- Angina pectoris

Содержание
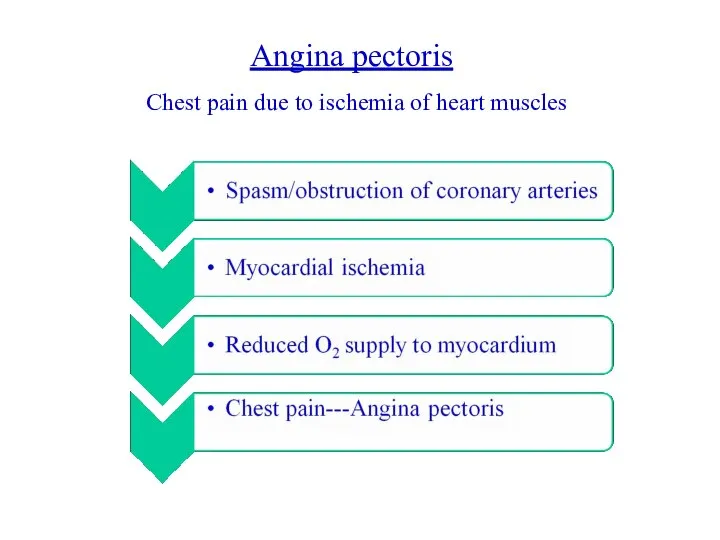
- 2. Angina pectoris Chest pain due to ischemia of heart muscles
- 3. Weak relationship between severity of pain and degree of oxygen supply- there can be severe pain
- 4. Stable angina: Also called “Effort Angina” Discomfort is precipitated by activity Minimal or no symptoms at
- 5. Unstable angina: Also called “Crescendo angina” Acute coronary syndrome in which angina worsens Occurs at rest
- 6. Microvascular angina: Also called Syndrome X Cause unknown Probably due to poor functioning of the small
- 7. Prinzmetal’s angina Prinzmetal’s angina is a variant form of angina with normal coronary vessels or minimal
- 8. Symptoms What is the cause of ischemia ? either ↑ oxygen demand or ↓ oxygen supply
- 9. Treatment: Aims: Relief of symptoms Slowing progression of the disease Reduction of future events like myocardial
- 10. Drugs: 1. For treatment of acute attacks: Organic nitrates/nitrites 2. For prophylaxis: Organic nitrates Beta blockers
- 11. ↑ Heart rate ↑ Contractility ↑ Preload ↑ Afterload ↓ Coronary flow ↓ Regional myocardial blood
- 12. Organic nitrates Pro drugs release NO ↑ Levels of intracellular cGMP Dephosphorylation of mysosin light chain
- 13. Relaxation of vascular smooth muscles- vasodilatation NO-mediated guanylyl cyclase activation inhibits platelet aggregation Relaxation of smooth
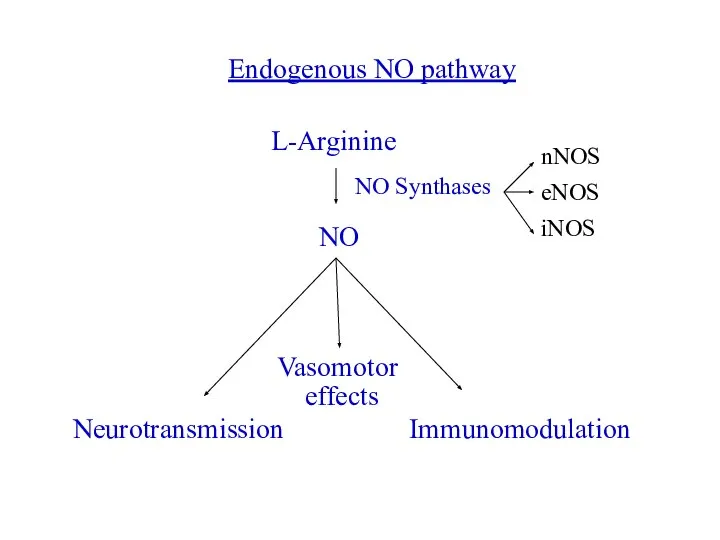
- 14. L-Arginine NO NO Synthases Neurotransmission Vasomotor effects Immunomodulation Endogenous NO pathway nNOS eNOS iNOS
- 15. Three different forms of NO synthase are found in humans: 1. Neuronal NOS (nNOS or NOS1)-
- 16. CVS Effects: Vasodilatation- low concentrations preferably dilate veins Venodilatation→ decreases venous return to heart Decreased chamber
- 17. HR-unchanged or may increase slightly (reflex tachycardia) Cardiac output slightly reduced Even low doses can cause
- 18. Coronary blood flow may initially increase transiently Subsequently, due to decreased BP, may decrease Nitrates have
- 19. Reduction in myocardial O2 consumption is caused by: Peripheral pooling of blood- reduced preload Arteriolar dilatation-
- 20. How myocardial O2 consumption can be determined? Double product: HR × systolic BP- approximate measure of
- 21. Pharmacokinetics: Orally ineffective because of high first pass metabolism Administered sublingually to avoid first pass matabolism
- 22. ADRs: Headache- may be severe May disappear after continued use or, Decrease dose Transient episodes of
- 23. Administration of nitrates: Sublingual Oral: For prophylaxis, require high doses due to first pass metabolism, isosorbide
- 24. Transdermal nitrogycerine discs impregnated with nitroglycerine polymer- gradual absorption and 24 h plasma nitrate concentration Onset
- 25. Ca2+ antagonists: ↓ Ca2+ influx Negative iono and chronotropic effects Peripheral vasodilatation Used in variant angina
- 26. β-Blockers: Effective in reducing severity and frequency of exertional angina May worsen vasospastic angina- contraindicated Reduce
- 27. Ranolazine: Reserve agent for treatment of chronic, resistant angina Inhibits cardiac late Na+ current Effects the
- 29. Скачать презентацию
Слайд 3Weak relationship between severity of pain and degree of oxygen supply- there
Weak relationship between severity of pain and degree of oxygen supply- there
Слайд 4Stable angina:
Also called “Effort Angina”
Discomfort is precipitated by activity
Minimal or no symptoms
Stable angina:
Also called “Effort Angina”
Discomfort is precipitated by activity
Minimal or no symptoms
Слайд 5Unstable angina:
Also called “Crescendo angina”
Acute coronary syndrome in which angina worsens
Occurs at
Unstable angina:
Also called “Crescendo angina”
Acute coronary syndrome in which angina worsens
Occurs at
Слайд 6Microvascular angina:
Also called Syndrome X
Cause unknown
Probably due to poor functioning of the
Microvascular angina:
Also called Syndrome X
Cause unknown
Probably due to poor functioning of the
Слайд 7Prinzmetal’s angina
Prinzmetal’s angina is a variant form of angina with normal coronary
Prinzmetal’s angina
Prinzmetal’s angina is a variant form of angina with normal coronary
Слайд 8Symptoms
What is the cause of ischemia ?
either ↑ oxygen demand or
Symptoms
What is the cause of ischemia ?
either ↑ oxygen demand or
Слайд 9Treatment:
Aims:
Relief of symptoms
Slowing progression of the disease
Reduction of future events like myocardial
Treatment:
Aims:
Relief of symptoms
Slowing progression of the disease
Reduction of future events like myocardial
Слайд 10Drugs:
1. For treatment of acute attacks:
Organic nitrates/nitrites
2. For prophylaxis:
Organic nitrates
Beta blockers
Calcium
Drugs:
1. For treatment of acute attacks:
Organic nitrates/nitrites
2. For prophylaxis:
Organic nitrates
Beta blockers
Calcium
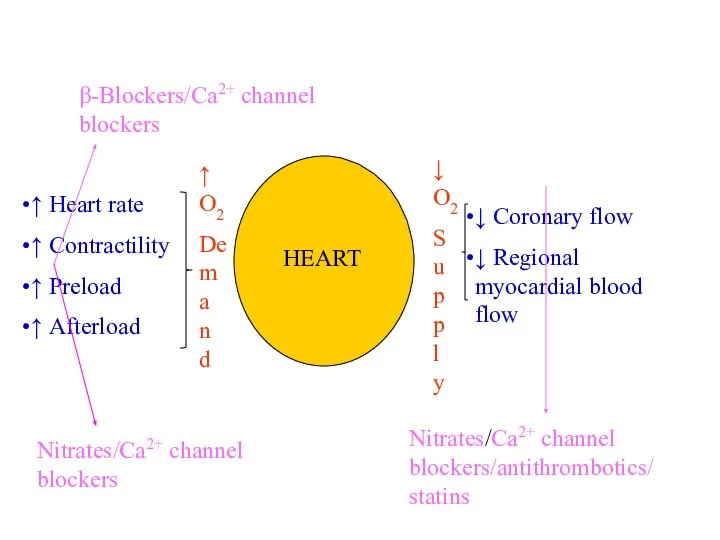
Слайд 11↑ Heart rate
↑ Contractility
↑ Preload
↑ Afterload
↓ Coronary flow
↓ Regional myocardial blood flow
↑
↑ Heart rate
↑ Contractility
↑ Preload
↑ Afterload
↓ Coronary flow
↓ Regional myocardial blood flow
↑
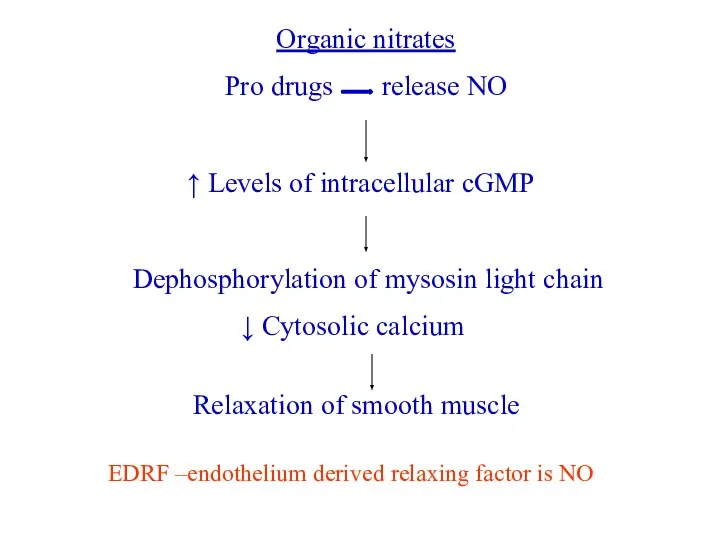
Слайд 12Organic nitrates
Pro drugs release NO
↑ Levels of intracellular cGMP
Dephosphorylation of mysosin light
Organic nitrates
Pro drugs release NO
↑ Levels of intracellular cGMP
Dephosphorylation of mysosin light
Слайд 13Relaxation of vascular smooth muscles- vasodilatation
NO-mediated guanylyl cyclase activation inhibits platelet aggregation
Relaxation
Relaxation of vascular smooth muscles- vasodilatation
NO-mediated guanylyl cyclase activation inhibits platelet aggregation
Relaxation
Слайд 14L-Arginine
NO
NO Synthases
Neurotransmission
Vasomotor
effects
Immunomodulation
Endogenous NO pathway
nNOS
eNOS
iNOS
L-Arginine
NO
NO Synthases
Neurotransmission
Vasomotor
effects
Immunomodulation
Endogenous NO pathway
nNOS
eNOS
iNOS
Слайд 15Three different forms of NO synthase are found in humans:
1. Neuronal NOS
Three different forms of NO synthase are found in humans:
1. Neuronal NOS
Слайд 16CVS Effects:
Vasodilatation- low concentrations preferably dilate veins
Venodilatation→ decreases venous return to heart
Decreased
CVS Effects:
Vasodilatation- low concentrations preferably dilate veins
Venodilatation→ decreases venous return to heart
Decreased
Слайд 17HR-unchanged or may increase slightly (reflex tachycardia)
Cardiac output slightly reduced
Even low doses
HR-unchanged or may increase slightly (reflex tachycardia)
Cardiac output slightly reduced
Even low doses
Слайд 18Coronary blood flow may initially increase transiently
Subsequently, due to decreased BP, may
Coronary blood flow may initially increase transiently
Subsequently, due to decreased BP, may
Слайд 19Reduction in myocardial O2 consumption is caused by:
Peripheral pooling of blood- reduced
Reduction in myocardial O2 consumption is caused by:
Peripheral pooling of blood- reduced
Слайд 20How myocardial O2 consumption can be determined?
Double product: HR × systolic BP-
How myocardial O2 consumption can be determined?
Double product: HR × systolic BP-
Слайд 21Pharmacokinetics:
Orally ineffective because of high first pass metabolism
Administered sublingually to avoid first
Pharmacokinetics:
Orally ineffective because of high first pass metabolism
Administered sublingually to avoid first
Слайд 22ADRs:
Headache- may be severe
May disappear after continued use or,
Decrease dose
Transient episodes of
ADRs:
Headache- may be severe
May disappear after continued use or,
Decrease dose
Transient episodes of
Слайд 23Administration of nitrates:
Sublingual
Oral: For prophylaxis, require high doses due to first pass
Administration of nitrates:
Sublingual
Oral: For prophylaxis, require high doses due to first pass
Слайд 24Transdermal nitrogycerine discs impregnated with nitroglycerine polymer- gradual absorption and 24 h
Transdermal nitrogycerine discs impregnated with nitroglycerine polymer- gradual absorption and 24 h
Слайд 25Ca2+ antagonists:
↓ Ca2+ influx
Negative iono and chronotropic effects
Peripheral vasodilatation
Used in variant angina
Ca2+ antagonists:
↓ Ca2+ influx
Negative iono and chronotropic effects
Peripheral vasodilatation
Used in variant angina
Слайд 26β-Blockers:
Effective in reducing severity and frequency of exertional angina
May worsen vasospastic angina-
β-Blockers:
Effective in reducing severity and frequency of exertional angina
May worsen vasospastic angina-
Слайд 27Ranolazine:
Reserve agent for treatment of chronic, resistant angina
Inhibits cardiac late Na+ current
Effects
Ranolazine:
Reserve agent for treatment of chronic, resistant angina
Inhibits cardiac late Na+ current
Effects
 Иммунитет. Воспаление
Иммунитет. Воспаление Атеросклероз у пожилых людей
Атеросклероз у пожилых людей Инсульт и его осложнения
Инсульт и его осложнения Новая коронавирусная инфекция у больных хирургического профиля - тактические подходы
Новая коронавирусная инфекция у больных хирургического профиля - тактические подходы Хранение лекарственных средств и изделий медицинского назначения
Хранение лекарственных средств и изделий медицинского назначения Мифы о питании
Мифы о питании Основные принципы нейрофизиологической диагностики
Основные принципы нейрофизиологической диагностики Звуковая гимнастика. Ее разновидности. Применение в ЛФК
Звуковая гимнастика. Ее разновидности. Применение в ЛФК Дәріхана қорлары және дәріхана ассортиментінің тауарларын сақтау бөлімінің жұмысын ұйымдастыру
Дәріхана қорлары және дәріхана ассортиментінің тауарларын сақтау бөлімінің жұмысын ұйымдастыру Уход и наблюдение за детьми с заболеваниями ССС
Уход и наблюдение за детьми с заболеваниями ССС Создание инновационного операционного блока модульного типа в СПб ГБУЗ Клиническая больница Святителя Луки
Создание инновационного операционного блока модульного типа в СПб ГБУЗ Клиническая больница Святителя Луки Составляющие ЗОЖ
Составляющие ЗОЖ Хроническая почечная недост
Хроническая почечная недост Разминка перед тренировкой : понятие, виды, правила выполнения
Разминка перед тренировкой : понятие, виды, правила выполнения Областное государственное казённое учреждение Романовский реабилитационный Центр инвалидов
Областное государственное казённое учреждение Романовский реабилитационный Центр инвалидов Производные пиримидина
Производные пиримидина Гипоксия плода и новорожденного ребенка
Гипоксия плода и новорожденного ребенка Опыт органосохраняющих оперций при раке молочной железы в ОБУЗ КОКОД
Опыт органосохраняющих оперций при раке молочной железы в ОБУЗ КОКОД Шинирующий бюгельный протез
Шинирующий бюгельный протез Синдромы микроструктурных аномалий хромосом
Синдромы микроструктурных аномалий хромосом Комплекс упражнений №1. Выполнение движений по тексту
Комплекс упражнений №1. Выполнение движений по тексту Усилители вкуса: влияние и последствия
Усилители вкуса: влияние и последствия Психовегетативные жалобы в практике участкового врача
Психовегетативные жалобы в практике участкового врача Роль информатики в медицине
Роль информатики в медицине Медико-психологическая помощь в условиях пандемии Covid-19
Медико-психологическая помощь в условиях пандемии Covid-19 Клинические формы воспаления
Клинические формы воспаления Висцеральное поражение при TORCH инфекции
Висцеральное поражение при TORCH инфекции Плечевое сплетение, симптомы тотального поражения
Плечевое сплетение, симптомы тотального поражения