- Abdominal Hernias. Ada Yee

Содержание
- 2. Warm up Indirect inguinal hernias are caused by weakness of the transversalis fascia Direct inguinal hernias
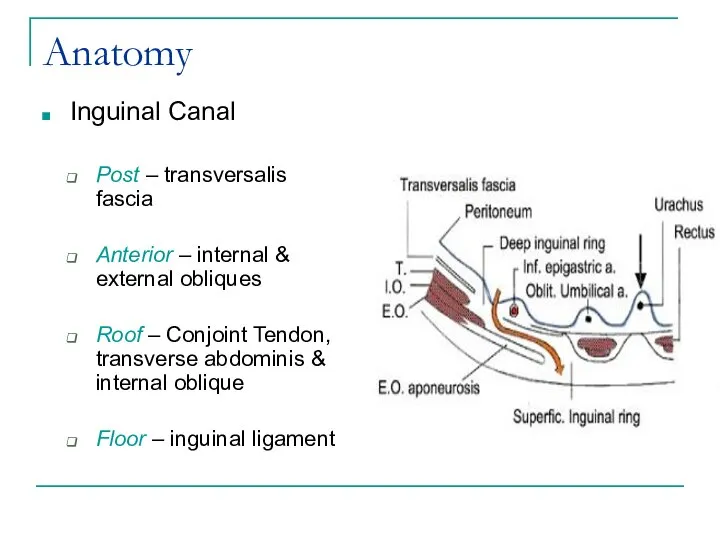
- 3. Anatomy Inguinal Canal Post – transversalis fascia Anterior – internal & external obliques Roof – Conjoint
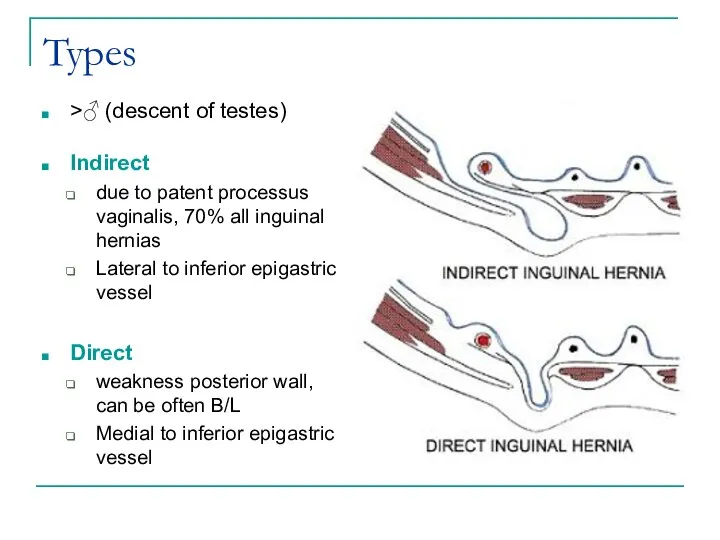
- 4. Types >♂ (descent of testes) Indirect due to patent processus vaginalis, 70% all inguinal hernias Lateral
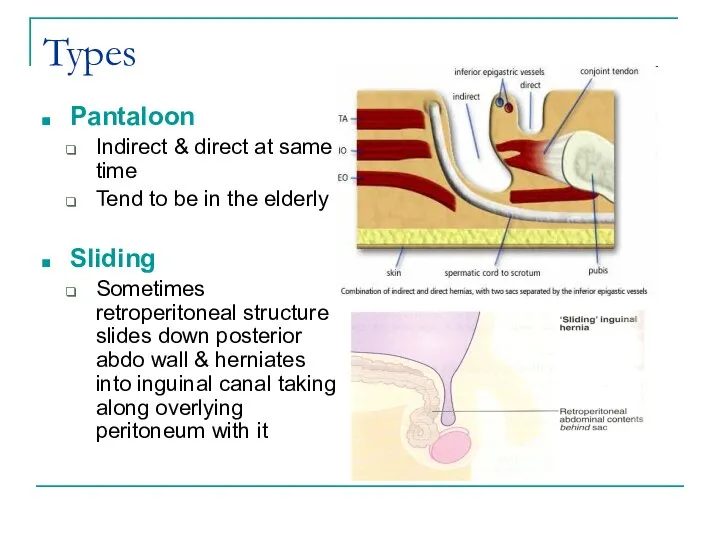
- 5. Types Pantaloon Indirect & direct at same time Tend to be in the elderly Sliding Sometimes
- 6. Types Incarcerated A chronically irreducible hernia which is not strangulated Strangled Tends to occur with indirect
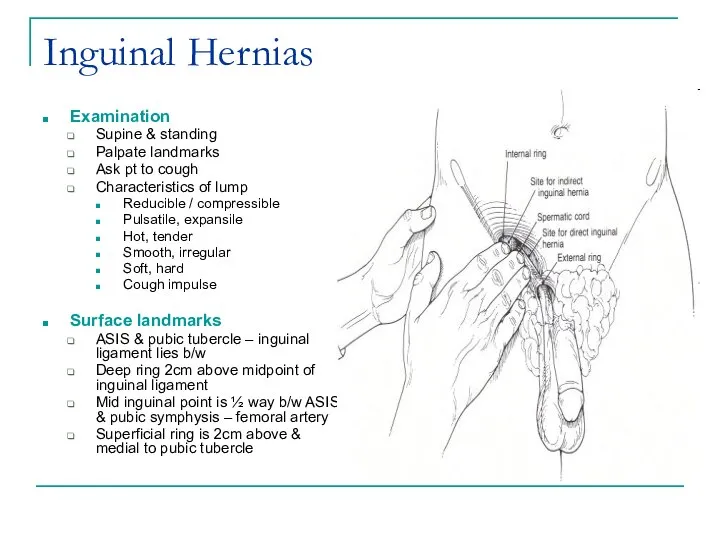
- 7. Inguinal Hernias Examination Supine & standing Palpate landmarks Ask pt to cough Characteristics of lump Reducible
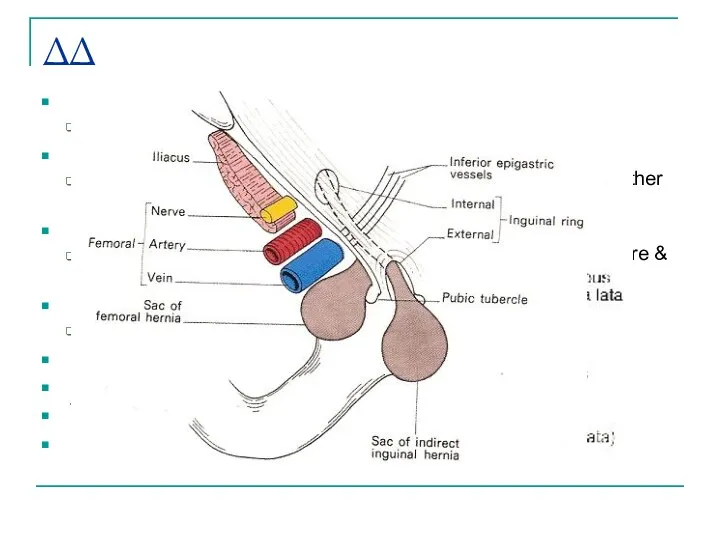
- 8. ΔΔ Femoral hernia Lie lateral & below the pubic tubercle Lymphadenopathy Mobile, pain, fever, recent infections,
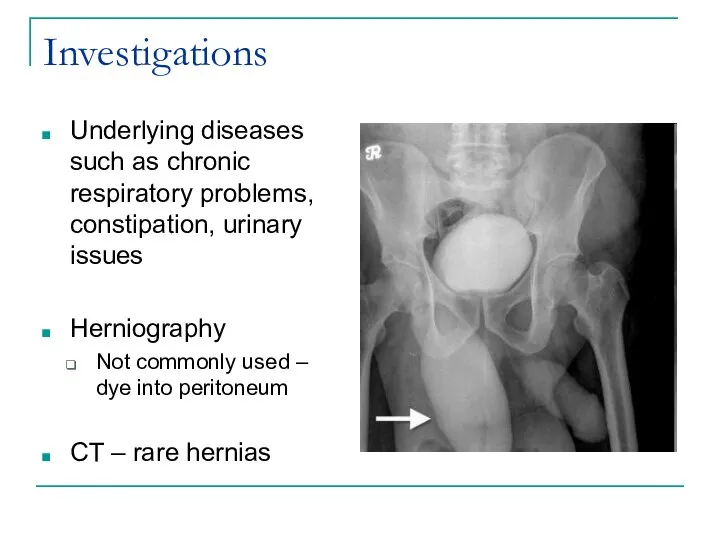
- 9. Investigations Underlying diseases such as chronic respiratory problems, constipation, urinary issues Herniography Not commonly used –
- 10. Management & Indications for Surgery
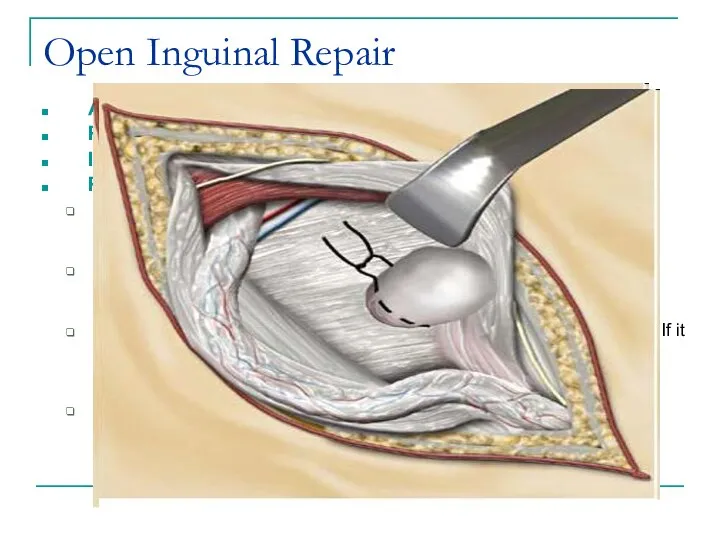
- 11. Open Inguinal Repair Anaesthesia – general, spinal, local Position - supine Incision – 2cm above &
- 12. Open Inguinal Repair Procedure cont’ Indirect sac will be identified by separating the cord structures. The
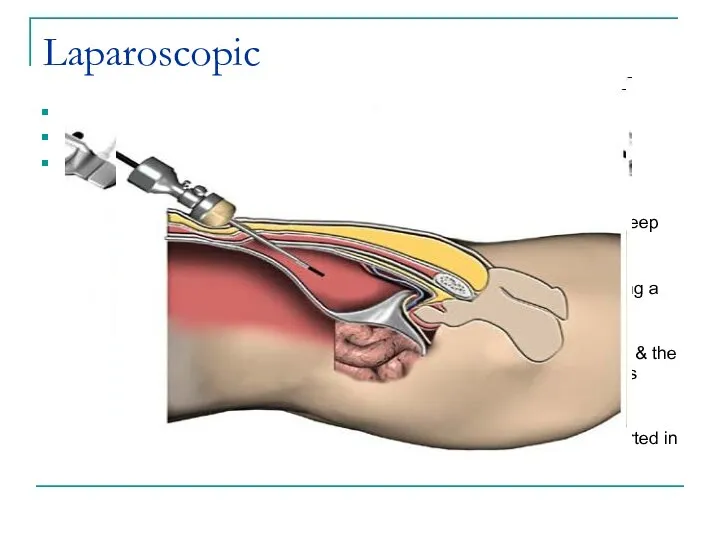
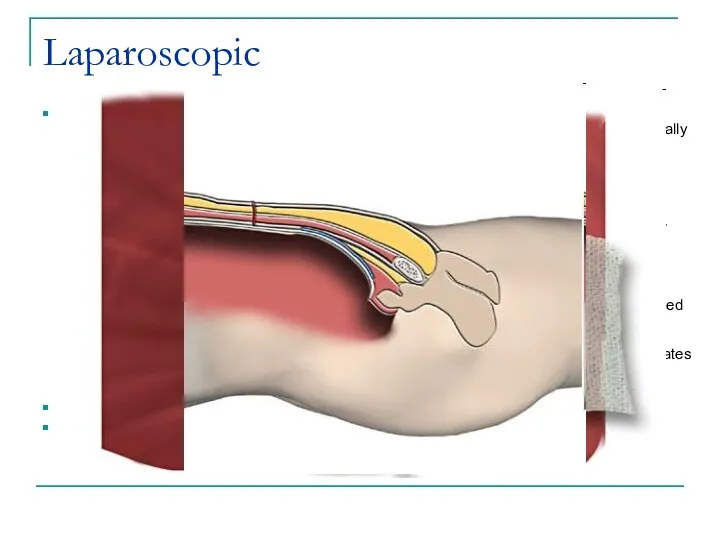
- 13. Laparoscopic Anaesthesia – general Position – supine Incision & Approach A 2 cm transverse incision is
- 14. Laparoscopic Procedure The peritoneum is separated from the abdominal wall behind the inguinal area, laterally to
- 15. Complications of Op Infection Bleeding Recurrence Urinary retention Testicular atrophy Neuropraxia / nerve entrapment
- 17. Скачать презентацию
Слайд 3Anatomy
Inguinal Canal
Post – transversalis fascia
Anterior – internal & external obliques
Roof – Conjoint
Anatomy
Inguinal Canal
Post – transversalis fascia
Anterior – internal & external obliques
Roof – Conjoint
Слайд 4Types
>♂ (descent of testes)
Indirect
due to patent processus vaginalis, 70% all inguinal
Types
>♂ (descent of testes)
Indirect
due to patent processus vaginalis, 70% all inguinal
Слайд 5Types
Pantaloon
Indirect & direct at same time
Tend to be in the elderly
Sliding
Sometimes
Types
Pantaloon
Indirect & direct at same time
Tend to be in the elderly
Sliding
Sometimes
Слайд 6Types
Incarcerated
A chronically irreducible hernia which is not strangulated
Strangled
Tends to occur with indirect
Types
Incarcerated
A chronically irreducible hernia which is not strangulated
Strangled
Tends to occur with indirect
Слайд 7Inguinal Hernias
Examination
Supine & standing
Palpate landmarks
Ask pt to cough
Characteristics of lump
Reducible /
Inguinal Hernias
Examination
Supine & standing
Palpate landmarks
Ask pt to cough
Characteristics of lump
Reducible /
Слайд 8ΔΔ
Femoral hernia
Lie lateral & below the pubic tubercle
Lymphadenopathy
Mobile, pain, fever, recent infections,
ΔΔ
Femoral hernia
Lie lateral & below the pubic tubercle
Lymphadenopathy
Mobile, pain, fever, recent infections,
Слайд 9Investigations
Underlying diseases such as chronic respiratory problems, constipation, urinary issues
Herniography
Not commonly used
Investigations
Underlying diseases such as chronic respiratory problems, constipation, urinary issues
Herniography
Not commonly used
Слайд 10Management & Indications for Surgery
Management & Indications for Surgery
Слайд 11Open Inguinal Repair
Anaesthesia – general, spinal, local
Position - supine
Incision – 2cm above
Open Inguinal Repair
Anaesthesia – general, spinal, local
Position - supine
Incision – 2cm above
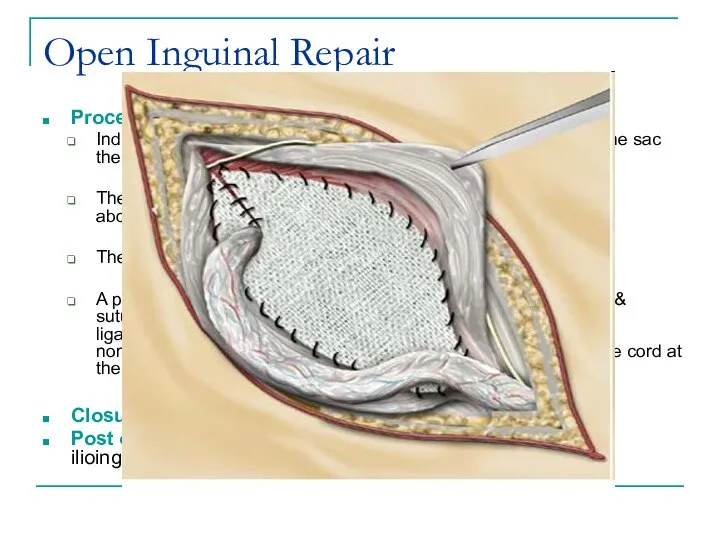
Слайд 12Open Inguinal Repair
Procedure cont’
Indirect sac will be identified by separating the cord
Open Inguinal Repair
Procedure cont’
Indirect sac will be identified by separating the cord
Слайд 13Laparoscopic
Anaesthesia – general
Position – supine
Incision & Approach
A 2 cm transverse incision is
Laparoscopic
Anaesthesia – general
Position – supine
Incision & Approach
A 2 cm transverse incision is
Слайд 14Laparoscopic
Procedure
The peritoneum is separated from the abdominal wall behind the inguinal area,
Laparoscopic
Procedure
The peritoneum is separated from the abdominal wall behind the inguinal area,
Слайд 15Complications of Op
Infection
Bleeding
Recurrence
Urinary retention
Testicular atrophy
Neuropraxia / nerve entrapment
Complications of Op
Infection
Bleeding
Recurrence
Urinary retention
Testicular atrophy
Neuropraxia / nerve entrapment
 Жасөспірім қыздарға арналған тренинг сабақ
Жасөспірім қыздарға арналған тренинг сабақ To demonstrate gastric ulser induction/formation by different methods
To demonstrate gastric ulser induction/formation by different methods Модернизация первичного звена здравоохранения Мурманской области. Терский район
Модернизация первичного звена здравоохранения Мурманской области. Терский район Радионуклидная диагностика. Лекция 3
Радионуклидная диагностика. Лекция 3 Травмы. Определение. Виды. Опасности и осложнения. Действия медсестры
Травмы. Определение. Виды. Опасности и осложнения. Действия медсестры Ревматоидный полиартрит
Ревматоидный полиартрит Инфаркт миокарда и его осложнения
Инфаркт миокарда и его осложнения Ивановский Дмитрий Иосифович - первооткрыватель вируса - табачной мозаики
Ивановский Дмитрий Иосифович - первооткрыватель вируса - табачной мозаики Право на бесплатную медицинскую помощь
Право на бесплатную медицинскую помощь Fizicheskoe_razvitie
Fizicheskoe_razvitie PRP-терапия в лечении эпикондилитов
PRP-терапия в лечении эпикондилитов Функциональная анатомия лимфатической системы
Функциональная анатомия лимфатической системы Гнійничкові захворювання шкіри. Піодермії
Гнійничкові захворювання шкіри. Піодермії Природа - найкращий лiкар
Природа - найкращий лiкар Заболевания крови
Заболевания крови Введение в гигиену
Введение в гигиену Современные методы диагностики хронических облитерирующих заболеваний артерий нижних конечностей
Современные методы диагностики хронических облитерирующих заболеваний артерий нижних конечностей Клиническая фармакология лекарственных средств, применяемых при заболеваниях желудочно-кишечного тракта (часть 1)
Клиническая фармакология лекарственных средств, применяемых при заболеваниях желудочно-кишечного тракта (часть 1) Центр медицинского массажа и косметологии
Центр медицинского массажа и косметологии Финал кейса по медицине
Финал кейса по медицине Основы маммографии
Основы маммографии 精神分裂症. Schizophrenie
精神分裂症. Schizophrenie Реабилитация больных с шейным остеохондрозом
Реабилитация больных с шейным остеохондрозом Синдро́м дли́тельного сдавле́ния
Синдро́м дли́тельного сдавле́ния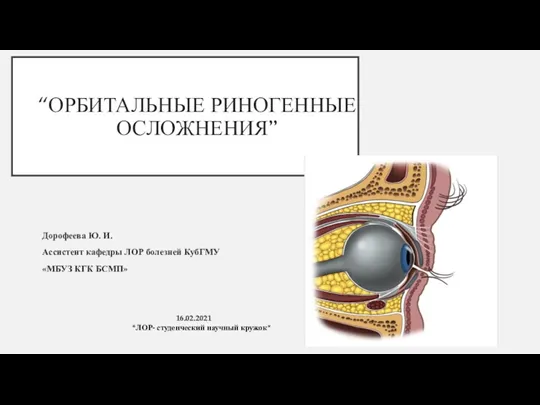 Орбитальные риногенные осложнения
Орбитальные риногенные осложнения Картотека игр на формирование правильной осанки
Картотека игр на формирование правильной осанки Синдром Клайнфельтера
Синдром Клайнфельтера DATA Program Diabetes Awareness, Training, and Action
DATA Program Diabetes Awareness, Training, and Action