- Immunology of transplantation. Reproductive immunology

Содержание
- 2. Transplantation immunology is getting increasingly important, from a clinical point of view, now involving cellular grafts
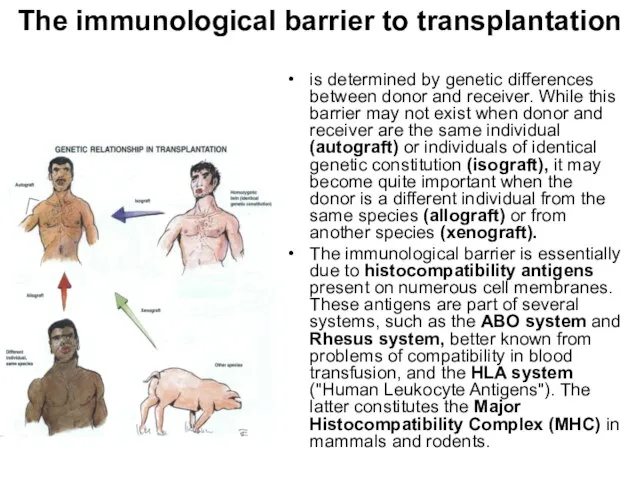
- 3. The immunological barrier to transplantation is determined by genetic differences between donor and receiver. While this
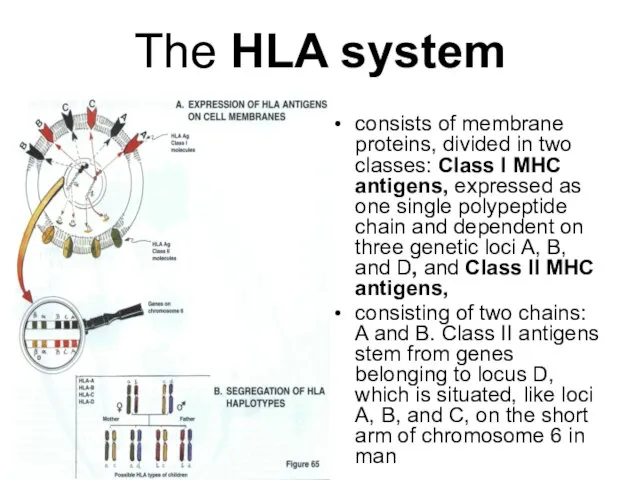
- 4. The HLA system consists of membrane proteins, divided in two classes: Class I MHC antigens, expressed
- 5. The HLA system (cont-d) Class I antigens are present on most nucleated cells, the distribution of
- 6. Clinical considerations even sister may be with an identical HLA formula. As a result, we are
- 7. transplantation between a donor and receiver which are not identical for their histocompatibility antigens, leads obligatorily
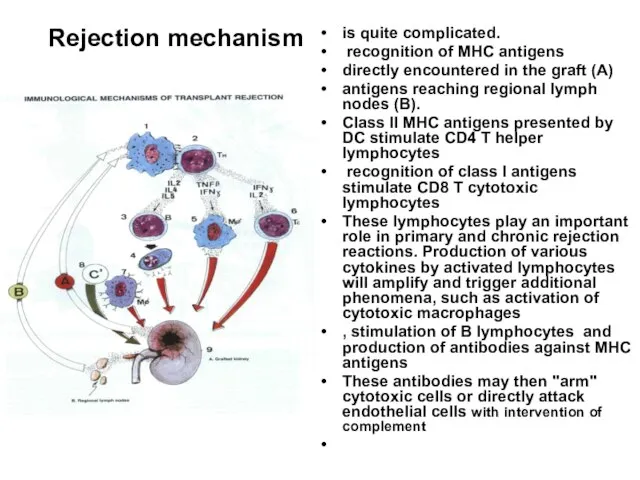
- 8. Rejection mechanism is quite complicated. recognition of MHC antigens directly encountered in the graft (A) antigens
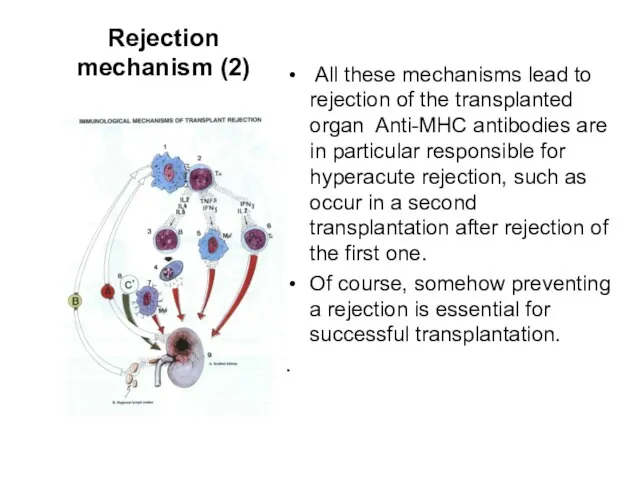
- 9. Rejection mechanism (2) All these mechanisms lead to rejection of the transplanted organ Anti-MHC antibodies are
- 10. Possible ways of prophylaxis A first step reducing as much as possible the MHC differences between
- 11. Graft-Versus-Host Reaction (GVH) In this type of reaction, it could be said that it is the
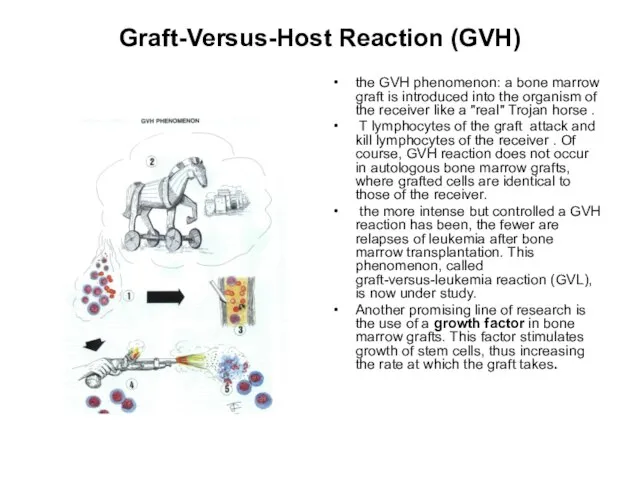
- 12. Graft-Versus-Host Reaction (GVH) the GVH phenomenon: a bone marrow graft is introduced into the organism of
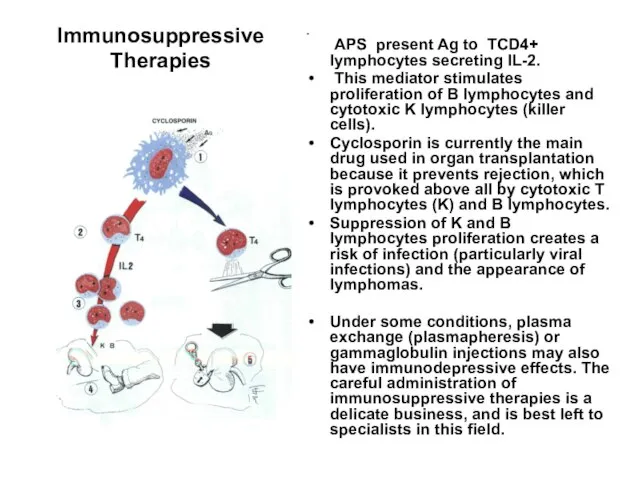
- 13. Immunosuppressive Therapies The main indications for immunosuppressive therapy are organ transplantation and autoimmune diseases. The first
- 14. Immunosuppressive Therapies APS present Ag to TCD4+ lymphocytes secreting IL-2. This mediator stimulates proliferation of B
- 15. Immune Response to Pregnancy (Alloimmunity) Function: to alert the mother to react to the baby as
- 16. There are five categories of immune problems that can cause pregnancy loss, IVF failures and infertility.
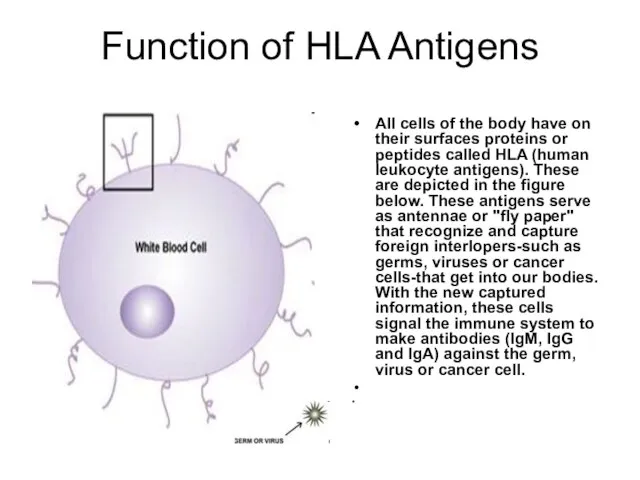
- 17. Function of HLA Antigens All cells of the body have on their surfaces proteins or peptides
- 18. A pregnancy must also be recognized as a foreign being (father puts HLA antigens on the
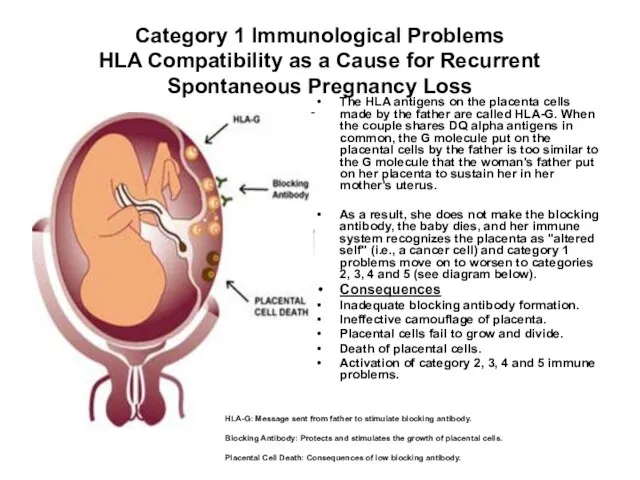
- 19. Category 1 Immunological Problems HLA Compatibility as a Cause for Recurrent Spontaneous Pregnancy Loss The HLA
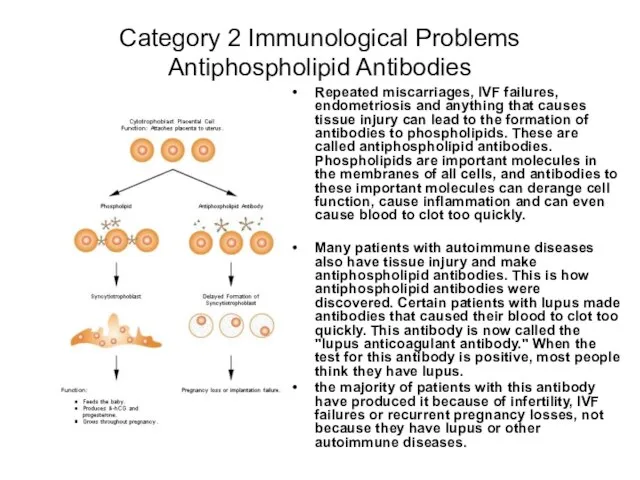
- 20. Category 2 Immunological Problems Antiphospholipid Antibodies Repeated miscarriages, IVF failures, endometriosis and anything that causes tissue
- 21. The incidence of this problem increases in women by 15% with each pregnancy that is lost.
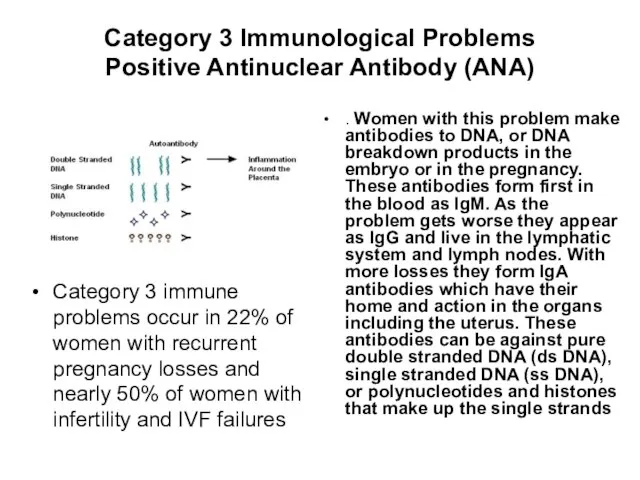
- 22. Category 3 Immunological Problems Positive Antinuclear Antibody (ANA) Category 3 immune problems occur in 22% of
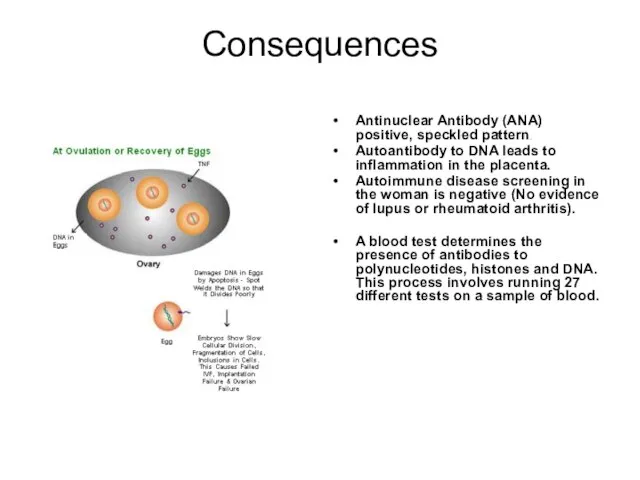
- 23. Consequences Antinuclear Antibody (ANA) positive, speckled pattern. Autoantibody to DNA leads to inflammation in the placenta.
- 24. Positive Antinuclear Antibody (ANA) Diagnosis The presence of antibodies is also tested for by doing the
- 25. Positive Antinuclear Antibody (ANA) Diagnosis (2) These same antibodies appear positive in women with lupus, rheumatoid
- 26. Category 4 Immunological Problems Autoimmune Response to Sperm Antigen 10% of women with infertility, implantation failures
- 27. Autoimmune Response to Sperm Antigen (2) Being exposed to antibody coated sperm dispensed by the male
- 28. Consequences Sperm antibody test positive. Sperm antibody positive by flow cytometer. Couple is unable to conceive
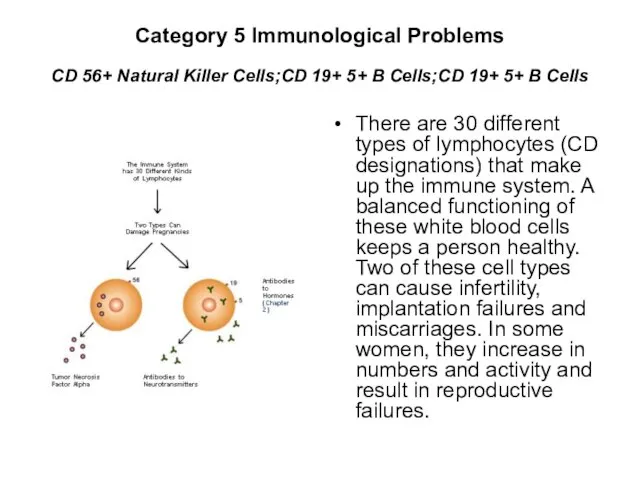
- 29. Category 5 Immunological Problems CD 56+ Natural Killer Cells;CD 19+ 5+ B Cells;CD 19+ 5+ B
- 30. Involved lyphocytes types TH-2 ("T Helper 2") The response is a balanced correct response during pregnancy
- 31. CD 56+ Natural Killer Cells Problem Increase in number 2-12% normal. Above 12% see infertility and
- 32. CD 56+ Natural Killer Cells Consequences Prevent implantation. Cause miscarriages by damaging the placental cells, causing
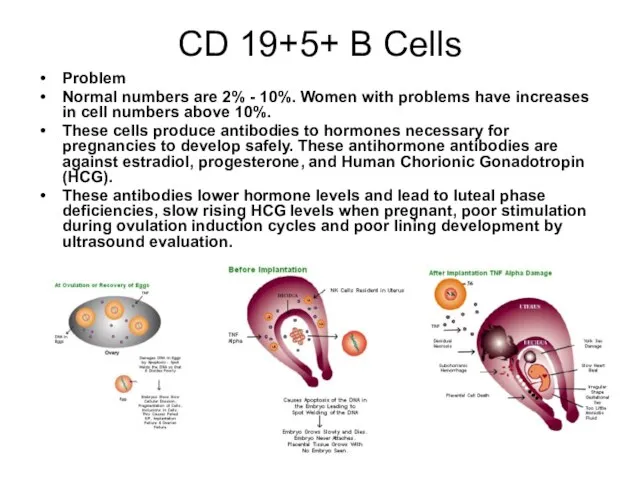
- 33. CD 19+5+ B Cells Problem Normal numbers are 2% - 10%. Women with problems have increases
- 34. CD 19+5+ B Cells Consequences Resistant ovary syndrome or premature ovarian failure. Day 3 FSH and
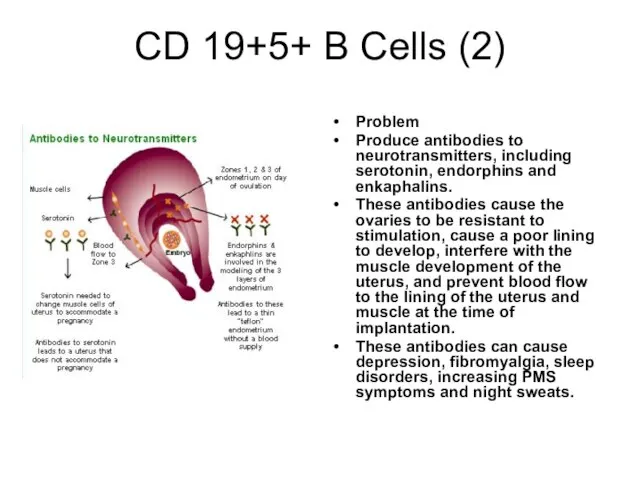
- 35. CD 19+5+ B Cells (2) Problem Produce antibodies to neurotransmitters, including serotonin, endorphins and enkaphalins. These
- 37. Скачать презентацию
Слайд 2Transplantation immunology
is getting increasingly important, from a clinical point of view,
now
Transplantation immunology
is getting increasingly important, from a clinical point of view,
now
Слайд 3The immunological barrier to transplantation
is determined by genetic differences between donor and
The immunological barrier to transplantation
is determined by genetic differences between donor and
Слайд 4The HLA system
consists of membrane proteins, divided in two classes: Class I
The HLA system
consists of membrane proteins, divided in two classes: Class I
Слайд 5The HLA system (cont-d)
Class I antigens are present on most nucleated cells,
The HLA system (cont-d)
Class I antigens are present on most nucleated cells,
Слайд 6Clinical considerations
even sister may be with an identical HLA formula. As
Clinical considerations
even sister may be with an identical HLA formula. As
Слайд 7transplantation between a donor and receiver which are not identical for their
transplantation between a donor and receiver which are not identical for their
Слайд 8Rejection mechanism
is quite complicated.
recognition of MHC antigens
directly encountered in
Rejection mechanism
is quite complicated.
recognition of MHC antigens
directly encountered in
Слайд 9Rejection mechanism (2)
All these mechanisms lead to rejection of the transplanted
Rejection mechanism (2)
All these mechanisms lead to rejection of the transplanted
Слайд 10Possible ways of prophylaxis
A first step
reducing as much as possible the
Possible ways of prophylaxis
A first step
reducing as much as possible the
Слайд 11Graft-Versus-Host Reaction (GVH)
In this type of reaction, it could be said that
Graft-Versus-Host Reaction (GVH)
In this type of reaction, it could be said that
Слайд 12Graft-Versus-Host Reaction (GVH)
the GVH phenomenon: a bone marrow graft is introduced into
Graft-Versus-Host Reaction (GVH)
the GVH phenomenon: a bone marrow graft is introduced into
Слайд 13Immunosuppressive Therapies
The main indications for immunosuppressive therapy
are organ transplantation and autoimmune
Immunosuppressive Therapies
The main indications for immunosuppressive therapy
are organ transplantation and autoimmune
Слайд 14Immunosuppressive Therapies
APS present Ag to TCD4+ lymphocytes secreting IL-2.
This mediator
Immunosuppressive Therapies
APS present Ag to TCD4+ lymphocytes secreting IL-2.
This mediator
Слайд 15Immune Response to Pregnancy (Alloimmunity)
Function: to alert the mother to react to
Immune Response to Pregnancy (Alloimmunity)
Function: to alert the mother to react to
Слайд 16There are five categories of immune problems that can cause pregnancy loss,
Слайд 17Function of HLA Antigens
All cells of the body have on their surfaces
Function of HLA Antigens
All cells of the body have on their surfaces
Слайд 18A pregnancy must also be recognized as a foreign being (father puts
A pregnancy must also be recognized as a foreign being (father puts
Слайд 19Category 1 Immunological Problems
HLA Compatibility as a Cause for Recurrent Spontaneous
Category 1 Immunological Problems HLA Compatibility as a Cause for Recurrent Spontaneous
Слайд 20Category 2 Immunological Problems
Antiphospholipid Antibodies
Repeated miscarriages, IVF failures, endometriosis and anything
Category 2 Immunological Problems
Antiphospholipid Antibodies
Repeated miscarriages, IVF failures, endometriosis and anything
Слайд 21The incidence of this problem increases in women by 15% with each
The incidence of this problem increases in women by 15% with each
Слайд 22Category 3 Immunological Problems
Positive Antinuclear Antibody (ANA)
Category 3 immune problems occur
Category 3 Immunological Problems
Positive Antinuclear Antibody (ANA)
Category 3 immune problems occur
Слайд 23Consequences
Antinuclear Antibody (ANA) positive, speckled pattern.
Autoantibody to DNA leads to inflammation in
Consequences
Antinuclear Antibody (ANA) positive, speckled pattern.
Autoantibody to DNA leads to inflammation in
Слайд 24Positive Antinuclear Antibody (ANA)
Diagnosis
The presence of antibodies is also tested for by
Positive Antinuclear Antibody (ANA)
Diagnosis
The presence of antibodies is also tested for by
Слайд 25Positive Antinuclear Antibody (ANA)
Diagnosis (2)
These same antibodies appear positive in women with
Positive Antinuclear Antibody (ANA)
Diagnosis (2)
These same antibodies appear positive in women with
Слайд 26Category 4 Immunological Problems
Autoimmune Response to Sperm Antigen
10% of women with
Category 4 Immunological Problems
Autoimmune Response to Sperm Antigen
10% of women with
Слайд 27Autoimmune Response to Sperm Antigen (2)
Being exposed to antibody coated sperm dispensed
Autoimmune Response to Sperm Antigen (2)
Being exposed to antibody coated sperm dispensed
Слайд 28Consequences
Sperm antibody test positive.
Sperm antibody positive by flow cytometer.
Couple is unable to
Consequences
Sperm antibody test positive.
Sperm antibody positive by flow cytometer.
Couple is unable to
Слайд 29Category 5 Immunological Problems
CD 56+ Natural Killer Cells;CD 19+ 5+ B Cells;CD
Category 5 Immunological Problems CD 56+ Natural Killer Cells;CD 19+ 5+ B Cells;CD
Слайд 30Involved lyphocytes types
TH-2 ("T Helper 2")
The response is a balanced correct response
Involved lyphocytes types
TH-2 ("T Helper 2")
The response is a balanced correct response
Слайд 31CD 56+ Natural Killer Cells
Problem
Increase in number 2-12% normal. Above
CD 56+ Natural Killer Cells
Problem
Increase in number 2-12% normal. Above
Слайд 32CD 56+ Natural Killer Cells
Consequences
Prevent implantation.
Cause miscarriages by damaging the placental
CD 56+ Natural Killer Cells
Consequences
Prevent implantation.
Cause miscarriages by damaging the placental
Слайд 33CD 19+5+ B Cells
Problem
Normal numbers are 2% - 10%. Women
CD 19+5+ B Cells
Problem
Normal numbers are 2% - 10%. Women
Слайд 34CD 19+5+ B Cells
Consequences
Resistant ovary syndrome or premature ovarian failure. Day
CD 19+5+ B Cells
Consequences
Resistant ovary syndrome or premature ovarian failure. Day
Слайд 35CD 19+5+ B Cells (2)
Problem
Produce antibodies to neurotransmitters, including serotonin, endorphins
CD 19+5+ B Cells (2)
Problem
Produce antibodies to neurotransmitters, including serotonin, endorphins
 ПОРЯДОК
ПОРЯДОК Место компьютера в современном мире
Место компьютера в современном мире Комплексные числа и арифметические операции над ними.
Комплексные числа и арифметические операции над ними. Горное дело
Горное дело Орнаменты ханты и священные изображения
Орнаменты ханты и священные изображения Взаимосвязь объектов в архитектурном макете
Взаимосвязь объектов в архитектурном макете Модели и типы обучения
Модели и типы обучения  Рецензия на картину Рафаэдя Санти "Сикстинская Мадонна"
Рецензия на картину Рафаэдя Санти "Сикстинская Мадонна" Бабочкина почта
Бабочкина почта Презентация на тему Зима (1 класс)
Презентация на тему Зима (1 класс) SEZUAL зрение для слепых
SEZUAL зрение для слепых ARRP и RARP Топологии Маршрутизаторы Cisco
ARRP и RARP Топологии Маршрутизаторы Cisco Предмет, методы, система экологического права как отрасли права
Предмет, методы, система экологического права как отрасли права Русская ярмарка (3 класс)
Русская ярмарка (3 класс) Твои игрушки
Твои игрушки Музей боевой славы (Иркутск)
Музей боевой славы (Иркутск) Психологический портрет Лукьянова Егора
Психологический портрет Лукьянова Егора Аккредитация ОУ. Предмет "Технология"
Аккредитация ОУ. Предмет "Технология" Статическая и динамическая сцинтиграфия
Статическая и динамическая сцинтиграфия Московский велоклуб«32 спицы»www.32spokes.ru2011 г.
Московский велоклуб«32 спицы»www.32spokes.ru2011 г. Презентация на тему Финансовая математика
Презентация на тему Финансовая математика Пушкины Зинаида Тимофеевна и Борис Борисович
Пушкины Зинаида Тимофеевна и Борис Борисович Презентация на тему Что такое светская этика
Презентация на тему Что такое светская этика  СигналТерритория Детства от Монтессори-центра
СигналТерритория Детства от Монтессори-центра НОРМАТИВНО-ПРАВОВОЕ ОБЕСПЕЧЕНИЕ ВВЕДЕНИЯ ФГОС НОО В ОУ
НОРМАТИВНО-ПРАВОВОЕ ОБЕСПЕЧЕНИЕ ВВЕДЕНИЯ ФГОС НОО В ОУ Понятие о причастии
Понятие о причастии Квиллинг для начинающих
Квиллинг для начинающих Введение в непрерывную интеграцию
Введение в непрерывную интеграцию