- Endocrine pathology endocrine pancreas

Содержание
- 2. ENDOCRINE PANCREAS
- 3. ENDOCRINE PANCREAS The pancreas consists of two functionally distinct components: The exocrine pancreas, which secretes digestive
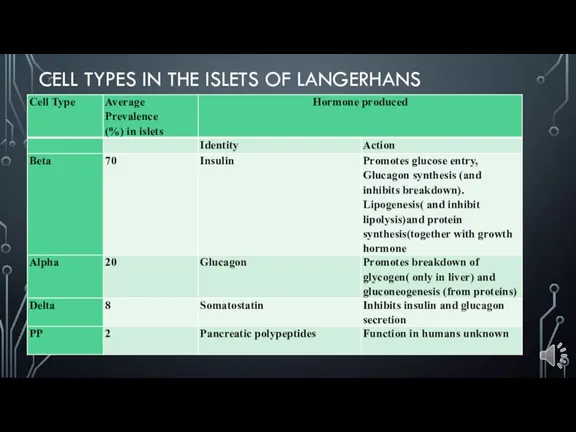
- 4. CELL TYPES IN THE ISLETS OF LANGERHANS
- 5. DIABETES MELLITUS Abnormal metabolic state characterised by glucose intolerance due to inadequate insulin action Type 1
- 6. Diagnosis is based on the clinical demonstration of glucose intolerance Insulin is unique, in that it
- 7. PATHOGENESIS The actions of insulin are all anabolic, that is, they promote the laying down of
- 8. In hyperglycaemia the renal threshold for glucose conservation is exceeded, so that there is osmotic diuresis
- 9. The combined result of severe ketosis, acidosis, hyperglycaemia, hyperosmolarity and electrolyte disturbance is to impair cerebral
- 10. CLASSIFICATION Type 1 (juvenile-onset, insulin-dependent diabetes) Typically presents in childhood. The patient usually shows the catabolic
- 11. Postmortem examination of the pancreas in patients who had recently developed type 1 diabetes but died
- 12. Autoimmune destruction. The majority of patients have circulatory antibodies to several different types of islet cell.
- 13. Type 2 (maturity-onset, non-insulin-dependent diabetes) is more common than type 1 and usually presents in middle
- 14. Type 2 (maturity-onset, non-insulin-dependent diabetes) Genetic factors clearly play an important part in the aetiology of
- 15. Secondary diabetes Hypersecretion of any of the hormones that tend to exert a hyperglycaemic effect may
- 16. COMPLICATIONS The commonest complications are seen in blood vessels. Atheroma, often ultimately severe and extensive, develops
- 17. TUMOURS Less common than pancreatic adenocarcinoma Present with endocrine effects and may be malignant Insulinoma: causes
- 18. Insulinoma Insulinoma is the commonest islet cell tumour and produces hypoglycaemia through hypersecretion of insulin. During
- 19. Gastrinomas : Although gastrin is usually produced in the G-cells of the stomach, tumours of the
- 21. Скачать презентацию
Слайд 3ENDOCRINE PANCREAS
The pancreas consists of two functionally distinct components:
The exocrine pancreas, which
ENDOCRINE PANCREAS
The pancreas consists of two functionally distinct components:
The exocrine pancreas, which
Слайд 4CELL TYPES IN THE ISLETS OF LANGERHANS
CELL TYPES IN THE ISLETS OF LANGERHANS
Слайд 5DIABETES MELLITUS
Abnormal metabolic state characterised by glucose intolerance due to inadequate insulin
DIABETES MELLITUS
Abnormal metabolic state characterised by glucose intolerance due to inadequate insulin
Слайд 6Diagnosis is based on the clinical demonstration of glucose intolerance
Insulin is
Diagnosis is based on the clinical demonstration of glucose intolerance
Insulin is
Слайд 7PATHOGENESIS
The actions of insulin are all anabolic, that is, they promote the
PATHOGENESIS
The actions of insulin are all anabolic, that is, they promote the
Слайд 8In hyperglycaemia the renal threshold for glucose conservation is exceeded, so that
In hyperglycaemia the renal threshold for glucose conservation is exceeded, so that
Слайд 9The combined result of severe ketosis, acidosis, hyperglycaemia, hyperosmolarity and electrolyte disturbance
The combined result of severe ketosis, acidosis, hyperglycaemia, hyperosmolarity and electrolyte disturbance
Слайд 10CLASSIFICATION
Type 1 (juvenile-onset, insulin-dependent diabetes)
Typically presents in childhood.
The patient usually shows
CLASSIFICATION
Type 1 (juvenile-onset, insulin-dependent diabetes)
Typically presents in childhood.
The patient usually shows
Слайд 11Postmortem examination of the pancreas in patients who had recently developed type
Postmortem examination of the pancreas in patients who had recently developed type
Слайд 12Autoimmune destruction. The majority of patients have circulatory antibodies to several different
Autoimmune destruction. The majority of patients have circulatory antibodies to several different
Слайд 13Type 2 (maturity-onset, non-insulin-dependent diabetes)
is more common than type 1 and
Type 2 (maturity-onset, non-insulin-dependent diabetes)
is more common than type 1 and
Слайд 14Type 2 (maturity-onset, non-insulin-dependent diabetes)
Genetic factors clearly play an important part in
Type 2 (maturity-onset, non-insulin-dependent diabetes)
Genetic factors clearly play an important part in
Слайд 15Secondary diabetes
Hypersecretion of any of the hormones that tend to exert a
Secondary diabetes
Hypersecretion of any of the hormones that tend to exert a
Слайд 16
COMPLICATIONS
The commonest complications are seen in blood vessels.
Atheroma, often ultimately severe
COMPLICATIONS
The commonest complications are seen in blood vessels.
Atheroma, often ultimately severe
Слайд 17TUMOURS
Less common than pancreatic adenocarcinoma
Present with endocrine effects and may be
TUMOURS
Less common than pancreatic adenocarcinoma
Present with endocrine effects and may be
Слайд 18Insulinoma
Insulinoma is the commonest islet cell tumour and produces hypoglycaemia through hypersecretion
Insulinoma
Insulinoma is the commonest islet cell tumour and produces hypoglycaemia through hypersecretion
Слайд 19Gastrinomas : Although gastrin is usually produced in the G-cells of the
Gastrinomas : Although gastrin is usually produced in the G-cells of the
Похожие презентации
 Галактоземия
Галактоземия Туберкулез кезінде қолданылатын патогенетикалық емдер
Туберкулез кезінде қолданылатын патогенетикалық емдер
 Информационные основы диагностического процесса. Установление характера заболевания
Информационные основы диагностического процесса. Установление характера заболевания Клинико - морфологические аспекты хронической почечной недостаточности. Анамнез, диагностика и этапы терапевтической коррекции
Клинико - морфологические аспекты хронической почечной недостаточности. Анамнез, диагностика и этапы терапевтической коррекции Средства, нормализующие процессы обмена веществ и уплотняющие твердые ткани зуба
Средства, нормализующие процессы обмена веществ и уплотняющие твердые ткани зуба Философия и медицина. Врачи философы
Философия и медицина. Врачи философы Синдром Леша-Нихана
Синдром Леша-Нихана О реализации в Удмуртской Республике комплекса мер, направленных на формирование здорового образа жизни среди населения
О реализации в Удмуртской Республике комплекса мер, направленных на формирование здорового образа жизни среди населения Тіс жақ сүйегінің қабыну аурулары
Тіс жақ сүйегінің қабыну аурулары Генитоуринарный менопаузальный синдром
Генитоуринарный менопаузальный синдром Биохимия неоплазии
Биохимия неоплазии Реабилитация детей с ДЦП
Реабилитация детей с ДЦП Хирургические методы лечения заболеваний пародонта: лоскутные операции и методы остеопластики дефектов альвеолярного отростка
Хирургические методы лечения заболеваний пародонта: лоскутные операции и методы остеопластики дефектов альвеолярного отростка Основные принципы профилактики внутрибольничных инфекций Агафонов Владимир Николаевич
Основные принципы профилактики внутрибольничных инфекций Агафонов Владимир Николаевич Terapia depresji
Terapia depresji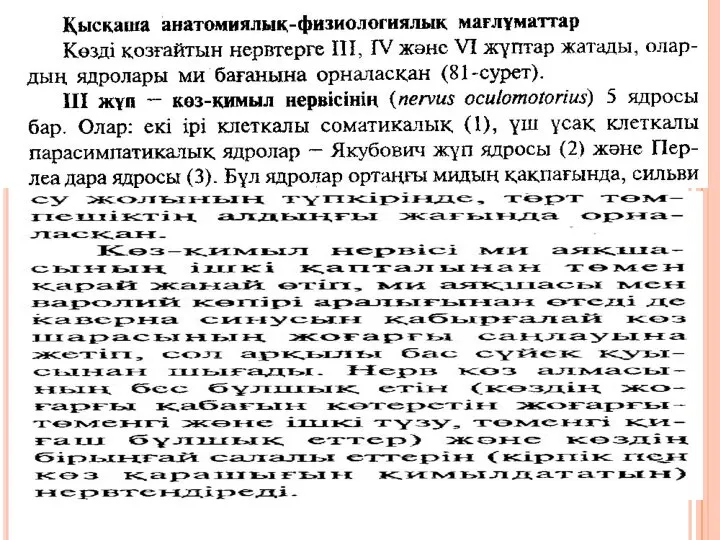 VII жұп берт нерві
VII жұп берт нерві Заболевания щитовидной железы
Заболевания щитовидной железы 14 сентября
14 сентября Травматический шок в практике фельдшера скорой медицинской помощи
Травматический шок в практике фельдшера скорой медицинской помощи Акушерское отделение патологии беременности г. Северодвинск
Акушерское отделение патологии беременности г. Северодвинск Тупі травми серця
Тупі травми серця Профилактика острых респираторных вирусных инфекций
Профилактика острых респираторных вирусных инфекций Вены. Варикозная болезнь
Вены. Варикозная болезнь Меласо. Снотворное и седативное средство
Меласо. Снотворное и седативное средство Паллиативті көмекті ұйымдастыру
Паллиативті көмекті ұйымдастыру Заболевания билиарной системы
Заболевания билиарной системы Фитотерапия хронического обструктивного бронхита
Фитотерапия хронического обструктивного бронхита