- Pathology of the exocrine pancreas

Содержание
- 2. EXOCRINE PANCREAS
- 3. OBJECTIVES Understand the aetiology Risk factors, Pathogenesis, Morphology, Clinical features and Outcome of pancreatic inflammations and
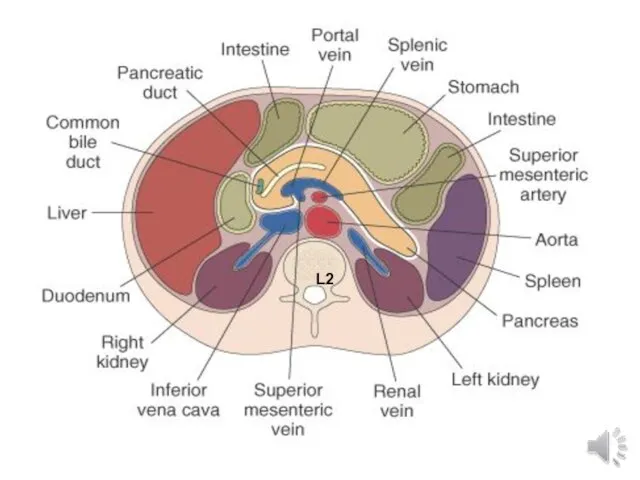
- 4. L2
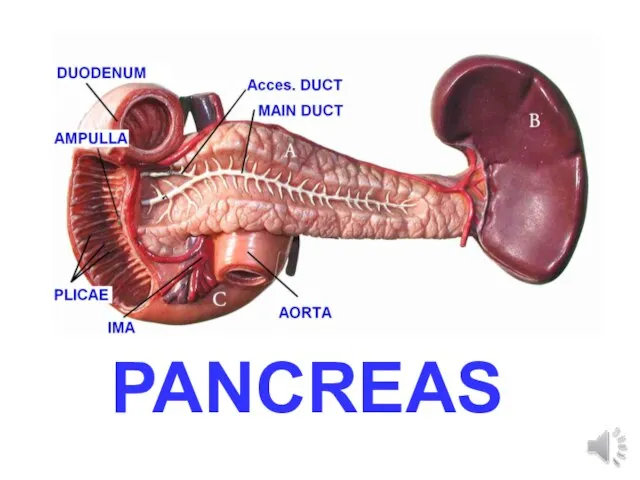
- 5. PANCREAS
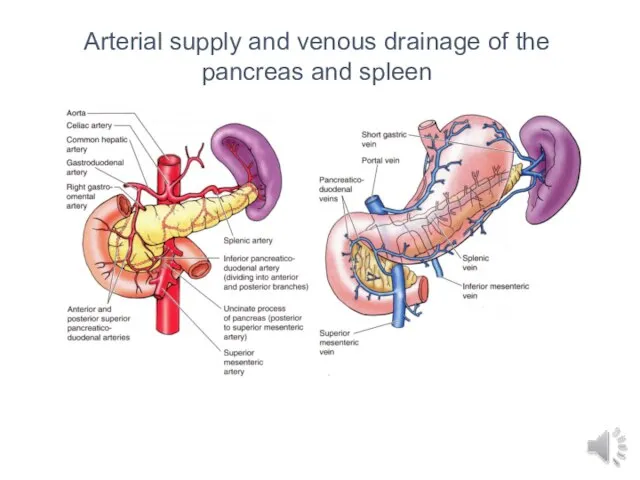
- 6. Arterial supply and venous drainage of the pancreas and spleen
- 7. Lymphatic drainage of the distal pancreas and spleen “Peri-”pancreatic lymph nodes, several groups.
- 9. Hepaticopancreatic ampulla (Ampulla of Vater)
- 10. Pancreatic Enzymes Amylase Lipase DNA-ase RNA-ase Zymogens: Trypsinogen Chymotrypsinogen Procarboxypeptidase A, B
- 11. PANCREAS DISEASES Congenital Inflammatory Acute Chronic Cysts Neoplasms
- 12. Congenital Agenesis (very rare) Annular Pancreas (pancreas encircles duodenum) (rare) Pancreas Divisum (failure of 2 ducts
- 13. PANCREATITIS ACUTE (VERY SERIOUS) CHRONIC (Calcifications, Pseudocyst)
- 14. ACUTE PANCREATITIS Idiopathic: Gallstones (45%) Ethanol (35%) Tumours: pancreas, ampulla, Scorpion stings Microbiological .bacterial: .viral: (mumps,
- 15. GALL STONES MUMPS VIRUS COMMON CAUSES OF PANCREATITIS PANCREATITIS
- 16. Pathogenesis Activation of proteolytic enzymes within pancreatic cells, starting with trypsin, leading to local and systemic
- 17. MORPHOLOGY OEDEMA FAT NECROSIS “SAPONIFICATION” ACUTE INFLAMMATORY INFILTRATE PANCREAS AUTODIGESTION BLOOD VESSEL DESTRUCTION
- 21. CLINICAL FEATURES • Pain: epigastric, noncolicky, constant can radiate to back • May improve when leaning
- 22. Repeated episodes of clinically evident acute pancreatitis Common cause is alcohol Autoimmune pancreatitis Cystic fibrosis Familial
- 23. CLINICAL FEATURES Abdominal Pain Vague abdominal symptoms chronic diarrhea(mal absorption) DM pseudocysts amylase elevated, or normal
- 24. Investigations • laboratory: . increase in serum glucose . increase in serum ALP, less commonly bilirubin
- 25. Management • pain, difficult to control • general management: . total abstinence from alcohol . enzyme
- 27. Cysts & Cystic tumours Pancreatic cysts are of two types True cysts which are lined by
- 28. ACUTE PANCREATITIS CHRONIC PANCREATITIS SYSTEMIC ORGAN FAILURE SHOCK ARDS ARF DIC PANCRATIC ABCESSES PANCREATIC PSEUDOCYST DOUDENAL
- 29. CARCINOMA OF THE PANCREAS USUALLY ADENOCARCINOMA MAY PRESENT WITH OBSTRUCTIVE JAUNDICE VERY POOR PROGNOSIS AETIOLOGY CIGARETTE
- 30. CLINICOPATHOLOGICAL FEATURES MOST ARE ADENOCARCINOMA MOST COMMONLY ARISE IN THE HEAD OF THE PANCREAS COMPRESS THE
- 31. Pancreatic Adenocarcinoma
- 32. REMEMBER Painless jaundice in an elderly person is CARCINOMA of the head of the pancreas until
- 34. Скачать презентацию

Слайд 3OBJECTIVES
Understand the aetiology
Risk factors,
Pathogenesis,
Morphology,
Clinical features and
Outcome of pancreatic
OBJECTIVES
Understand the aetiology
Risk factors,
Pathogenesis,
Morphology,
Clinical features and
Outcome of pancreatic
Слайд 4L2
L2
Слайд 5PANCREAS
PANCREAS
Слайд 6Arterial supply and venous drainage of the pancreas and spleen
Arterial supply and venous drainage of the pancreas and spleen
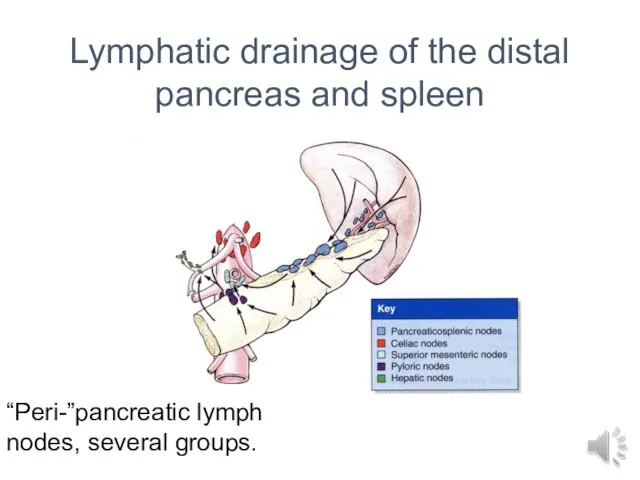
Слайд 7Lymphatic drainage of the distal pancreas and spleen
“Peri-”pancreatic lymph nodes, several groups.
Lymphatic drainage of the distal pancreas and spleen
“Peri-”pancreatic lymph nodes, several groups.
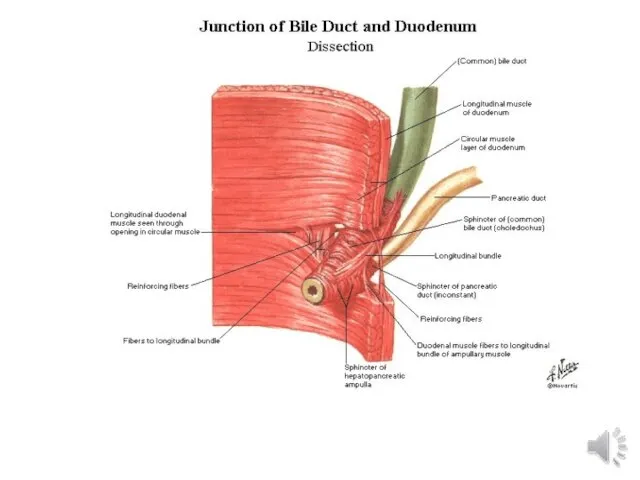
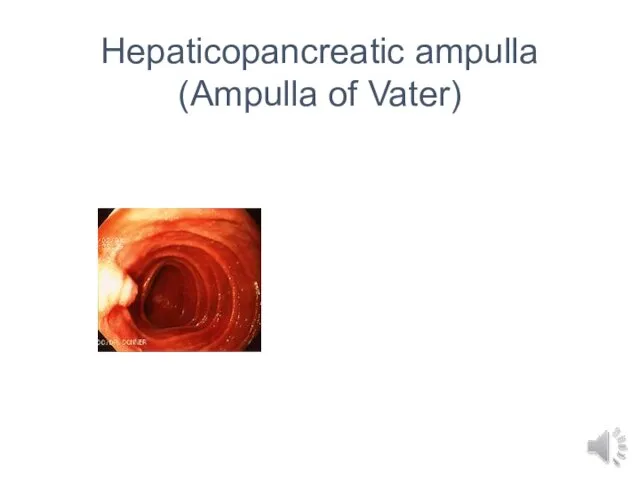
Слайд 9Hepaticopancreatic ampulla
(Ampulla of Vater)
Hepaticopancreatic ampulla
(Ampulla of Vater)
Слайд 10Pancreatic Enzymes
Amylase
Lipase
DNA-ase
RNA-ase
Zymogens: Trypsinogen Chymotrypsinogen Procarboxypeptidase A, B
Pancreatic Enzymes
Amylase
Lipase
DNA-ase
RNA-ase
Zymogens: Trypsinogen Chymotrypsinogen Procarboxypeptidase A, B
Слайд 11PANCREAS DISEASES
Congenital
Inflammatory
Acute
Chronic
Cysts
Neoplasms
PANCREAS DISEASES
Congenital
Inflammatory
Acute
Chronic
Cysts
Neoplasms
Слайд 12Congenital
Agenesis (very rare)
Annular Pancreas (pancreas encircles duodenum) (rare)
Pancreas Divisum (failure of 2
Congenital
Agenesis (very rare)
Annular Pancreas (pancreas encircles duodenum) (rare)
Pancreas Divisum (failure of 2
Слайд 13PANCREATITIS
ACUTE (VERY SERIOUS)
CHRONIC (Calcifications, Pseudocyst)
PANCREATITIS
ACUTE (VERY SERIOUS)
CHRONIC (Calcifications, Pseudocyst)
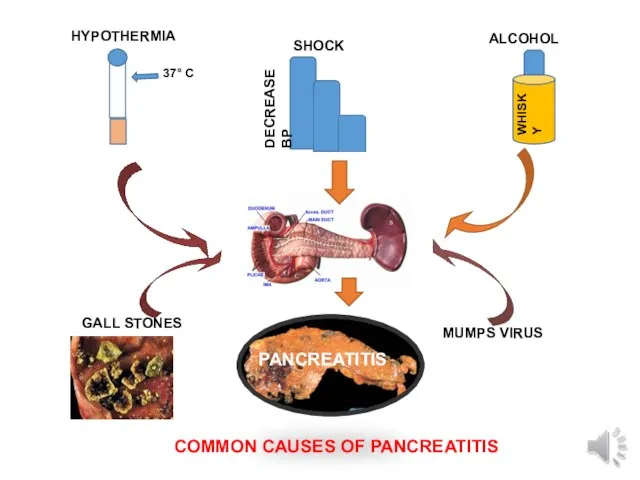
Слайд 14ACUTE PANCREATITIS
Idiopathic:
Gallstones (45%)
Ethanol (35%)
Tumours: pancreas, ampulla,
Scorpion stings
Microbiological .bacterial: .viral: (mumps,
ACUTE PANCREATITIS
Idiopathic:
Gallstones (45%)
Ethanol (35%)
Tumours: pancreas, ampulla,
Scorpion stings
Microbiological .bacterial: .viral: (mumps,
Слайд 15GALL STONES
MUMPS VIRUS
COMMON CAUSES OF PANCREATITIS
PANCREATITIS
GALL STONES
MUMPS VIRUS
COMMON CAUSES OF PANCREATITIS
PANCREATITIS
Слайд 16Pathogenesis
Activation of proteolytic enzymes within pancreatic cells, starting with trypsin, leading
Pathogenesis
Activation of proteolytic enzymes within pancreatic cells, starting with trypsin, leading
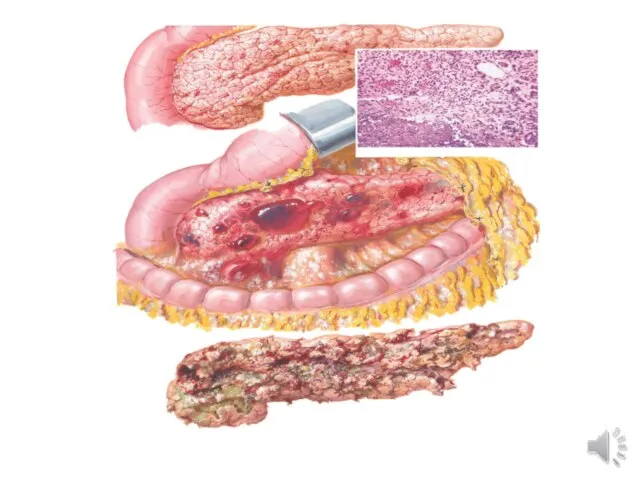
Слайд 17MORPHOLOGY
OEDEMA
FAT NECROSIS
“SAPONIFICATION”
ACUTE INFLAMMATORY INFILTRATE
PANCREAS AUTODIGESTION
BLOOD VESSEL DESTRUCTION
MORPHOLOGY
OEDEMA
FAT NECROSIS
“SAPONIFICATION”
ACUTE INFLAMMATORY INFILTRATE
PANCREAS AUTODIGESTION
BLOOD VESSEL DESTRUCTION


Слайд 21CLINICAL FEATURES
• Pain: epigastric, noncolicky, constant can radiate to back
• May improve
CLINICAL FEATURES
• Pain: epigastric, noncolicky, constant can radiate to back
• May improve
Слайд 22Repeated episodes of clinically evident acute pancreatitis
Common cause is alcohol
Autoimmune pancreatitis
Cystic
Repeated episodes of clinically evident acute pancreatitis
Common cause is alcohol
Autoimmune pancreatitis
Cystic
Слайд 23CLINICAL FEATURES
Abdominal Pain
Vague abdominal symptoms
chronic diarrhea(mal absorption)
DM
pseudocysts
amylase elevated, or normal
CLINICAL FEATURES
Abdominal Pain
Vague abdominal symptoms
chronic diarrhea(mal absorption)
DM
pseudocysts
amylase elevated, or normal
Слайд 24Investigations
• laboratory:
. increase in serum glucose
. increase in serum ALP, less commonly
Investigations
• laboratory:
. increase in serum glucose
. increase in serum ALP, less commonly
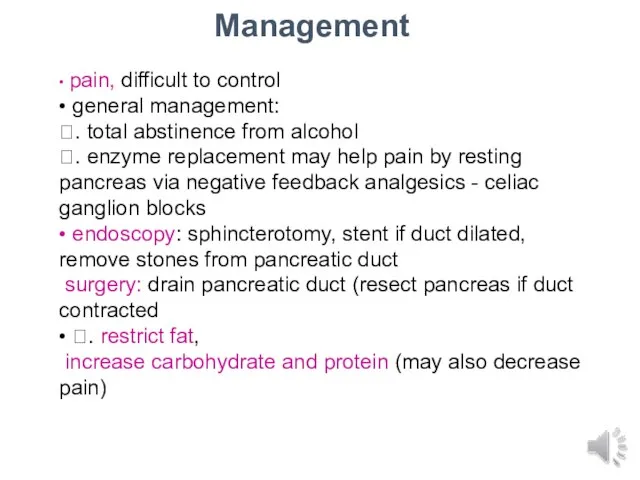
Слайд 25Management
• pain, difficult to control
• general management:
. total abstinence from alcohol
. enzyme
Management
• pain, difficult to control
• general management:
. total abstinence from alcohol
. enzyme
Слайд 27Cysts & Cystic tumours
Pancreatic cysts are of two types
True cysts which are
Cysts & Cystic tumours
Pancreatic cysts are of two types
True cysts which are
Слайд 28ACUTE PANCREATITIS
CHRONIC PANCREATITIS
SYSTEMIC ORGAN FAILURE
SHOCK
ARDS
ARF
DIC
PANCRATIC ABCESSES
PANCREATIC PSEUDOCYST
DOUDENAL OBSTRUCTION
PSEUDOCYST
DUCT OBSTRUCTION
MALABSORPTION STEATORRHEA
SECONDARY DIABETES
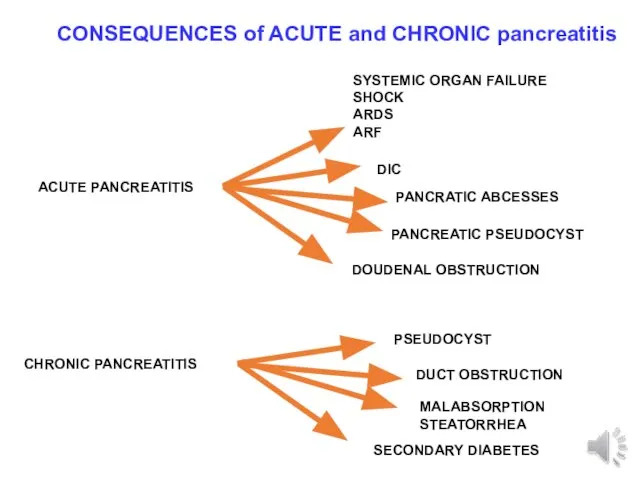
CONSEQUENCES of
ACUTE PANCREATITIS
CHRONIC PANCREATITIS
SYSTEMIC ORGAN FAILURE
SHOCK
ARDS
ARF
DIC
PANCRATIC ABCESSES
PANCREATIC PSEUDOCYST
DOUDENAL OBSTRUCTION
PSEUDOCYST
DUCT OBSTRUCTION
MALABSORPTION STEATORRHEA
SECONDARY DIABETES
CONSEQUENCES of
Слайд 29CARCINOMA OF THE PANCREAS
USUALLY ADENOCARCINOMA
MAY PRESENT WITH OBSTRUCTIVE JAUNDICE
VERY POOR PROGNOSIS
AETIOLOGY
CIGARETTE SMOKING
DM
FAMILIAL
CARCINOMA OF THE PANCREAS
USUALLY ADENOCARCINOMA
MAY PRESENT WITH OBSTRUCTIVE JAUNDICE
VERY POOR PROGNOSIS
AETIOLOGY
CIGARETTE SMOKING
DM
FAMILIAL
Слайд 30CLINICOPATHOLOGICAL FEATURES
MOST ARE ADENOCARCINOMA
MOST COMMONLY ARISE IN THE HEAD OF THE
CLINICOPATHOLOGICAL FEATURES
MOST ARE ADENOCARCINOMA
MOST COMMONLY ARISE IN THE HEAD OF THE
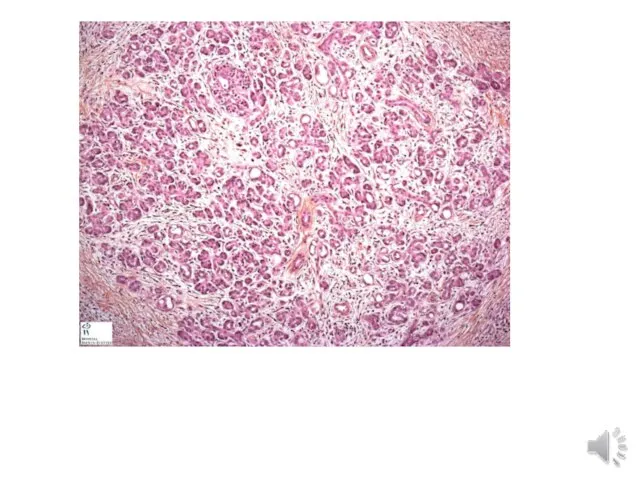
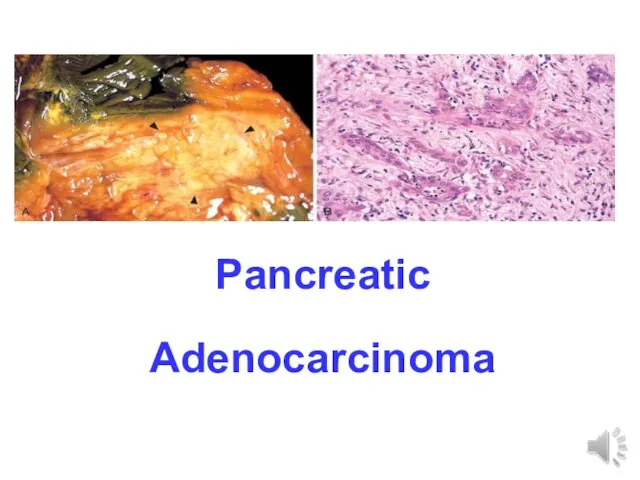
Слайд 31Pancreatic
Adenocarcinoma
Pancreatic
Adenocarcinoma
Слайд 32REMEMBER
Painless jaundice in an elderly person is CARCINOMA of the head of
REMEMBER
Painless jaundice in an elderly person is CARCINOMA of the head of
 reabilitatsia_zabolevaniy_organov_dykhania (1)
reabilitatsia_zabolevaniy_organov_dykhania (1) Ультразвуковая допплерография в стоматологии
Ультразвуковая допплерография в стоматологии Депрессия (от латинского слова depressio - подавление)
Депрессия (от латинского слова depressio - подавление) Нарушение осанки и плоскостопие
Нарушение осанки и плоскостопие Курение как социальное зло в наше время
Курение как социальное зло в наше время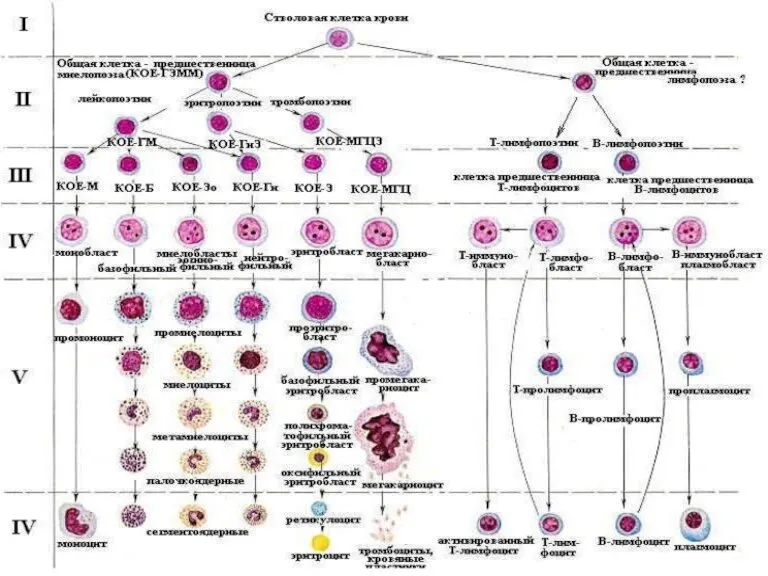 Болезни системы крови
Болезни системы крови Heart failure slideset
Heart failure slideset Хирургическая онкология
Хирургическая онкология Синдром полости в легком
Синдром полости в легком Тема Роды
Тема Роды ВИЧ и его профилактика
ВИЧ и его профилактика Принципы современной защиты от гриппа и ОРЗ и аптечные продажи
Принципы современной защиты от гриппа и ОРЗ и аптечные продажи СПИД
СПИД Цереброваскулярлы аурулар
Цереброваскулярлы аурулар Первая помощь при кровотечениях
Первая помощь при кровотечениях Чесотка. Чесоточный клещ
Чесотка. Чесоточный клещ Заболевания нервной системы и их профилактика
Заболевания нервной системы и их профилактика Клеточные элементы ликвора
Клеточные элементы ликвора Дисбиотические патологические процессы
Дисбиотические патологические процессы ВИЧ-инфекция
ВИЧ-инфекция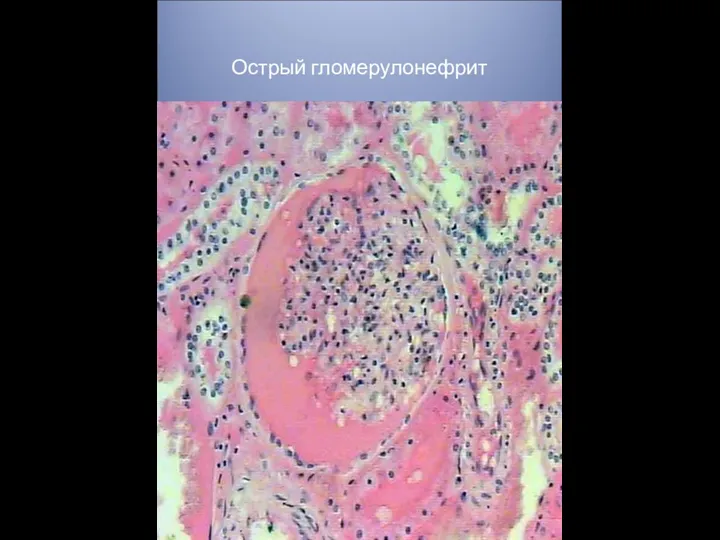 Острый гломерулонефрит
Острый гломерулонефрит Медицинские учреждения
Медицинские учреждения Травматический шок
Травматический шок Сознание
Сознание Природные антибактериальные средства
Природные антибактериальные средства Диагностика хронической недостаточности сердца
Диагностика хронической недостаточности сердца Особенности диагностики. Оказание неотложной помощи. Интенсивная терапия
Особенности диагностики. Оказание неотложной помощи. Интенсивная терапия Аналар мен балалар денсаулығын қорғау
Аналар мен балалар денсаулығын қорғау