- Medical Error

Содержание
- 2. Medical Error is preventable adverse effect of medical care, whether or not it is evident or
- 3. Medical Errors Medical Errors represents a serious public health problem and pose a threat to patient
- 4. 2 Types of Human Errors Active Error- occur at the point of contact between a human
- 5. 2 Types of Human Errors Latent Errors- refer to less apparent failures of organization or design
- 6. How common are Medical Errors?
- 7. Medical Errors… A recent John Hopkins study claims more than 250,000 people in the U.S. die
- 9. Some facts… 440, 000 patient die every year from preventable medical errors. (Journal of Patient safety)
- 10. Types of Medical Error (Leape, Lucian; Lawthers, Ann G.; Brennan, Troyen A., et al. Preventing Medical
- 11. Most Common Medical Errors Misdiagnosis Delayed Diagnosis Medication Error (most common) Faulty Medical Devices Infection (CLABSI,
- 13. 8 Common Root Causes of Medical Errors Communication Problems (Verbal/Written) Inadequate Information Flow Human Problems Patient
- 14. Prevention of Medical Errors Error prevention measures include: Reduce reliance on memory Improved Information access Error-proofing
- 15. MEDICAL ERROR REPORTING
- 16. All providers (nurses, pharmacists, and physicians) must accept the inherent issues in their roles as healthcare
- 17. Medical errors and near misses should be reported when they are discovered. Healthcare professionals are usually
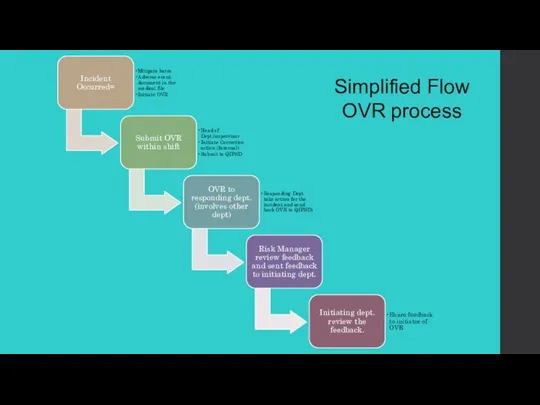
- 18. Simplified Flow OVR process
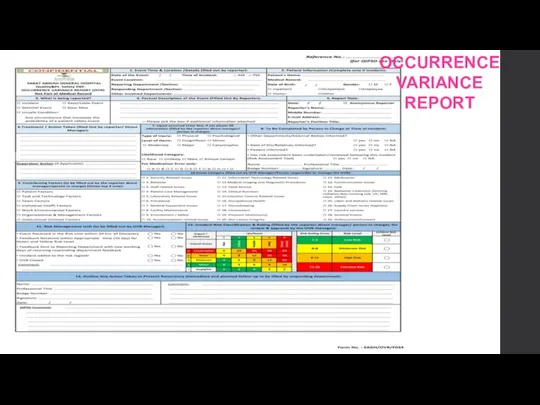
- 19. OCCURRENCE VARIANCE REPORT
- 20. We learn most from our painful mistakes. Mistakes can injure patients and land physicians in legal
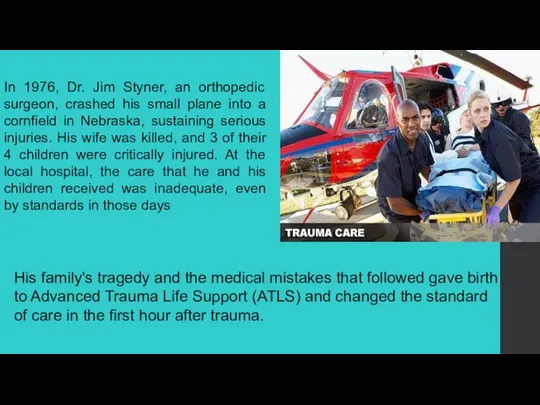
- 21. In 1976, Dr. Jim Styner, an orthopedic surgeon, crashed his small plane into a cornfield in
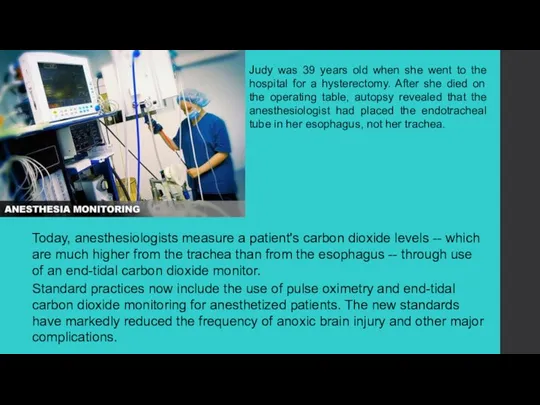
- 22. Judy was 39 years old when she went to the hospital for a hysterectomy. After she
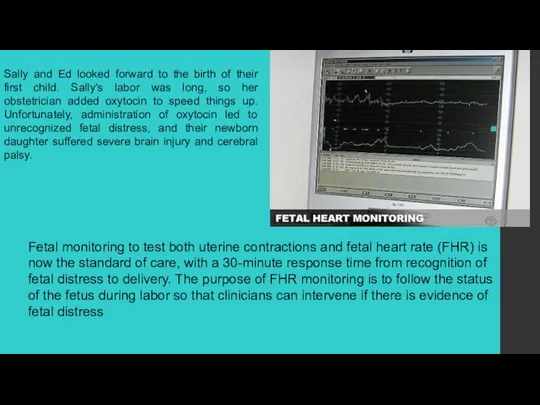
- 23. Sally and Ed looked forward to the birth of their first child. Sally's labor was long,
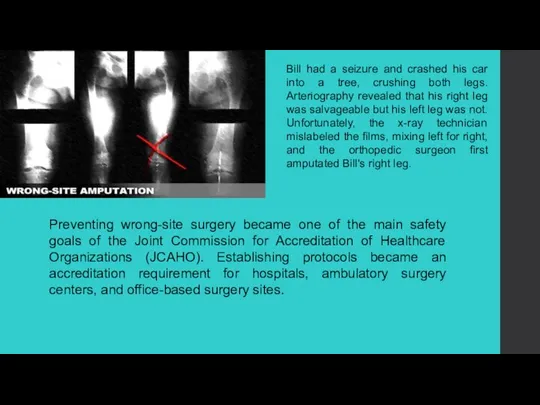
- 24. Preventing wrong-site surgery became one of the main safety goals of the Joint Commission for Accreditation
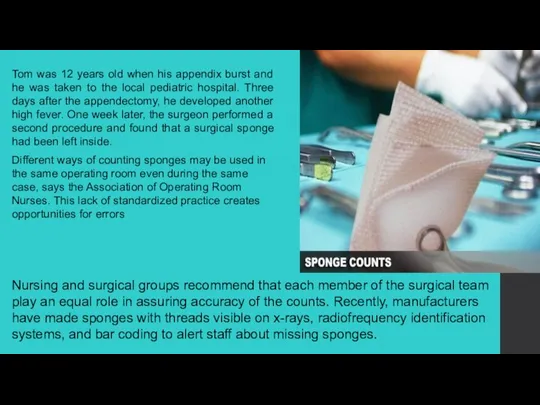
- 25. Tom was 12 years old when his appendix burst and he was taken to the local
- 26. As a young child, Betty had been given penicillin, turned blue, and was rushed to the
- 27. Linda wasn't doing well in her first trimester. The nausea and vomiting left her severely dehydrated
- 28. Frank was 72 years old when he broke his right leg in a car accident and
- 29. Lillian was 68 years old and weighed 250 lb when she underwent surgery to remove her
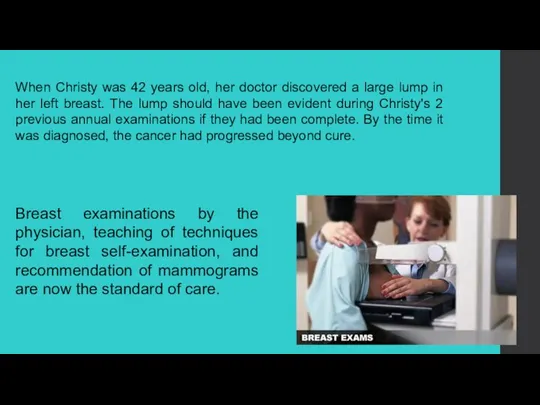
- 30. When Christy was 42 years old, her doctor discovered a large lump in her left breast.
- 32. Скачать презентацию
Слайд 3Medical Errors
Medical Errors represents a serious public health problem and pose a
Medical Errors
Medical Errors represents a serious public health problem and pose a
Слайд 42 Types of Human Errors
Active Error- occur at the point of contact
2 Types of Human Errors
Active Error- occur at the point of contact
Слайд 52 Types of Human Errors
Latent Errors- refer to less apparent failures of
2 Types of Human Errors
Latent Errors- refer to less apparent failures of
Слайд 6How common are Medical Errors?
How common are Medical Errors?
Слайд 7Medical Errors…
A recent John Hopkins study claims more than 250,000 people in
Medical Errors…
A recent John Hopkins study claims more than 250,000 people in
Слайд 9Some facts…
440, 000 patient die every year from preventable medical errors. (Journal
Some facts…
440, 000 patient die every year from preventable medical errors. (Journal
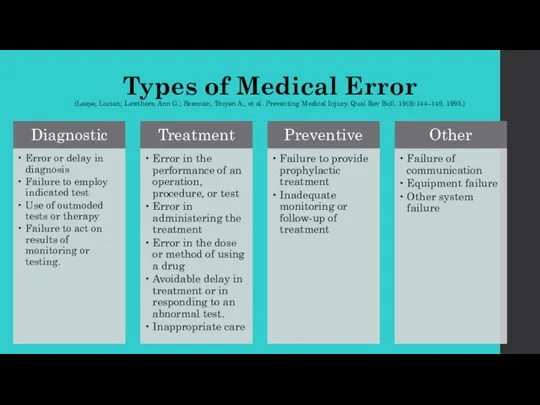
Слайд 10Types of Medical Error
(Leape, Lucian; Lawthers, Ann G.; Brennan, Troyen A., et
Types of Medical Error (Leape, Lucian; Lawthers, Ann G.; Brennan, Troyen A., et
Слайд 11Most Common Medical Errors
Misdiagnosis
Delayed Diagnosis
Medication Error (most common)
Faulty Medical Devices
Infection (CLABSI,
Most Common Medical Errors
Misdiagnosis
Delayed Diagnosis
Medication Error (most common)
Faulty Medical Devices
Infection (CLABSI,
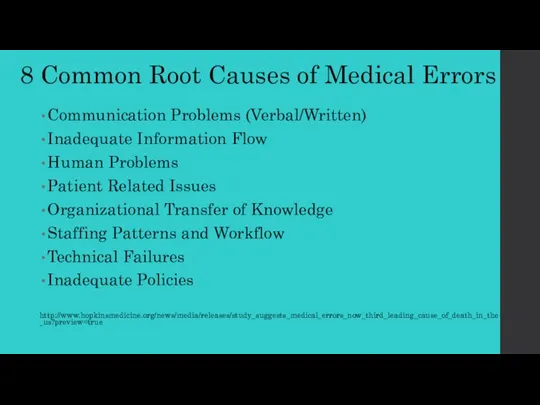
Слайд 138 Common Root Causes of Medical Errors
Communication Problems (Verbal/Written)
Inadequate Information Flow
Human
8 Common Root Causes of Medical Errors
Communication Problems (Verbal/Written)
Inadequate Information Flow
Human
Слайд 14Prevention of Medical Errors
Error prevention measures include:
Reduce reliance on memory
Improved Information access
Error-proofing
Prevention of Medical Errors
Error prevention measures include:
Reduce reliance on memory
Improved Information access
Error-proofing
Слайд 15MEDICAL ERROR REPORTING
MEDICAL ERROR REPORTING
Слайд 16All providers (nurses, pharmacists, and physicians) must accept the inherent issues in
All providers (nurses, pharmacists, and physicians) must accept the inherent issues in
Слайд 17Medical errors and near misses should be reported when they are discovered.
Medical errors and near misses should be reported when they are discovered.
Слайд 18Simplified Flow OVR process
Simplified Flow OVR process
Слайд 19OCCURRENCE VARIANCE REPORT
OCCURRENCE VARIANCE REPORT
Слайд 20We learn most from our painful mistakes. Mistakes can injure patients and
We learn most from our painful mistakes. Mistakes can injure patients and
Слайд 21In 1976, Dr. Jim Styner, an orthopedic surgeon, crashed his small plane
In 1976, Dr. Jim Styner, an orthopedic surgeon, crashed his small plane
Слайд 22Judy was 39 years old when she went to the hospital for
Judy was 39 years old when she went to the hospital for
Слайд 23Sally and Ed looked forward to the birth of their first child.
Sally and Ed looked forward to the birth of their first child.
Слайд 24Preventing wrong-site surgery became one of the main safety goals of the
Слайд 25Tom was 12 years old when his appendix burst and he was
Tom was 12 years old when his appendix burst and he was
Слайд 26As a young child, Betty had been given penicillin, turned blue, and
As a young child, Betty had been given penicillin, turned blue, and
Слайд 27Linda wasn't doing well in her first trimester. The nausea and vomiting
Linda wasn't doing well in her first trimester. The nausea and vomiting
Слайд 28Frank was 72 years old when he broke his right leg in
Frank was 72 years old when he broke his right leg in
Слайд 29Lillian was 68 years old and weighed 250 lb when she underwent
Lillian was 68 years old and weighed 250 lb when she underwent
Слайд 30When Christy was 42 years old, her doctor discovered a large lump
When Christy was 42 years old, her doctor discovered a large lump
 Клинические рекомендации: желудочковые нарушения ритма, желудочковые тахикардии и внезапная смерть
Клинические рекомендации: желудочковые нарушения ритма, желудочковые тахикардии и внезапная смерть Антиаритмические средства, влияющие на вегетативную регуляцию сердца
Антиаритмические средства, влияющие на вегетативную регуляцию сердца Сигналінг
Сигналінг Избегание супрессоров роста
Избегание супрессоров роста Нарушения кровообращения
Нарушения кровообращения Доработки функциональности ЕИС в части закупок лекарственных препаратов
Доработки функциональности ЕИС в части закупок лекарственных препаратов Основные клинические синдромы при заболеваниях мочевыделительной системы
Основные клинические синдромы при заболеваниях мочевыделительной системы Ретиноиды и их применение
Ретиноиды и их применение Виды нарушений. Коррекционная педагогика
Виды нарушений. Коррекционная педагогика Организация обеспечения инфекционной безопасности в рамках компетенции медицинской сестры по инфекционному контролю в ОРИТ
Организация обеспечения инфекционной безопасности в рамках компетенции медицинской сестры по инфекционному контролю в ОРИТ Применение фитбола в программе реабилитации при межпозвоночных грыжах
Применение фитбола в программе реабилитации при межпозвоночных грыжах Иннервация спинного нерва
Иннервация спинного нерва Роль информатики в медицине
Роль информатики в медицине Донорство крови
Донорство крови Циклические изменения, которые затрагивают весь организм женщины
Циклические изменения, которые затрагивают весь организм женщины Введение в клиническую лабораторную диагностику. Особенности забора, транспортировки, хранения, исследования
Введение в клиническую лабораторную диагностику. Особенности забора, транспортировки, хранения, исследования Лечение костномозговой формы лучевой болезни
Лечение костномозговой формы лучевой болезни Иннервация нижней конечности
Иннервация нижней конечности Урок гігієнічного навчання для дітей молодшого шкільного віку
Урок гігієнічного навчання для дітей молодшого шкільного віку терапия
терапия Инфекционные заболевания. Характеристика механизмов передачи возбудителей
Инфекционные заболевания. Характеристика механизмов передачи возбудителей Блокаторы кальциевых каналов
Блокаторы кальциевых каналов Эхинококкозы: эпидемиология, клиника, диагностика, лечение, диспансеризация и профилактика
Эхинококкозы: эпидемиология, клиника, диагностика, лечение, диспансеризация и профилактика Ультразвуковое исследование портальной гипертензии
Ультразвуковое исследование портальной гипертензии Свет. Фототерапия. Гелиотерапия. Механизмы воздействия солнечного света на организм
Свет. Фототерапия. Гелиотерапия. Механизмы воздействия солнечного света на организм Общая пропедевтика системы пищеварения
Общая пропедевтика системы пищеварения Профессиональная нейросенсорная тугоухость
Профессиональная нейросенсорная тугоухость Дәлелді медицинаның құралдары және әдістері
Дәлелді медицинаның құралдары және әдістері