Слайд 8DIAGNOSIS OF CARDIOMEGALY
PHYSICAL EXAMINATION:
Percussion: wider vascular bundle, wider borders of heart dullness
Auscultation:
DIAGNOSIS OF CARDIOMEGALY
PHYSICAL EXAMINATION:
Percussion: wider vascular bundle, wider borders of heart dullness
Auscultation:
Слайд 9DIAGNOSIS OF CARDIOMEGALY
LABORATORY FINDINGS:
CDC: diagnosis of anaemia, polycythemia (COPD, cyanotic congenital heart
DIAGNOSIS OF CARDIOMEGALY
LABORATORY FINDINGS:
CDC: diagnosis of anaemia, polycythemia (COPD, cyanotic congenital heart
Слайд 10DIAGNOSIS OF CARDIOMEGALY
INSTRUMENTAL INVESTIGATIONS:
Chest X-ray (shape of the heart, enlargement of certain
DIAGNOSIS OF CARDIOMEGALY
INSTRUMENTAL INVESTIGATIONS:
Chest X-ray (shape of the heart, enlargement of certain
Слайд 11DIAGNOSIS OF CARDIOMEGALY
INSTRUMENTAL INVESTIGATIONS:
Echocardiography is the most valuable non-invasive methods of diagnosis
DIAGNOSIS OF CARDIOMEGALY
INSTRUMENTAL INVESTIGATIONS:
Echocardiography is the most valuable non-invasive methods of diagnosis
Слайд 12MANAGEMENT OF PATIENTS WITH CARDIOMEGALY
To confirm cardiomegaly (to determine enlargement of the
MANAGEMENT OF PATIENTS WITH CARDIOMEGALY
To confirm cardiomegaly (to determine enlargement of the
Слайд 13MANAGEMENT OF PATIENTS WITH CARDIOMEGALY
ASSESSMENT OF FUNCTIONAL SIGNIFICANCE OF CARDIOMEGALY:
Symptoms of
MANAGEMENT OF PATIENTS WITH CARDIOMEGALY
ASSESSMENT OF FUNCTIONAL SIGNIFICANCE OF CARDIOMEGALY:
Symptoms of
Слайд 14MANAGEMENT OF PATIENTS WITH CARDIOMEGALY
PLANNING MANAGEMENT OF THE PATIENT:
Prevention: changing lifestyle, treatment
MANAGEMENT OF PATIENTS WITH CARDIOMEGALY
PLANNING MANAGEMENT OF THE PATIENT:
Prevention: changing lifestyle, treatment
Слайд 15CARDIOMYOPATHIES (CM)
European Society of Cardiology (ESC), 2008
“Cardiomyopathies are structural and functional myocardial
CARDIOMYOPATHIES (CM)
European Society of Cardiology (ESC), 2008 “Cardiomyopathies are structural and functional myocardial
Слайд 16CARDIOMYOPATHIES
CM phenotypes
HCM (hypertrophic CM)
DCM (dilated CM)
ARVD (arrhythmogenic right ventricular dysplasia)
RCM (restrictive
CARDIOMYOPATHIES
CM phenotypes
HCM (hypertrophic CM)
DCM (dilated CM)
ARVD (arrhythmogenic right ventricular dysplasia)
RCM (restrictive
Слайд 17ESC RECOMMENDATIONS (2008)
All CM phenotypes are divided into:
Familial (inherited, genetic)
Non-identified genetic disorder
A
ESC RECOMMENDATIONS (2008)
All CM phenotypes are divided into:
Familial (inherited, genetic)
Non-identified genetic disorder
A
Слайд 18Non-familial (acquired, non-genetic)
Idiopathic
A disease subgroup
Toxic CM
Endocrine CM
Alimentary (nutritional) CM (thiamine
Idiopathic
A disease subgroup
Toxic CM
Endocrine CM
Alimentary (nutritional) CM (thiamine
Слайд 19HYPERTROPHIC CARDIOMYOPATHY
Hypertrophic cardiomyopathy is defined by the presence of increased left ventricular
HYPERTROPHIC CARDIOMYOPATHY
Hypertrophic cardiomyopathy is defined by the presence of increased left ventricular
Слайд 20HYPERTROPHIC CARDIOMYOPATHY
2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy
HCM is
HYPERTROPHIC CARDIOMYOPATHY
2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy
HCM is
Слайд 21HYPERTROPHIC CARDIOMYOPATHY
HCM is the main cause of
sudden cardiac death (SCD)
in
HYPERTROPHIC CARDIOMYOPATHY
HCM is the main cause of
sudden cardiac death (SCD)
in
Слайд 22HYPERTROPHIC CARDIOMYOPATHY
HCM is characterised by considerable (more than 15 mm) hypertrophy of
HYPERTROPHIC CARDIOMYOPATHY
HCM is characterised by considerable (more than 15 mm) hypertrophy of
Слайд 23HYPERTROPHIC CARDIOMYOPATHY
HYPERTROPHIC CARDIOMYOPATHY
Слайд 24HYPERTROPHIC CARDIOMYOPATHY
HYPERTROPHIC CARDIOMYOPATHY
Слайд 25HYPERTROPHIC CARDIOMYOPATHY
HYPERTROPHIC CARDIOMYOPATHY
Слайд 26HYPERTROPHIC CARDIOMYOPATHY
HYPERTROPHIC CARDIOMYOPATHY
Слайд 27HYPERTROPHIC CARDIOMYOPATHY
Pathogenesis of HCM includes 4 interrelated processes:
Left ventricular outflow tract obstruction
HYPERTROPHIC CARDIOMYOPATHY
Pathogenesis of HCM includes 4 interrelated processes:
Left ventricular outflow tract obstruction
Слайд 28HYPERTROPHIC CARDIOMYOPATHY
CLINICAL MANIFESTATION:
Asymptomatic course in 25% cases
Dyspnoea on exertion (90%), orthopnoea;
Angina (70-80%);
Syncope
HYPERTROPHIC CARDIOMYOPATHY
CLINICAL MANIFESTATION:
Asymptomatic course in 25% cases
Dyspnoea on exertion (90%), orthopnoea;
Angina (70-80%);
Syncope
Слайд 29HYPERTROPHIC CARDIOMYOPATHY
ON EXAMINATION:
intense, raised cardiac impulse shifted slightly to the left
double, triple
HYPERTROPHIC CARDIOMYOPATHY
ON EXAMINATION:
intense, raised cardiac impulse shifted slightly to the left
double, triple
Слайд 30HYPERTROPHIC CARDIOMYOPATHY
DIAGNOSIS:
DNA-diagnosis using polymerase chain reaction (PSR)
Genetic testing of relations in
HYPERTROPHIC CARDIOMYOPATHY
DIAGNOSIS:
DNA-diagnosis using polymerase chain reaction (PSR)
Genetic testing of relations in
Слайд 31HYPERTROPHIC CARDIOMYOPATHY
HYPERTROPHIC CARDIOMYOPATHY
Слайд 32HYPERTROPHIC CARDIOMYOPATHY
Left ventricular wall or IVS thickness >15 mm
HYPERTROPHIC CARDIOMYOPATHY
Left ventricular wall or IVS thickness >15 mm
Слайд 33HYPERTROPHIC CARDIOMYOPATHY
MEDICAL TREATMENT:
ß-blockers
Increase diastolic filling/relaxation of the LV
Are first choice in
HYPERTROPHIC CARDIOMYOPATHY
MEDICAL TREATMENT:
ß-blockers
Increase diastolic filling/relaxation of the LV
Are first choice in
Слайд 34HYPERTROPHIC CARDIOMYOPATHY
Invasive methods of HCM management
Transaortic septal myectomy (Morrow’s procedure)
is a
HYPERTROPHIC CARDIOMYOPATHY
Invasive methods of HCM management
Transaortic septal myectomy (Morrow’s procedure)
is a
Слайд 35HYPERTROPHIC CARDIOMYOPATHY
Percutaneous transluminal septal alcohol ablation
May be chosen for highly symptomatic adult
HYPERTROPHIC CARDIOMYOPATHY
Percutaneous transluminal septal alcohol ablation
May be chosen for highly symptomatic adult
Слайд 36DILATED CARDIOMYOPATHY (DCM)
Is a disease of the cardiac muscle characterised by dilation
DILATED CARDIOMYOPATHY (DCM)
Is a disease of the cardiac muscle characterised by dilation
Слайд 37DILATED CARDIOMYOPATHY
Dilated cardiomyopathy is responsible for 9% of all cases of heart
DILATED CARDIOMYOPATHY
Dilated cardiomyopathy is responsible for 9% of all cases of heart
Слайд 38CLINICAL MANIFESTATIONS OF DCM
Symptoms: palpitation, syncopes, weakness, dyspnoea, reduced exercise tolerance and
CLINICAL MANIFESTATIONS OF DCM
Symptoms: palpitation, syncopes, weakness, dyspnoea, reduced exercise tolerance and
Слайд 39CLINICAL MANIFESTATIONS OF DCM
Physical changes
Inspection, palpation:
Swollen, pulsating jugular veins
Diffuse apical pulse shifted
CLINICAL MANIFESTATIONS OF DCM
Physical changes
Inspection, palpation:
Swollen, pulsating jugular veins
Diffuse apical pulse shifted
Слайд 40DIAGNOSIS OF DCM
ECG: no specific changes
- Ventricular arrhythmia
- Atrial fibrillation
- Impaired contractility
-
DIAGNOSIS OF DCM
ECG: no specific changes
- Ventricular arrhythmia
- Atrial fibrillation
- Impaired contractility
-
Слайд 41DIAGNOSIS OF DCM
Cardiomegaly (cardiothoracic ratio > 50%)
Pulmonary congestion
DIAGNOSIS OF DCM
Cardiomegaly (cardiothoracic ratio > 50%)
Pulmonary congestion
Слайд 42DIAGNOSIS OF DCM
Dilation of heart cavities
EF < 40%
Sings of pulmonary hypertension
Hypokinesis of
DIAGNOSIS OF DCM
Dilation of heart cavities
EF < 40%
Sings of pulmonary hypertension
Hypokinesis of
Слайд 43DIAGNOSIS OF DCM
Radionuclide methods
Can be used to assess the size of
DIAGNOSIS OF DCM
Radionuclide methods
Can be used to assess the size of
Слайд 44EXCLUSION CRITERIA FOR DCM
Systemic arterial hypertension (> 160/100 mm Hg)
Ischaemic heart
EXCLUSION CRITERIA FOR DCM
Systemic arterial hypertension (> 160/100 mm Hg)
Ischaemic heart
Слайд 45MANAGEMENT OF DCM
To exclude factors which may worsen dysfunction of myocardium
Medical treatment:
Management
MANAGEMENT OF DCM
To exclude factors which may worsen dysfunction of myocardium
Medical treatment:
Management
Слайд 46MYOCARDITIS
Inflammatory impairment of the heart muscle due to influence (direct or indirect
MYOCARDITIS
Inflammatory impairment of the heart muscle due to influence (direct or indirect
Слайд 47ETIOLOGY OF MYOCARDITIS
Bacteria
Rickettsiae and Spirochaete
Viruses
Protozoa
Fungi
Parasitic diseases
Deficiencies (hypophosphataemia, hypomagnesemia, hypocalcaemia, carnitine or selenium
ETIOLOGY OF MYOCARDITIS
Bacteria
Rickettsiae and Spirochaete
Viruses
Protozoa
Fungi
Parasitic diseases
Deficiencies (hypophosphataemia, hypomagnesemia, hypocalcaemia, carnitine or selenium
Слайд 48VIRAL INFECTION IN MYOCARDITIS
Coxsackie of A and B groups, ЕСНО, A and
VIRAL INFECTION IN MYOCARDITIS
Coxsackie of A and B groups, ЕСНО, A and
Слайд 49MYOCARDITIS
THE COURSE OF THE DISEASE
Mild: mostly focal, without cavity dilation, systolic dysfunction,
MYOCARDITIS
THE COURSE OF THE DISEASE
Mild: mostly focal, without cavity dilation, systolic dysfunction,
Слайд 50DIAGNOSIS OF MYOCARDITIS
1 CRITERIA OF INFLAMMATION, INFECTION:
Fatigue, hyperthermia, accelerated ESR, leucocytosis,
DIAGNOSIS OF MYOCARDITIS
1 CRITERIA OF INFLAMMATION, INFECTION:
Fatigue, hyperthermia, accelerated ESR, leucocytosis,
Слайд 51DIAGNOSIS OF MYOCARDITIS
2 CRITERIA OF MYOCARDIAL INVOLVEMENT:
Clinical: cardialgia, heart palpitations, irregular heart
DIAGNOSIS OF MYOCARDITIS
2 CRITERIA OF MYOCARDIAL INVOLVEMENT:
Clinical: cardialgia, heart palpitations, irregular heart
Слайд 52DIAGNOSIS OF MYOCARDITIS
New York Heart Association (NYHA)
History of infection confirmed clinically and
DIAGNOSIS OF MYOCARDITIS
New York Heart Association (NYHA)
History of infection confirmed clinically and
Слайд 53MANAGEMENT OF MYOCARDITIS
1 Etiotropic treatment
Antibacterial, antiviral, antiparasitic drugs
2 Pathogenic treatment
Non-steroidal anti-inflammatory drugs
MANAGEMENT OF MYOCARDITIS
1 Etiotropic treatment
Antibacterial, antiviral, antiparasitic drugs
2 Pathogenic treatment
Non-steroidal anti-inflammatory drugs
Слайд 54HF is a clinical syndrome characterized by typical symptoms (e.g. breathlessness, ankle
HF is a clinical syndrome characterized by typical symptoms (e.g. breathlessness, ankle
Слайд 55A state in which the heart cannot provide sufficient cardiac output to
A state in which the heart cannot provide sufficient cardiac output to
Слайд 56HF – is an imprecise term used to describe the pathological state
HF – is an imprecise term used to describe the pathological state
Слайд 57CLASSIFICATION
Heart failure can be classified in several ways 1 - Acute and
CLASSIFICATION
Heart failure can be classified in several ways 1 - Acute and
Слайд 58ACCF/AHA stages of HF
Stage A: At high risk for HF but without
ACCF/AHA stages of HF
Stage A: At high risk for HF but without
Слайд 59ESC Guidelines for diagnostic and treatment of acute and chronic HF (2016)
Definition
ESC Guidelines for diagnostic and treatment of acute and chronic HF (2016)
Definition
Слайд 60NEW YORK НЕАRT ASSOCIATION (NYHA) FUNCTIONAL CLASSIFICATION OF CHF
I class. Patients with
NEW YORK НЕАRT ASSOCIATION (NYHA) FUNCTIONAL CLASSIFICATION OF CHF
I class. Patients with
Слайд 61MANAGEMENT OF
HEART FAILURE (HF)
The main purposes:
To reduce mortality !!!
To relieve HF
MANAGEMENT OF
HEART FAILURE (HF)
The main purposes:
To reduce mortality !!!
To relieve HF
Слайд 62THE MAIN PRINCIPLES OF
HF MANAGEMENT
To reveal and exclude triggering factors
To
THE MAIN PRINCIPLES OF
HF MANAGEMENT
To reveal and exclude triggering factors
To
Слайд 63METHODS OF HF MANAGEMENT
Non-medical (changing lifestyle)
Pharmacotherapy (ACE inhibitors or ARBs, beta-blockers, aldosterone
METHODS OF HF MANAGEMENT
Non-medical (changing lifestyle)
Pharmacotherapy (ACE inhibitors or ARBs, beta-blockers, aldosterone
Слайд 64Pharmacotherapy for HF
1 DRUGS PROVED TO BE ABLE TO REDUCE MORBIDITY AND
Pharmacotherapy for HF
1 DRUGS PROVED TO BE ABLE TO REDUCE MORBIDITY AND
Слайд 65ACE inhibitors recommended
by Russian Cardiology Society
Enalapril 2,5×2 - 20×2
Captopril 6,25×3 -
ACE inhibitors recommended
by Russian Cardiology Society
Enalapril 2,5×2 - 20×2
Captopril 6,25×3 -
Слайд 66RULES FOR ADMINISTRATION OF ACE INHIBITORS
To discontinue active diuretic therapy or to
RULES FOR ADMINISTRATION OF ACE INHIBITORS
To discontinue active diuretic therapy or to
Слайд 67ESC recommendations.
ARBs II with proved influence on prognosis
Candesartan from 4-8 mg daily
ESC recommendations.
ARBs II with proved influence on prognosis
Candesartan from 4-8 mg daily
Слайд 68ESC recommendations.
β-blockers with proved influence on prognosis
Bisoprolol
from 1.25 mg daily to 10
ESC recommendations.
β-blockers with proved influence on prognosis
Bisoprolol
from 1.25 mg daily to 10
Слайд 69Peculiarities of taking ß-blockers
To all patients with manifestations of CHF due to
Peculiarities of taking ß-blockers
To all patients with manifestations of CHF due to
Слайд 70ESC recommendations.
Aldosterone antagonists
Eplerenone
from 25 mg daily to 50 mg daily
Spironolactone
from
ESC recommendations.
Aldosterone antagonists
Eplerenone
from 25 mg daily to 50 mg daily
Spironolactone
from
Слайд 71ESC recommendations.
Aldosterone antagonists
Contraindicated:
K level >5.0 mmol/L, creatinine >220 mcmol/L,
While taking
ESC recommendations.
Aldosterone antagonists
Contraindicated:
K level >5.0 mmol/L, creatinine >220 mcmol/L,
While taking
Слайд 72IVABRADIN, a standard medication for CHF management
Reviewing European recommendations on HF (2012):
Ivabradin
IVABRADIN, a standard medication for CHF management
Reviewing European recommendations on HF (2012):
Ivabradin
Слайд 73Indications for administration of diuretics:
To eliminate clinical symptoms of fluid retention. They
Indications for administration of diuretics:
To eliminate clinical symptoms of fluid retention. They
Слайд 74Doses of diuretics during active stage of HF treatment
Furosemide from 20–40 mg
Doses of diuretics during active stage of HF treatment
Furosemide from 20–40 mg
 Уход за больными терапевтического и хирургического профиля
Уход за больными терапевтического и хирургического профиля Хроническое системное венерическое инфекционное заболевание сифилис
Хроническое системное венерическое инфекционное заболевание сифилис Деятельность медицинской сестры при выполнении различных видов физиотерапевтических процедур
Деятельность медицинской сестры при выполнении различных видов физиотерапевтических процедур Каждому муниципалитету – маршрут здоровья
Каждому муниципалитету – маршрут здоровья Принципы терапии новой коронавирусной инфекции COVID - 19
Принципы терапии новой коронавирусной инфекции COVID - 19 Первая помощь при тепловом и солнечном ударах
Первая помощь при тепловом и солнечном ударах Науқас 30 жаста. Психиатриялық ауруханаға бірінші рет туыстарының жетелеуімен келді
Науқас 30 жаста. Психиатриялық ауруханаға бірінші рет туыстарының жетелеуімен келді Хирургическая инфекция. Особенности обследования пациента
Хирургическая инфекция. Особенности обследования пациента ВИЧ-инфекция
ВИЧ-инфекция Эндокринная система человека. Лекция 26
Эндокринная система человека. Лекция 26 Домашняя аптечка
Домашняя аптечка Патофизиология почек
Патофизиология почек Mouse GBM: A Pilot Collection on NBIA
Mouse GBM: A Pilot Collection on NBIA Роль и функции акушерки при оказании первичной реанимационной помощи новорождённому в родильном зале
Роль и функции акушерки при оказании первичной реанимационной помощи новорождённому в родильном зале Правила остановки артериального кровотечения
Правила остановки артериального кровотечения Двигательные режимы, периоды в ЛФК
Двигательные режимы, периоды в ЛФК Патофизиология водно-солевого обмена
Патофизиология водно-солевого обмена Профилактика сердечно-сосудистых заболеваний
Профилактика сердечно-сосудистых заболеваний Пластическая хирургия
Пластическая хирургия Регургитации на клапанах
Регургитации на клапанах Сердечно легочная реанимация
Сердечно легочная реанимация Сердечно-легочная реанимация
Сердечно-легочная реанимация Teeth anatomy and dental diseases
Teeth anatomy and dental diseases Корь, краснуха, скарлатина
Корь, краснуха, скарлатина Желчный пузырь
Желчный пузырь Организация диспансерного наблюдения за детьми раннего возраста. Критерии эффективности
Организация диспансерного наблюдения за детьми раннего возраста. Критерии эффективности Правила выписывания таблеток
Правила выписывания таблеток Эндоваскулярная хирургия
Эндоваскулярная хирургия