- General principles of anaesthesiology

Содержание
- 2. Introduction Preoperative History and Physical IV’s and Premedication Commonly Used Medications Room Setup and Monitors Induction
- 3. Definitions Anesthesia - From the Greek meaning lack of sensation; particularly during surgical intervention.
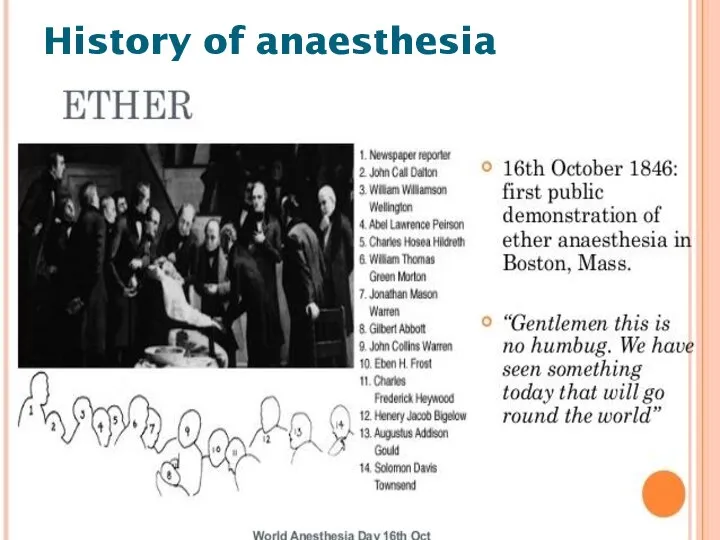
- 4. On October 16, 1846, in Boston, William T.G. Morton - the first publicized demonstration of general
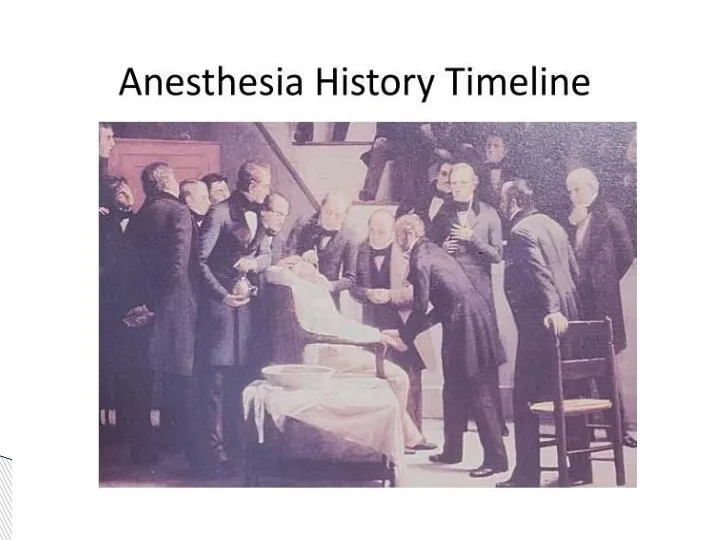
- 5. History of anaesthesia
- 6. History of anaesthesia
- 7. General anesthesia– a condition characterized by temporary shutting down consciousness pain sensitivity reflexes relaxation of skeletal
- 10. Reversible, drug-induced condition Amnesia & unconsciousness Analgesia Muscle relaxation Attenuation of autonomic responses to noxious stimulation
- 11. Anaesthesiology is the science of managing the life functions of the patients organism in time of
- 12. General Anesthesia Preoperative evaluation Intraoperative management Postoperative management
- 13. Physical Examination Physical exams of all systems. Airway assessment to determine the likelihood of difficult intubation
- 14. Unlike the standard internal medicine H&P, ours is much more focused, with specific attention being paid
- 15. • Elective: operation at a time to suit both patient and surgeon; for example hip replacement,
- 16. • Urgent: operation as soon as possible after resuscitation and within 24 h; for example intestinal
- 17. Of particular interest in the history portion of the evaluation are: Coronary Artery Disease Hypertension Asthma
- 18. Coronary Artery Disease What is the patient’s exercise tolerance? How well will his or her heart
- 19. Coronary Artery Disease What is the patient’s exercise tolerance? How well will his or her heart
- 20. Hypertension How well controlled is it? Intraoperative blood pressure management is affected by preoperative blood pressure
- 21. Asthma How well controlled is it? What triggers it? Many of the stressors of surgery as
- 22. Kidney or Liver disease Different anesthetic drugs have different modes of clearance and organ function can
- 23. Reflux Disease Present or not? Anesthetized and relaxed patients are prone to regurgitation and aspiration, particularly
- 24. Smoking Currently smoking? Airway and secretion management can become more difficult in smokers. Preoperative History and
- 25. Alcohol Consumption or Drug Abuse? Drinkers have an increased tolerance to many sedative drugs (conversely they
- 26. Diabetes Well controlled? The stress response to surgery and anesthesia can markedly increase blood glucose concentrations,
- 27. Medications Many medications interact with anesthetic agents, and some should be taken on the morning of
- 28. Allergies We routinely give narcotics and antibiotics perioperatively, and it is important to know the types
- 29. Family History There is a rare, but serious disorder known as malignant hyperthermia that affects susceptible
- 30. Anesthesia history Has the patient ever had anesthesia and surgery before? Did anything go wrong? Preoperative
- 31. Last Meal Whether the patient has an empty stomach or not impacts the choice of induction
- 32. All patients must have an assessment made of their airway, the aim being to try and
- 33. Finding any of these suggests that intubation may be more difficult. • limitation of mouth opening;
- 34. Also, any loose or missing teeth should be noted, as should cervical range of motion, mouth
- 35. Mallampati Classification Class I: Entire uvula and tonsillar pillars visible Class II: Tip of uvula and
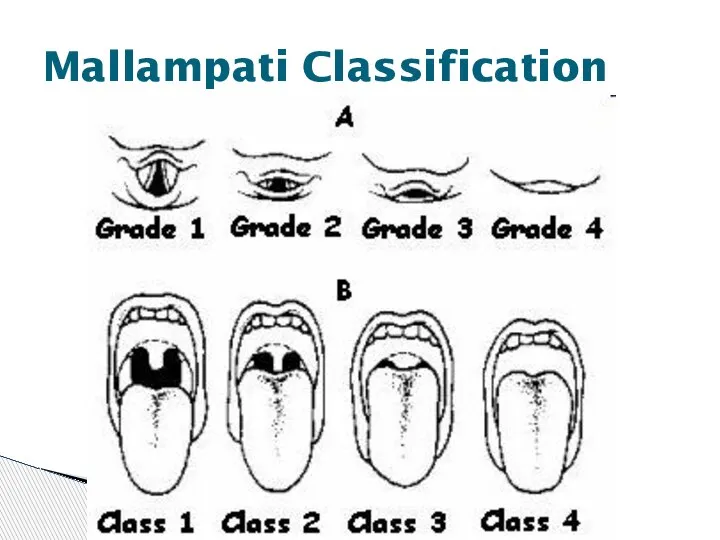
- 36. Mallampati Classification
- 37. Finally, a physical status classification is assigned, based on the criteria of the American Society of
- 38. ASA Physical Status Classification ASA-I: Healthy patient with no systemic disease ASA-II: Mild systemic disease ,
- 39. general anesthesia Simple (one-component) anaesthesia Inhalation mask endotracheal Noninhalation intravenous Combined (multi-component anaesthesia Inhalation + Inhalation
- 40. local anesthesia Terminal anesthesia Infiltration anesthesia Nerve block anesthesia trunk plexus regional anesthesia Spinal anesthesia Epidural
- 42. Every patient (with the exception of some children that can have their IV’s inserted following inhalation
- 43. Premedication refers to the administration of any drugs in the period before induction of anaesthesia. a
- 44. Many patients are understandably nervous preoperatively, and we often premedicate them, usually with a rapid acting
- 45. Before bringing the patient to the room, the anesthesia machine, ventilator, monitors, and cart must be
- 47. The monitors that we use on most patients include the pulse oximeter, blood pressure monitor, and
- 48. The anesthesia cart is set up to allow easy access to intubation equipment including endotracheal tubes,
- 49. Other preparations that can be done before the case focus on patient positioning and comfort, since
- 50. Four Phases Induction Maintenance Emergence Recovery General Anesthesia
- 51. Four Phases Induction Maintenance Emergence Recovery
- 52. You now have your sedated patient in the room with his IV and he’s comfortably lying
- 53. Stage I – Amnesia Stage II – Excitement Stage III – Surgical Intervention (4 planes) Stage
- 54. Stage I (stage of analgesia or disorientation): from beginning of induction of general anesthesia to loss
- 55. Stage III (stage of surgical anesthesia): from onset of automatic respiration to respiratory paralysis. It is
- 56. Plane II - from cessation of eyeball movements to beginning of paralysis of intercostal muscles. Laryngeal
- 57. Plane III - from beginning to completion of intercostal muscle paralysis. Diaphragmatic respiration persists but there
- 58. Plane IV - from complete intercostal paral ysis to diaphragmatic paralysis (apnea). Stage IV: from stoppage
- 59. The first part of induction of anesthesia should be preoxygenation with 100% oxygen delivered via a
- 60. Patients frequently become apneic after induction and you may have to assist ventilation. The most common
- 62. • Propofol Typical adult induction dose 1.5–2.5 mg/kg Popular and widely used drug associated with rapid
- 64. • Thiopental Sodium Typical adult induction dose 3–5 mg/kg (2.5% solution) The ‘gold-standard’ against which all
- 66. Ketamine Typical adult induction dose 0.5–2 mg/kg Useful for sedation with profound analgesia. Increases pulse rate
- 68. Ketamine
- 72. Assuming that you are now able to mask ventilate the patient, the next step is usually
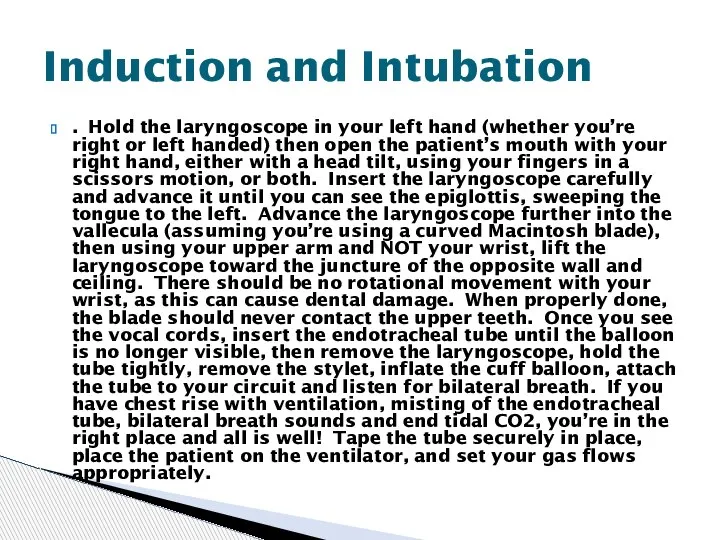
- 73. . Hold the laryngoscope in your left hand (whether you’re right or left handed) then open
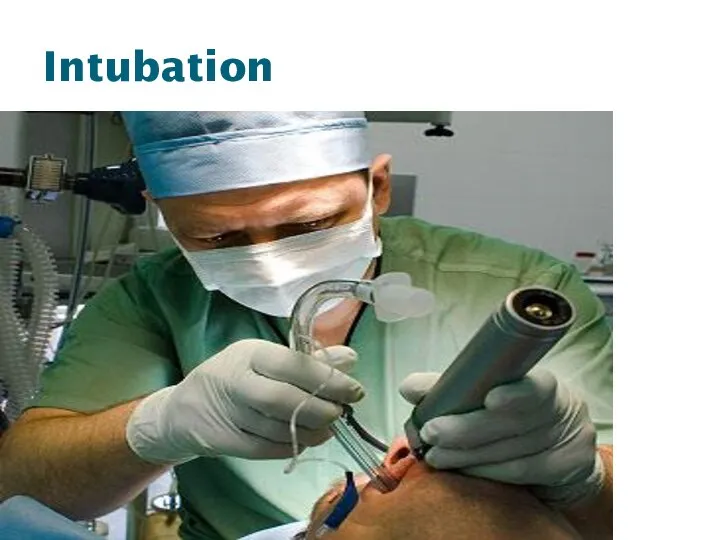
- 74. Intubation
- 75. Careful and continues vigilance of vital sings and depth of anesthesia is the integral part of
- 76. It is important to keep track of the blood loss during the case and should be
- 77. It is also vital to pay attention to the case itself, since blood loss can occur
- 78. One can also prepare for potential post-operative problems during the case, by treating the patient intraoperatively
- 81. Volatile Anesthetics Halothane Pro: Cheap, Nonirritating so can be used for inhalation induction Con: Long time
- 83. Volatile Anesthetics Sevoflurane Pro: Nonirritating so can be used for inhalation induction, Extremely rapid onset/offset Con:
- 85. Volatile Anesthetics Isoflurane Pro: Cheap, Excellent renal, hepatic, coronary, and cerebral blood flow preservation Con: Long
- 86. Volatile Anesthetics Desflurane Pro: Extremely rapid onset/offset Con: Expensive, Stimulates catecholamine release, Possibly increases postoperative nausea
- 88. Nitrous Oxide Pro: Decreases volatile anesthetic requirement, Dirt cheap, Less myocardial depression than volatile agents Con:
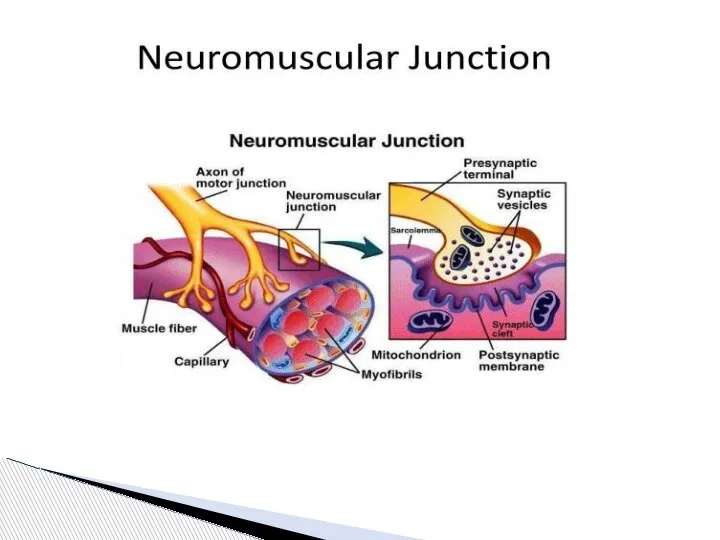
- 91. Muscle Relaxants Depolarizing Succinylcholine inhibits the postjunctional receptor and passively diffuses off the membrane, while circulating
- 92. Nondepolarizing Many different kinds, all ending in “onium” or “urium”. Each has different site of metabolism,
- 93. EMERGENCE FROM GENERAL ANESTHESIA 1. Reversal of muscle relaxation. 2. Turning off the inhalation agents and
- 94. First, the patient’s neuromuscular blockade must be re-assessed, and if necessary reversed and then rechecked with
- 95. . Once the patient is reversed, awake, suctioned, and extubated, care must be taken in transferring
- 96. The anesthesiologist’s job isn’t over once the patient leaves the operating room. Concerns that are directly
- 97. Other concerns include continuing awareness of the patient’s airway and level of consciousness, as well as
- 98. Opioids Morphine – long acting, histamine release, renally excreted active metabolite with opiate properties therefore beware
- 100. Скачать презентацию
Слайд 2Introduction
Preoperative History and Physical
IV’s and Premedication
Commonly Used Medications
Room Setup and
Introduction
Preoperative History and Physical
IV’s and Premedication
Commonly Used Medications
Room Setup and
Слайд 3Definitions
Anesthesia - From the Greek meaning lack of sensation; particularly during surgical
Definitions
Anesthesia - From the Greek meaning lack of sensation; particularly during surgical
Слайд 4On October 16, 1846, in Boston, William T.G. Morton - the first
On October 16, 1846, in Boston, William T.G. Morton - the first
Слайд 5History of anaesthesia
History of anaesthesia
Слайд 6History of anaesthesia
History of anaesthesia
Слайд 7General anesthesia–
a condition characterized by temporary shutting down
consciousness
pain sensitivity
reflexes
relaxation of skeletal
General anesthesia–
a condition characterized by temporary shutting down
consciousness
pain sensitivity
reflexes
relaxation of skeletal
Слайд 10Reversible, drug-induced condition
Amnesia & unconsciousness
Analgesia
Muscle relaxation
Attenuation of autonomic responses
Reversible, drug-induced condition
Amnesia & unconsciousness
Analgesia
Muscle relaxation
Attenuation of autonomic responses
Слайд 11Anaesthesiology is the science of managing the life functions of the patients
Anaesthesiology is the science of managing the life functions of the patients
Слайд 12General Anesthesia
Preoperative evaluation
Intraoperative management
Postoperative management
General Anesthesia
Preoperative evaluation
Intraoperative management
Postoperative management
Слайд 13Physical Examination
Physical exams of all systems.
Airway assessment to determine the
Physical exams of all systems.
Airway assessment to determine the
Слайд 14Unlike the standard internal medicine H&P, ours is much more focused, with
Unlike the standard internal medicine H&P, ours is much more focused, with
Слайд 15• Elective: operation at a time to suit both patient and surgeon;
• Elective: operation at a time to suit both patient and surgeon;
Слайд 16• Urgent: operation as soon as possible after resuscitation and within 24
• Urgent: operation as soon as possible after resuscitation and within 24
Слайд 17Of particular interest in the history portion of the evaluation are:
Coronary Artery
Of particular interest in the history portion of the evaluation are:
Coronary Artery
Слайд 18Coronary Artery Disease
What is the patient’s exercise tolerance? How well will his
Coronary Artery Disease
What is the patient’s exercise tolerance? How well will his
Слайд 19Coronary Artery Disease
What is the patient’s exercise tolerance? How well will his
Coronary Artery Disease
What is the patient’s exercise tolerance? How well will his
Слайд 20Hypertension
How well controlled is it? Intraoperative blood pressure management is affected by
Hypertension
How well controlled is it? Intraoperative blood pressure management is affected by

Слайд 21Asthma
How well controlled is it? What triggers it? Many of the stressors
Asthma
How well controlled is it? What triggers it? Many of the stressors
Слайд 22Kidney or Liver disease
Different anesthetic drugs have different modes of clearance and
Different anesthetic drugs have different modes of clearance and
Слайд 23Reflux Disease
Present or not? Anesthetized and relaxed patients are prone to regurgitation
Reflux Disease
Present or not? Anesthetized and relaxed patients are prone to regurgitation
Слайд 24Smoking
Currently smoking? Airway and secretion management can become more difficult in smokers.
Smoking
Currently smoking? Airway and secretion management can become more difficult in smokers.
Слайд 25Alcohol Consumption or Drug Abuse?
Drinkers have an increased tolerance to many sedative
Alcohol Consumption or Drug Abuse?
Drinkers have an increased tolerance to many sedative
Слайд 26Diabetes
Well controlled? The stress response to surgery and anesthesia can markedly increase
Diabetes
Well controlled? The stress response to surgery and anesthesia can markedly increase
Слайд 27Medications
Many medications interact with anesthetic agents, and some should be taken on
Medications
Many medications interact with anesthetic agents, and some should be taken on
Слайд 28Allergies
We routinely give narcotics and antibiotics perioperatively, and it is important to
Allergies
We routinely give narcotics and antibiotics perioperatively, and it is important to
Слайд 29Family History
There is a rare, but serious disorder known as malignant hyperthermia
Family History
There is a rare, but serious disorder known as malignant hyperthermia
Слайд 30Anesthesia history
Has the patient ever had anesthesia and surgery before? Did anything
Anesthesia history
Has the patient ever had anesthesia and surgery before? Did anything
Слайд 31Last Meal
Whether the patient has an empty stomach or not impacts the
Last Meal
Whether the patient has an empty stomach or not impacts the
Слайд 32All patients must have an assessment made of their airway, the aim
All patients must have an assessment made of their airway, the aim
Слайд 33Finding any of these suggests that intubation may be more difficult.
• limitation
Finding any of these suggests that intubation may be more difficult.
• limitation
Слайд 34Also, any loose or missing teeth should be noted, as should cervical
Also, any loose or missing teeth should be noted, as should cervical
Слайд 35 Mallampati Classification
Class I: Entire uvula and tonsillar pillars visible
Class II: Tip of
Mallampati Classification
Class I: Entire uvula and tonsillar pillars visible
Class II: Tip of
Слайд 36Mallampati Classification
Mallampati Classification
Слайд 37Finally, a physical status classification is assigned, based on the criteria of
Finally, a physical status classification is assigned, based on the criteria of
Слайд 38ASA Physical Status Classification
ASA-I: Healthy patient with no systemic disease
ASA-II: Mild systemic
ASA Physical Status Classification
ASA-I: Healthy patient with no systemic disease
ASA-II: Mild systemic
Слайд 39general anesthesia
Simple (one-component) anaesthesia
Inhalation
mask
endotracheal
Noninhalation
intravenous
Combined (multi-component anaesthesia
Inhalation
general anesthesia
Simple (one-component) anaesthesia
Inhalation
mask
endotracheal
Noninhalation
intravenous
Combined (multi-component anaesthesia
Inhalation
Слайд 40local anesthesia
Terminal anesthesia
Infiltration anesthesia
Nerve block anesthesia
trunk
plexus
regional anesthesia
local anesthesia
Terminal anesthesia
Infiltration anesthesia
Nerve block anesthesia
trunk
plexus
regional anesthesia
Слайд 42Every patient (with the exception of some children that can have their
Every patient (with the exception of some children that can have their
Слайд 43 Premedication refers to the administration of any drugs in the period
Premedication refers to the administration of any drugs in the period
Слайд 44Many patients are understandably nervous preoperatively, and we often premedicate them, usually
Many patients are understandably nervous preoperatively, and we often premedicate them, usually
Слайд 45Before bringing the patient to the room, the anesthesia machine, ventilator, monitors,
Before bringing the patient to the room, the anesthesia machine, ventilator, monitors,

Слайд 47The monitors that we use on most patients include the pulse oximeter,
The monitors that we use on most patients include the pulse oximeter,
Слайд 48The anesthesia cart is set up to allow easy access to intubation
The anesthesia cart is set up to allow easy access to intubation
Слайд 49Other preparations that can be done before the case focus on patient
Other preparations that can be done before the case focus on patient
Слайд 50 Four Phases
Induction
Maintenance
Emergence
Recovery
General Anesthesia
Four Phases
Induction
Maintenance
Emergence
Recovery
General Anesthesia
Слайд 51Four Phases
Induction
Maintenance
Emergence
Recovery
Induction
Maintenance
Emergence
Recovery
Слайд 52 You now have your sedated patient in the room with his
You now have your sedated patient in the room with his
Слайд 53Stage I – Amnesia
Stage II – Excitement
Stage III – Surgical
Stage I – Amnesia
Stage II – Excitement
Stage III – Surgical
Слайд 54Stage I (stage of analgesia or disorientation): from beginning of induction of
Stage I (stage of analgesia or disorientation): from beginning of induction of
Слайд 55Stage III (stage of surgical anesthesia): from onset of automatic respiration to
Stage III (stage of surgical anesthesia): from onset of automatic respiration to
Слайд 56Plane II - from cessation of eyeball movements to beginning of paralysis
Plane II - from cessation of eyeball movements to beginning of paralysis
Слайд 57Plane III - from beginning to completion of intercostal muscle paralysis. Diaphragmatic
Plane III - from beginning to completion of intercostal muscle paralysis. Diaphragmatic
Слайд 58Plane IV - from complete intercostal paral
ysis to diaphragmatic paralysis (apnea).
Stage
Plane IV - from complete intercostal paral
ysis to diaphragmatic paralysis (apnea).
Stage
Слайд 59The first part of induction of anesthesia should be preoxygenation with 100%
The first part of induction of anesthesia should be preoxygenation with 100%
Слайд 60 Patients frequently become apneic after induction and you may have to
Patients frequently become apneic after induction and you may have to
Слайд 62• Propofol
Typical adult induction
dose 1.5–2.5 mg/kg
Popular and widely used
• Propofol
Typical adult induction
dose 1.5–2.5 mg/kg
Popular and widely used
Слайд 64• Thiopental Sodium
Typical adult induction dose 3–5 mg/kg (2.5% solution)
The
• Thiopental Sodium
Typical adult induction dose 3–5 mg/kg (2.5% solution)
The
Слайд 66Ketamine
Typical adult induction dose 0.5–2 mg/kg
Useful for sedation with profound
Ketamine
Typical adult induction dose 0.5–2 mg/kg
Useful for sedation with profound
Слайд 68Ketamine
Ketamine

Слайд 72Assuming that you are now able to mask ventilate the patient, the
Assuming that you are now able to mask ventilate the patient, the
Слайд 73. Hold the laryngoscope in your left hand (whether you’re right or
. Hold the laryngoscope in your left hand (whether you’re right or
Слайд 74Intubation
Intubation
Слайд 75Careful and continues vigilance of vital sings and depth of anesthesia is
Careful and continues vigilance of vital sings and depth of anesthesia is
Слайд 76It is important to keep track of the blood loss during the
It is important to keep track of the blood loss during the
Слайд 77It is also vital to pay attention to the case itself, since
It is also vital to pay attention to the case itself, since
Слайд 78One can also prepare for potential post-operative problems during the case, by
One can also prepare for potential post-operative problems during the case, by
Слайд 81Volatile Anesthetics
Halothane
Pro: Cheap, Nonirritating so can be used for inhalation induction
Con: Long
Volatile Anesthetics
Halothane
Pro: Cheap, Nonirritating so can be used for inhalation induction
Con: Long
Слайд 83Volatile Anesthetics
Sevoflurane
Pro: Nonirritating so can be used for inhalation induction, Extremely rapid
Volatile Anesthetics
Sevoflurane
Pro: Nonirritating so can be used for inhalation induction, Extremely rapid
Слайд 85Volatile Anesthetics
Isoflurane
Pro: Cheap, Excellent renal, hepatic, coronary, and cerebral blood flow preservation
Con:
Volatile Anesthetics
Isoflurane
Pro: Cheap, Excellent renal, hepatic, coronary, and cerebral blood flow preservation
Con:
Слайд 86Volatile Anesthetics
Desflurane
Pro: Extremely rapid onset/offset
Con: Expensive, Stimulates catecholamine release, Possibly increases postoperative
Volatile Anesthetics
Desflurane
Pro: Extremely rapid onset/offset
Con: Expensive, Stimulates catecholamine release, Possibly increases postoperative
Слайд 88Nitrous Oxide
Pro: Decreases volatile anesthetic requirement, Dirt cheap, Less myocardial depression than
Pro: Decreases volatile anesthetic requirement, Dirt cheap, Less myocardial depression than

Слайд 91Muscle Relaxants
Depolarizing
Succinylcholine inhibits the postjunctional receptor and passively diffuses off the membrane,
Muscle Relaxants
Depolarizing
Succinylcholine inhibits the postjunctional receptor and passively diffuses off the membrane,
Слайд 92Nondepolarizing
Many different kinds, all ending in “onium” or “urium”. Each has different
Nondepolarizing
Many different kinds, all ending in “onium” or “urium”. Each has different
Слайд 93EMERGENCE FROM GENERAL ANESTHESIA
1. Reversal of muscle relaxation.
2. Turning off
EMERGENCE FROM GENERAL ANESTHESIA
1. Reversal of muscle relaxation.
2. Turning off
Слайд 94First, the patient’s neuromuscular blockade must be re-assessed, and if necessary reversed
First, the patient’s neuromuscular blockade must be re-assessed, and if necessary reversed
Слайд 95. Once the patient is reversed, awake, suctioned, and extubated, care must
. Once the patient is reversed, awake, suctioned, and extubated, care must
Слайд 96The anesthesiologist’s job isn’t over once the patient leaves the operating room.
The anesthesiologist’s job isn’t over once the patient leaves the operating room.
Слайд 97Other concerns include continuing awareness of the patient’s airway and level of
Other concerns include continuing awareness of the patient’s airway and level of
Слайд 98Opioids
Morphine – long acting, histamine release, renally excreted active metabolite with opiate
Opioids
Morphine – long acting, histamine release, renally excreted active metabolite with opiate
 Влияние факторов риска на организм человека
Влияние факторов риска на организм человека Анемия и беременность
Анемия и беременность МДК 02.03 лекцция № 3 ч1 акушеркам гемостаз
МДК 02.03 лекцция № 3 ч1 акушеркам гемостаз Аллергические заболевания и их профилактика
Аллергические заболевания и их профилактика Сколиоз
Сколиоз Тип Sacromastigophora, Подтип Mastigophora (Flagellata, жгутиковые)
Тип Sacromastigophora, Подтип Mastigophora (Flagellata, жгутиковые) bd4r
bd4r Жалпы зәр анализі
Жалпы зәр анализі Что мы знаем о СПИДе
Что мы знаем о СПИДе Гистоплазмоз
Гистоплазмоз Хронический панкреатит
Хронический панкреатит Медицинская помощь при проникающем ранении глаза
Медицинская помощь при проникающем ранении глаза ВИЧ – инфекция. Определение. Этиология. Эпидемиология. Патогенез. Клиника. Лечение. Профилактика
ВИЧ – инфекция. Определение. Этиология. Эпидемиология. Патогенез. Клиника. Лечение. Профилактика Нейротоксичность химиотерапии
Нейротоксичность химиотерапии Жарақаттан кейінгі ірінді перикардит емі
Жарақаттан кейінгі ірінді перикардит емі Показатели деятельности бюро №2-филиал ФКУ ГБ МСЭ по РБ
Показатели деятельности бюро №2-филиал ФКУ ГБ МСЭ по РБ :Түбір өзек жүйесіндегі анастомоздар мен коллатералдер
:Түбір өзек жүйесіндегі анастомоздар мен коллатералдер Гиперчувствительность замедленного типа. Методы диагностики ГЗТ
Гиперчувствительность замедленного типа. Методы диагностики ГЗТ Бешенство. Возбудитель бешенства
Бешенство. Возбудитель бешенства Практическая работа Изучение осанки и наличия плоскостопия
Практическая работа Изучение осанки и наличия плоскостопия Методы определения активности антибиотиков и чувствительности к ним микроорганизмов
Методы определения активности антибиотиков и чувствительности к ним микроорганизмов Фармакотерапия в сестринской практике
Фармакотерапия в сестринской практике Дистанционная литотрипсия
Дистанционная литотрипсия Технология использования липосом для непосредственной доставки в головной мозг. Области применения данных технологий
Технология использования липосом для непосредственной доставки в головной мозг. Области применения данных технологий Стресс и здоровье
Стресс и здоровье Психопатологическая семиотика. Психопатологическая синдромология
Психопатологическая семиотика. Психопатологическая синдромология Лейкозы (лейкемии)
Лейкозы (лейкемии) Ультрадыбыстық суреттерді интерпретациялау
Ультрадыбыстық суреттерді интерпретациялау