- Peptic Ulcer

Содержание
- 2. Peptic Ulcer 10% population affected Gastric ulcer in elderly 5-6th decade Duodenal ulcer in adults 4th
- 3. Duodenal Ulcer Proximal duodenum 1 - 2 cm of pylorus ▲ acid Distal duodenum = ZE
- 4. Type 1 Gastric Ulcer most common (among gastric Ulcers) proximal antrum ↓ mucosal defense ↓ acid
- 5. Type II Gastric Ulcer Secondary to DU + pyloric stenosis
- 6. Type III Gastric Ulcer Prepyloric and pyloric canal ulcer acid ▲ common etiology with DU
- 7. Incidence etiology CP Investigations DD Rx
- 8. Pathogenesis Imbalance of acid-pepsin and mucosal defence H. pylori infection NSAID ZE Syndrome Type A personality
- 9. H.pylori 95% - duodenal ulcer 80% - gastric ulcer ↓ mucosal resistance hydrophobicity eradication reduces ulcer
- 10. NSAID Suppress prostaglandins prostaglandin ► ↓ acid secretion ↑ ▲ mucosal blood flow ↑ mucus &
- 11. A/ DU NSAIDs Acid hypersecretion Rapid gastric emptying Impaired acid disposal Smoking
- 12. Duodenal Ulcer Increased secretion of acid More rapid gastric emptying Decreased prostaglandin Chronic duodenitis with H.pylori
- 13. Gastric Ulcer H.pylori NSAIDs Duodenogastric reflux Impaired gastric mucosal defense
- 14. Gastric Ulcer Acid secretion - normal to low Reflux of duodenal contents → gastritis → ulcer
- 15. Clinical Presentation Duodenal Ulcer pain relieved by food or alkali pain several hours after meal Gastric
- 16. Periodic chronic recurrent pain Nausea & vomiting Weight loss Epigastric tenderness
- 17. Investigations Endoscopy 90% sensitivity must in all pts. with severe pain excludes malignancy biopsy can be
- 18. Investigations Barium Meal double (air) contrast 90% sensitivity
- 19. H Pylori detection: Breath test Blood test Tissue test
- 20. Treatment Stop smoking, NSAIDs Stop alcohol Antacids - acid neutralisation H2 receptor antagonist -Ranitidine - secretion
- 21. H+ pump inhibition - H+/K+ase inhibition - Omeprazole Anticholinergic - secretory inhibition Prostaglandin - Misoprostol -
- 22. Proton Pump Blockers Omeperazole Eso-meperazole Rabi-meperazole
- 23. Sucralfate - protective coating Colloidal Bismuth eradicate H.pylori protective coating Antibiotics - H.pylori Kit for H
- 24. H2 Receptor Antagonists On parietal cells Decrease basal & stimulated acid secretion Pepsin output decreased Decreased
- 25. Treatment - Duodenal Ulcer 95% control - medical Rx Surgery-Outdated, Obsolete Omeprazole better thanRanitidine Ulcer heels
- 26. Indications for surgery =Compl Hemorrhage Obstruction Perforation Intractability of pain Intractable pain ► HSV / TV
- 27. H2 blockers heals 75% DU in 4 weeks H/K proton pump inhibitor better results ulcer may
- 28. Indication of surgery in hemorrhage bleeding of > than 6 units recurrent bleed after endoscopic control
- 29. Perforation - simple closure with omental patch -Graham’s patch definitive surgery HSV TV + pyloroplasty parietal
- 30. Treatment GU Omeprazole, H2 receptor antagonist - 8 weeks if pain not relieved by 2 weeks
- 31. Type I - Distal Gastrectomy with vagotomy + G-D or GJ proximal ulcer- total gastrectomy parietal
- 32. Hemorrhage Hemorrhage - potential cause of death 15 -20% gross bleeding erosion of duodenal ulcer into
- 33. Perforation In 5-10% of cases pneumo-peritoneum in 75% cases peritonitis, pain, ileus leukocytosis, hypovolumia, IIIrd space
- 34. Obstruction Chronic ulcer disease with edema and scarring in 5% cases of DU nausea, vomiting, abdominal
- 35. Obstruction Endoscopy Ba study Scintigraphy Rx V + G-J / G-D
- 37. Скачать презентацию
Слайд 2Peptic Ulcer
10% population affected
Gastric ulcer in elderly 5-6th decade
Duodenal ulcer in adults
Peptic Ulcer
10% population affected
Gastric ulcer in elderly 5-6th decade
Duodenal ulcer in adults
Слайд 3Duodenal Ulcer
Proximal duodenum
1 - 2 cm of pylorus
▲ acid
Distal duodenum = ZE
Duodenal Ulcer
Proximal duodenum
1 - 2 cm of pylorus
▲ acid
Distal duodenum = ZE
Слайд 4Type 1 Gastric Ulcer
most common (among gastric Ulcers)
proximal antrum
↓ mucosal defense
↓ acid
Type 1 Gastric Ulcer
most common (among gastric Ulcers)
proximal antrum
↓ mucosal defense
↓ acid
Слайд 5Type II Gastric Ulcer
Secondary to DU + pyloric stenosis
Type II Gastric Ulcer
Secondary to DU + pyloric stenosis
Слайд 6Type III Gastric Ulcer
Prepyloric and pyloric canal ulcer
acid ▲
common etiology with DU
Type III Gastric Ulcer
Prepyloric and pyloric canal ulcer
acid ▲
common etiology with DU
Слайд 7Incidence
etiology
CP
Investigations
DD
Rx
Incidence
etiology
CP
Investigations
DD
Rx
Слайд 8Pathogenesis
Imbalance of acid-pepsin and mucosal defence
H. pylori infection
NSAID
ZE Syndrome
Type A personality
Pathogenesis
Imbalance of acid-pepsin and mucosal defence
H. pylori infection
NSAID
ZE Syndrome
Type A personality
Слайд 9H.pylori
95% - duodenal ulcer
80% - gastric ulcer
↓ mucosal resistance hydrophobicity
eradication reduces
H.pylori
95% - duodenal ulcer
80% - gastric ulcer
↓ mucosal resistance hydrophobicity
eradication reduces
Слайд 10NSAID
Suppress prostaglandins
prostaglandin ►
↓ acid secretion
↑ ▲ mucosal blood flow
↑ mucus &
NSAID
Suppress prostaglandins
prostaglandin ►
↓ acid secretion
↑ ▲ mucosal blood flow
↑ mucus &
Слайд 11A/ DU
NSAIDs
Acid hypersecretion
Rapid gastric emptying
Impaired acid disposal
Smoking
A/ DU
NSAIDs
Acid hypersecretion
Rapid gastric emptying
Impaired acid disposal
Smoking
Слайд 12Duodenal Ulcer
Increased secretion of acid
More rapid gastric emptying
Decreased prostaglandin
Chronic duodenitis with H.pylori
Smoking
Duodenal Ulcer
Increased secretion of acid
More rapid gastric emptying
Decreased prostaglandin
Chronic duodenitis with H.pylori
Smoking
Слайд 13Gastric Ulcer
H.pylori
NSAIDs
Duodenogastric reflux
Impaired gastric mucosal defense
Gastric Ulcer
H.pylori
NSAIDs
Duodenogastric reflux
Impaired gastric mucosal defense
Слайд 14Gastric Ulcer
Acid secretion - normal to low
Reflux of duodenal contents → gastritis
Gastric Ulcer
Acid secretion - normal to low
Reflux of duodenal contents → gastritis
Слайд 15Clinical Presentation
Duodenal Ulcer
pain relieved by food or alkali
pain several hours
Clinical Presentation
Duodenal Ulcer
pain relieved by food or alkali
pain several hours
Слайд 16Periodic chronic recurrent pain
Nausea & vomiting
Weight loss
Epigastric tenderness
Periodic chronic recurrent pain
Nausea & vomiting
Weight loss
Epigastric tenderness
Слайд 17Investigations
Endoscopy
90% sensitivity
must in all pts. with severe pain
Investigations
Endoscopy
90% sensitivity
must in all pts. with severe pain
Слайд 18Investigations
Barium Meal double (air) contrast
90% sensitivity
Investigations
Barium Meal double (air) contrast
90% sensitivity
Слайд 19H Pylori detection:
Breath test
Blood test
Tissue test
H Pylori detection:
Breath test
Blood test
Tissue test
Слайд 20Treatment
Stop smoking, NSAIDs
Stop alcohol
Antacids - acid neutralisation
H2 receptor antagonist -Ranitidine - secretion inhibition
Treatment
Stop smoking, NSAIDs
Stop alcohol
Antacids - acid neutralisation
H2 receptor antagonist -Ranitidine - secretion inhibition
Слайд 21H+ pump inhibition - H+/K+ase inhibition - Omeprazole
Anticholinergic - secretory inhibition
Prostaglandin -
H+ pump inhibition - H+/K+ase inhibition - Omeprazole
Anticholinergic - secretory inhibition
Prostaglandin -
Слайд 22Proton Pump Blockers
Omeperazole
Eso-meperazole
Rabi-meperazole
Proton Pump Blockers
Omeperazole
Eso-meperazole
Rabi-meperazole
Слайд 23Sucralfate - protective coating
Colloidal Bismuth
eradicate H.pylori
protective coating
Antibiotics - H.pylori
Kit
Sucralfate - protective coating
Colloidal Bismuth
eradicate H.pylori
protective coating
Antibiotics - H.pylori
Kit
Слайд 24H2 Receptor Antagonists
On parietal cells
Decrease basal & stimulated acid secretion
Pepsin output decreased
Decreased
H2 Receptor Antagonists
On parietal cells
Decrease basal & stimulated acid secretion
Pepsin output decreased
Decreased
Слайд 25Treatment - Duodenal Ulcer
95% control - medical Rx
Surgery-Outdated, Obsolete
Omeprazole better thanRanitidine
Ulcer heels
Treatment - Duodenal Ulcer
95% control - medical Rx
Surgery-Outdated, Obsolete
Omeprazole better thanRanitidine
Ulcer heels
Слайд 26Indications for surgery =Compl
Hemorrhage
Obstruction
Perforation
Intractability of pain
Intractable pain ► HSV / TV + GJ
Indications for surgery =Compl
Hemorrhage
Obstruction
Perforation
Intractability of pain
Intractable pain ► HSV / TV + GJ
Слайд 27H2 blockers heals 75% DU in 4 weeks
H/K proton pump inhibitor better
H2 blockers heals 75% DU in 4 weeks
H/K proton pump inhibitor better
Слайд 28Indication of surgery in hemorrhage
bleeding of > than 6 units
recurrent bleed after
Indication of surgery in hemorrhage
bleeding of > than 6 units
recurrent bleed after
Слайд 29Perforation - simple closure with omental patch -Graham’s patch
definitive surgery
HSV
TV + pyloroplasty
parietal
Perforation - simple closure with omental patch -Graham’s patch
definitive surgery
HSV
TV + pyloroplasty
parietal
Слайд 30Treatment GU
Omeprazole, H2 receptor antagonist - 8 weeks
if pain not relieved by
Treatment GU
Omeprazole, H2 receptor antagonist - 8 weeks
if pain not relieved by
Слайд 31Type I - Distal Gastrectomy with vagotomy + G-D or GJ
proximal ulcer-
Type I - Distal Gastrectomy with vagotomy + G-D or GJ
proximal ulcer-
Слайд 32Hemorrhage
Hemorrhage - potential cause of death
15 -20% gross bleeding
erosion of duodenal
Hemorrhage
Hemorrhage - potential cause of death
15 -20% gross bleeding
erosion of duodenal
Слайд 33Perforation
In 5-10% of cases
pneumo-peritoneum in 75% cases
peritonitis, pain, ileus
leukocytosis, hypovolumia, IIIrd space
Perforation
In 5-10% of cases
pneumo-peritoneum in 75% cases
peritonitis, pain, ileus
leukocytosis, hypovolumia, IIIrd space
Слайд 34Obstruction
Chronic ulcer disease with edema and scarring
in 5% cases of DU
nausea, vomiting,
Obstruction
Chronic ulcer disease with edema and scarring
in 5% cases of DU
nausea, vomiting,
Слайд 35Obstruction
Endoscopy
Ba study
Scintigraphy
Rx V + G-J / G-D
Obstruction
Endoscopy
Ba study
Scintigraphy
Rx V + G-J / G-D
 Особенности визуальной диагностики патологии дыхательной системы у детей на примере пневмонии
Особенности визуальной диагностики патологии дыхательной системы у детей на примере пневмонии Зачем мы спим ночью
Зачем мы спим ночью Кофеин, источники получения. Психостимулирующий и аналептический эффекты, механизмы их развития, показания к применению. Теизм
Кофеин, источники получения. Психостимулирующий и аналептический эффекты, механизмы их развития, показания к применению. Теизм Медицинские пластыри
Медицинские пластыри Биоэтика и реализация соматических прав в странах Арабского мира
Биоэтика и реализация соматических прав в странах Арабского мира Скалолазание как вид горного туризма для оздоравливания позвоночника
Скалолазание как вид горного туризма для оздоравливания позвоночника Медицинская паразитология. Гельминтология
Медицинская паразитология. Гельминтология Строение и работа мышц
Строение и работа мышц Столбняк. Определение. Этиология. Эпидемиология
Столбняк. Определение. Этиология. Эпидемиология Сон в короне
Сон в короне Реакция нейтрализации токсина антитоксической сывороткой. Реакция нейтрализации вирусов. РИФ
Реакция нейтрализации токсина антитоксической сывороткой. Реакция нейтрализации вирусов. РИФ Записывайтесь на вакцинацию COVID-19
Записывайтесь на вакцинацию COVID-19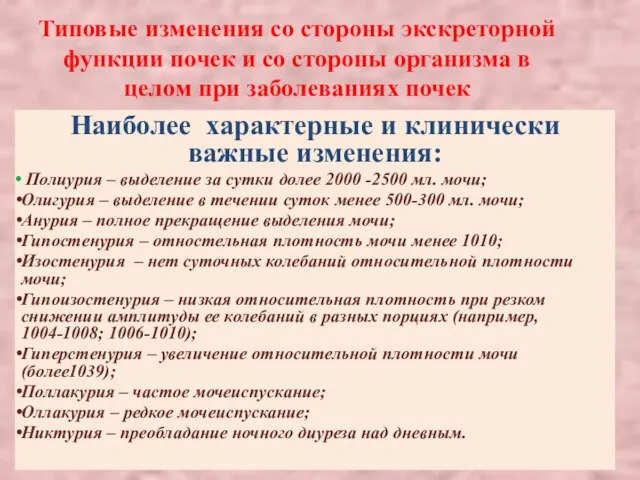 Типовые изменения со стороны экскреторной функции почек и со стороны организма в целом при заболеваниях почек
Типовые изменения со стороны экскреторной функции почек и со стороны организма в целом при заболеваниях почек Биоэтика
Биоэтика Лечение среднего кариеса. Техника наложения постоянной пломбы из композита химического и светового отверждения
Лечение среднего кариеса. Техника наложения постоянной пломбы из композита химического и светового отверждения Ботулизм
Ботулизм Кластерная головная боль
Кластерная головная боль Зиянды әдеттерді алдын алатын аппараттар
Зиянды әдеттерді алдын алатын аппараттар Проект #стопСПИД/ВИЧ
Проект #стопСПИД/ВИЧ Патогенез диабетических микроангиопатий
Патогенез диабетических микроангиопатий Абдоминальная бригада. Топографическая анатомия органов брюшной полости
Абдоминальная бригада. Топографическая анатомия органов брюшной полости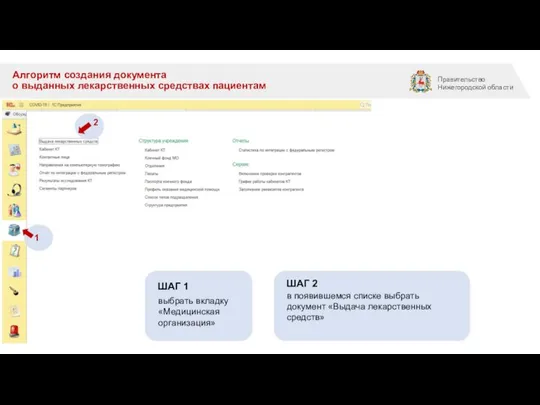 Алгоритм создания документа о выданных лекарственных средствах пациентам
Алгоритм создания документа о выданных лекарственных средствах пациентам Сахарный диабет
Сахарный диабет Медико-социальная поддержка пожилому населению в России
Медико-социальная поддержка пожилому населению в России Профессиональная деятельность акушерки при ведении беременности и родов у ВИЧ-инфицированных
Профессиональная деятельность акушерки при ведении беременности и родов у ВИЧ-инфицированных Альдостерон-рениновое соотношение (АРС)
Альдостерон-рениновое соотношение (АРС) Группы крови-1 (2)
Группы крови-1 (2) ГБУЗ КО Кемеровский клинический детский психоневрологический санаторий Искорка
ГБУЗ КО Кемеровский клинический детский психоневрологический санаторий Искорка