- Heart murmurs

Содержание
- 2. Outline I. Basic Pathophysiology II. Describing murmurs III. Systolic murmurs IV. Diastolic murmurs V. Continuous murmurs
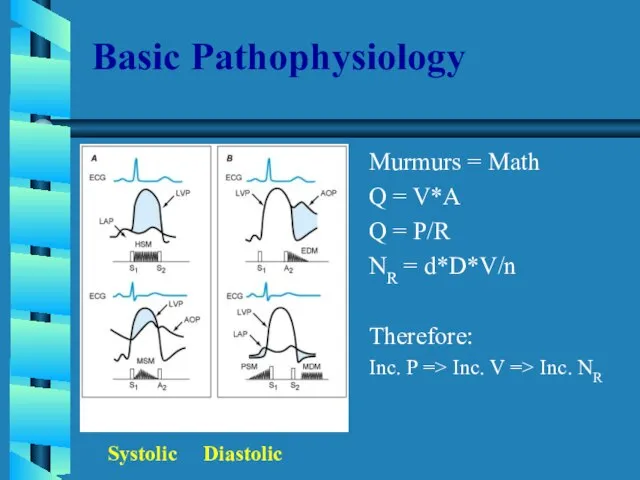
- 3. Basic Pathophysiology Murmurs = Math Q = V*A Q = P/R NR = d*D*V/n Therefore: Inc.
- 4. Describing a heart murmur 1. Timing murmurs are longer than heart sounds HS can distinguished by
- 5. Describing a heart murmur con’t: 4. Radiation reflects the intensity of the murmur and the direction
- 6. Describing a heart murmur con’t: 6. Pitch high, medium, low 7. Quality blowing, harsh, rumbling, and
- 7. Systolic Murmurs Derived from increased turbulence associated with: 1. Increased flow across normal SL valve or
- 8. Early Systolic murmurs 1. Acute severe mitral regurgitation decrescendo murmur best heard at apical impulse Caused
- 9. Midsystolic (ejection) murmurs Are the most common kind of heart murmur Are usually crescendo-decrescendo They may
- 10. Aortic stenosis Loudest in aortic area; radiates along the carotid arteries Intensity varies directly with CO
- 11. Hypertrophic cardiomyopathy Loudest b/t left sternal edge and apex; Grade 2-3/6 Does NOT radiate into neck;
- 12. Pansystolic (Holosystolic) Murmurs Are pathologic Murmur begins immediately with S1 and continues up to S2 1.
- 13. Diastolic Murmurs Almost always indicate heart disease Two basic types: 1. Early decrescendo diastolic murmurs signify
- 14. Aortic Regurgitation Best heard in the 2nd ICS at the left sternal edge High pitched, decrescendo
- 15. Mitral Stenosis Two components: 1. Middiastolic - during rapid ventricular filling 2. Presystolic - during atrial
- 16. Continuous Murmurs Begin in systole, peak near s2, and continue into all or part of diastole.
- 17. Back to the Basics 1. When does it occur - systole or diastole 2. Where is
- 19. Скачать презентацию
Слайд 2Outline
I. Basic Pathophysiology
II. Describing murmurs
III. Systolic murmurs
IV. Diastolic murmurs
V. Continuous murmurs
VI. Summary
Outline
I. Basic Pathophysiology
II. Describing murmurs
III. Systolic murmurs
IV. Diastolic murmurs
V. Continuous murmurs
VI. Summary
Слайд 3Basic Pathophysiology
Murmurs = Math
Q = V*A
Q = P/R
NR = d*D*V/n
Therefore:
Inc. P =>
Basic Pathophysiology
Murmurs = Math
Q = V*A
Q = P/R
NR = d*D*V/n
Therefore:
Inc. P =>
Слайд 4Describing a heart murmur
1. Timing
murmurs are longer than heart sounds
HS can distinguished
Describing a heart murmur
1. Timing
murmurs are longer than heart sounds
HS can distinguished
Слайд 5Describing a heart murmur con’t:
4. Radiation
reflects the intensity of the murmur and
Describing a heart murmur con’t:
4. Radiation
reflects the intensity of the murmur and
Слайд 6Describing a heart murmur con’t:
6. Pitch
high, medium, low
7. Quality
blowing, harsh, rumbling, and
Describing a heart murmur con’t:
6. Pitch
high, medium, low
7. Quality
blowing, harsh, rumbling, and
Слайд 7Systolic Murmurs
Derived from increased turbulence associated with:
1. Increased flow across normal SL
Systolic Murmurs
Derived from increased turbulence associated with:
1. Increased flow across normal SL
Слайд 8Early Systolic murmurs
1. Acute severe mitral regurgitation
decrescendo murmur
best heard at apical impulse
Early Systolic murmurs
1. Acute severe mitral regurgitation
decrescendo murmur
best heard at apical impulse
Слайд 9Midsystolic (ejection) murmurs
Are the most common kind of heart murmur
Are usually crescendo-decrescendo
They
Midsystolic (ejection) murmurs
Are the most common kind of heart murmur
Are usually crescendo-decrescendo
They
Слайд 10Aortic stenosis
Loudest in aortic area; radiates along the carotid arteries
Intensity varies directly
Aortic stenosis
Loudest in aortic area; radiates along the carotid arteries
Intensity varies directly
Слайд 11Hypertrophic cardiomyopathy
Loudest b/t left sternal edge and apex; Grade 2-3/6
Does NOT radiate
Hypertrophic cardiomyopathy
Loudest b/t left sternal edge and apex; Grade 2-3/6
Does NOT radiate
Слайд 12Pansystolic (Holosystolic) Murmurs
Are pathologic
Murmur begins immediately with S1 and continues up to
Pansystolic (Holosystolic) Murmurs
Are pathologic
Murmur begins immediately with S1 and continues up to
Слайд 13Diastolic Murmurs
Almost always indicate heart disease
Two basic types:
1. Early decrescendo diastolic murmurs
signify
Diastolic Murmurs
Almost always indicate heart disease
Two basic types:
1. Early decrescendo diastolic murmurs
signify
Слайд 14Aortic Regurgitation
Best heard in the 2nd ICS at the left sternal edge
High
Aortic Regurgitation
Best heard in the 2nd ICS at the left sternal edge
High
Слайд 15Mitral Stenosis
Two components:
1. Middiastolic - during rapid ventricular filling
2. Presystolic - during
Mitral Stenosis
Two components:
1. Middiastolic - during rapid ventricular filling
2. Presystolic - during
Слайд 16Continuous Murmurs
Begin in systole, peak near s2, and continue into all or
Continuous Murmurs
Begin in systole, peak near s2, and continue into all or
Слайд 17Back to the Basics
1. When does it occur - systole or diastole
2.
Back to the Basics
1. When does it occur - systole or diastole
2.
 РАЗВИТИЕ КАРТОГРАФИИ В РОССИИ(XVI – ПЕРВАЯ ПОЛОВИНА XIX ВЕКА)
РАЗВИТИЕ КАРТОГРАФИИ В РОССИИ(XVI – ПЕРВАЯ ПОЛОВИНА XIX ВЕКА) Методика обучения спуска на лыжах.
Методика обучения спуска на лыжах. Hallo!Wie hei?t du?Meine Familie.Meine Freunde.
Hallo!Wie hei?t du?Meine Familie.Meine Freunde. Ты, человек, любя природу,Хоть иногда её жалей:В увеселительных походахНе растопчи её полей.В вокзальной сутолоке векаТы оценит
Ты, человек, любя природу,Хоть иногда её жалей:В увеселительных походахНе растопчи её полей.В вокзальной сутолоке векаТы оценит Проект Район и деревня, где я живу Октябрьский район с.Черницыно
Проект Район и деревня, где я живу Октябрьский район с.Черницыно Брак в Древней Иудее
Брак в Древней Иудее Тема: Отмена крепостного права в России
Тема: Отмена крепостного права в России Водно-электролитные нарушения у хирургических больных, инвазивная терапия
Водно-электролитные нарушения у хирургических больных, инвазивная терапия Петербург Ф.М.Достоевского «Преступление и наказание»
Петербург Ф.М.Достоевского «Преступление и наказание» Презентация на тему Все профессии важны
Презентация на тему Все профессии важны  Проверка домашнего задания
Проверка домашнего задания Атмосфера и ее свойства
Атмосфера и ее свойства Теорема Фалеса
Теорема Фалеса «Я иду на урок биологии»
«Я иду на урок биологии» Восстание декабристов
Восстание декабристов Распространение колебаний в упругих средах. Волны
Распространение колебаний в упругих средах. Волны Иван Алексеевич Бунин1870-1953
Иван Алексеевич Бунин1870-1953 Фонд новых форм развития образования о вызовах современности
Фонд новых форм развития образования о вызовах современности Модуль управления тепловизионным комплексом
Модуль управления тепловизионным комплексом Состязание юных Математиков
Состязание юных Математиков Константин Сергеевич Станиславский
Константин Сергеевич Станиславский _AFTsNS_Lektsiya_1 (2)
_AFTsNS_Lektsiya_1 (2) Судебная система РФ
Судебная система РФ Иван Грозный
Иван Грозный система оценки качества образования в школе
система оценки качества образования в школе Заполнение Психоматрицы. Занятие 2
Заполнение Психоматрицы. Занятие 2 Предложение по размещению на фасаде
Предложение по размещению на фасаде Декабристы в Ялуторовске
Декабристы в Ялуторовске