- Lecture Туб бренд укор

Содержание
- 2. Lung tuberculoma Lung tuberculoma unites etiologically various capsulated caseous foci of more than 1 cm in
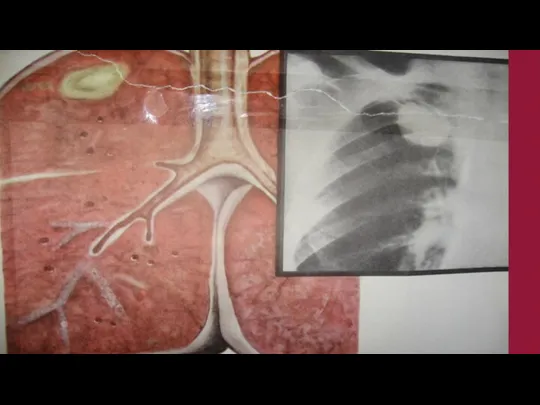
- 4. THE LUNG TUBERCULOMA The lung tuberculoma has the distinctive original clinical and anatomical display of secondary
- 5. CONDITIONS FOR FORMATION OF TUBERCULOMAS Physically active people. Decreased virulence and pathogenicity of Mycobacterium. Increased resistance
- 6. The source of tuberculoma formation is mainly of two forms of pulmonary tuberculosis: infiltrative-pneumonic and focal.
- 7. PATHOMORPHOLOGICAL CLASSIFICATION OF TUBERCULOMAS. Infiltrative-pneumonic tuberculoma Caseoma Pseudotuberculoma
- 8. INFILTRATIVE-PNEUMONIC TUBERCULOMA Presents as a round focus of pneumonia, containing masses of clotty necrosis, clearly limited
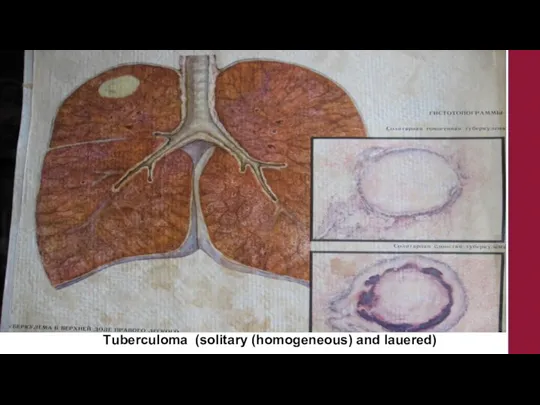
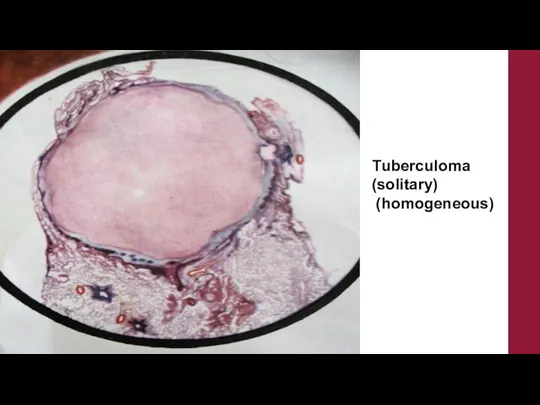
- 9. CASEOMA Big focus of caseous pneumonia surrounded by a fresh capsule. Types: Solitary homogenic caseoma (massive
- 10. Тuberculoma (solitary (homogeneous) and lauered)
- 11. Тuberculoma (solitary) (homogeneous)
- 12. Conglomerated tuberculema
- 13. Lauered tuberculoma
- 14. PSEUDOTUBERCULOMA Only revealed in case of dynamic observation of the patient and histological examination of material
- 15. There are three clinical variants of tuberculoma course: 1. progressing, described by occurrence of disintegration at
- 16. Variants of the tuberculema aggravation: 1) development of the perifocal inflammation; 2) cavitation - discharge of
- 17. 2. stable – absence of tuberculoma X-ray changes or rare aggravations without signs of tuberculoma progressing;
- 18. 3. regressing tuberculoma is characterized by its slow reduction in size, with subsequent formation of focus
- 19. PREVALENCE OF TUBERCULOMA The prevalence of tuberculoma among all forms of pulmonary tuberculosis is 6-10 %.
- 20. Clinical pattern As tuberculoma itself is a parameter of high body resistance, patients with this form
- 21. Physical examination At physical examination of a patient, there are no pathological signs in lungs. Crackles
- 22. CURRENT OF THE DISEASE Start of the disease: Debut of the disease is asymptomatic. The method
- 23. CURRENT OF THE DISEASE Period of progression: Moderate expression of symptoms of tuberculous intoxication. Appearance of
- 24. CURRENT OF THE DISEASE Period of regression: Reversal of symptoms. The tuberculoma gradually decreases in size,
- 25. Physical examination At physical examination of a patient, there are no pathological signs in lungs. Crackles
- 26. X-ray picture of tuberculoma X-ray image of tuberculoma looks like rounded shadow with precise contours. Inside
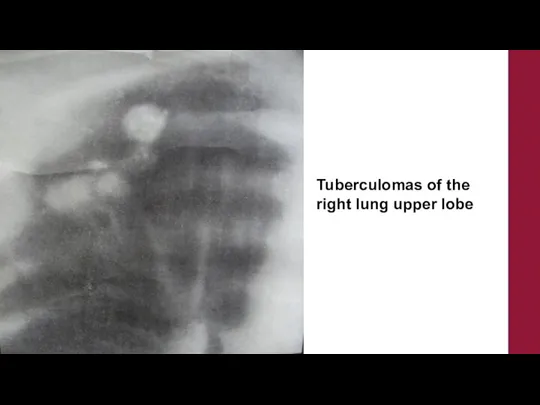
- 28. Tuberculomas of the right lung upper lobe
- 29. TUBERCULOMA IN THE PHASE OF DISINTERGRATION Characterised by eccentric locaiisation of semi-lunar shaped or beam-shaped zones
- 31. Tuberculoma of the left lung (upper lobe)
- 32. Tuberculoma of the left lung (upper lobe)
- 33. Tuberculoma of the right lung (upper lobe)
- 34. Tuberculoma of the right lung (upper lobe) in the phase of disintegration
- 36. Tuberculoma of the left lung in the phase of disintegration
- 37. Tuberculoma of the right lung upper lobe
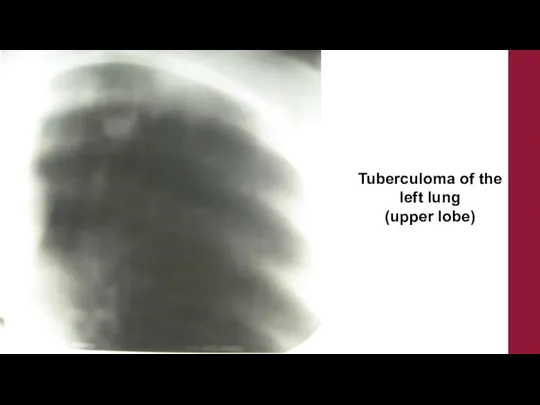
- 38. Tuberculoma of the left lung (upper lobe)
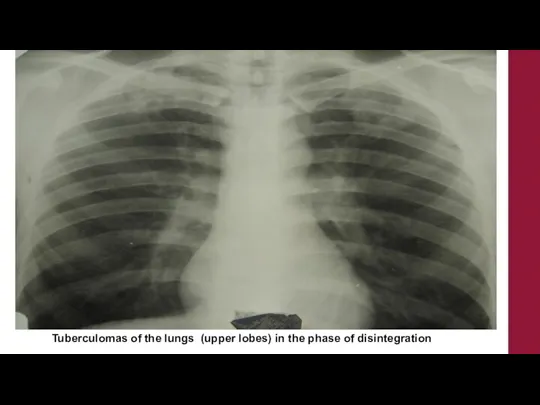
- 39. Tuberculomas of the lungs (upper lobes) in the phase of disintegration
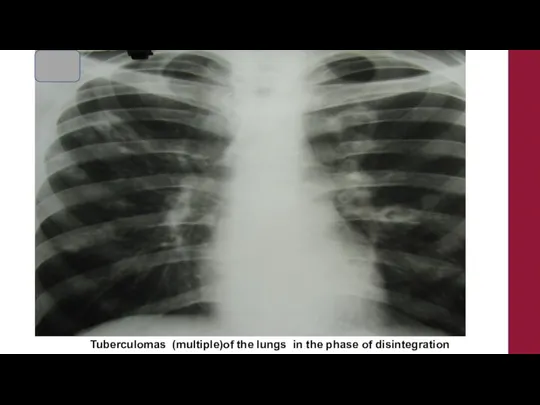
- 40. Tuberculomas (multiple)of the lungs in the phase of disintegration
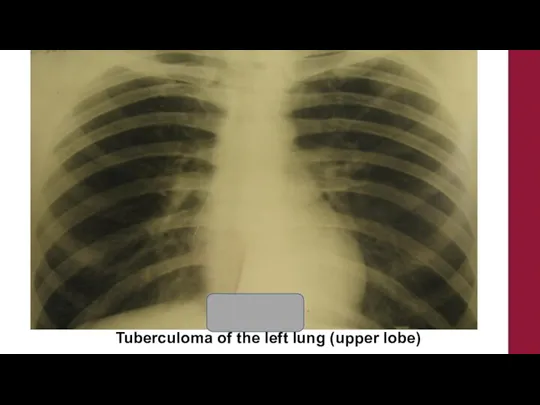
- 41. Tuberculoma of the left lung (upper lobe)
- 42. Tuberculoma of the right lung upper lobe
- 43. Pat. I.A.A, June. Tuberculoma of the left lung (upper lobe)
- 44. Pat. I.A.A. Tuberculoma of thе left lung upper lobe
- 45. Pat. I.A.A, October. Tuberculoma of the left lung In the phase of disintegration
- 46. Tomogram Tuberculoma of the left lung upper lobe
- 47. Pat E. Мultiple Tuberculomas. Diabetes Mellitiuos. MDR
- 48. Pat E Negative Dynamics Diabetes Mellitius. MDR
- 49. Tuberculoma of the right lung (upper lobe) Pat M. (July)
- 50. Pat M. March, ( 8 months later).
- 51. Pat M. March. Tomogram.
- 52. Pat M. March. Dynamics March - May
- 53. Tuberculoma of the left lung (upper lobe) Pat. G., May.
- 54. LABORATORY FINDINGS General blood analysis may reveal no significant changes: Lymphocytosis in 20% of the cases.
- 55. BLOOD PICTURE Blood picture is also without peculiarities. Sometimes moderate elevation of ESR and moderate leukocytosis
- 56. Mycobacterium tuberculosis Mycobacterium tuberculosis is not found in sputum at stable course of tuberculoma. Discharge of
- 57. Tuberculin tests Patients with lung tuberculoma in most cases positively react to tuberculin. Mantoux test is
- 58. Treatment Before the discovery of antituberculosis drugs, the forecast of tuberculoma was bad. Tuberculoma gave massive
- 59. Treatment When tuberculoma is diagnosed the patient must be hospitalized for long term treatment. Surgery is
- 60. TREATMENT General principles of treatment of TB patients but the antiTB drugs do not penetrate into
- 61. Chemotherapy
- 62. Surgical treatment. Usually operation is made with minimal removal of lung tissue. It is segmental resection.
- 63. Differential diagnostics
- 64. Differential diagnostics X-ray picture of tuberculoma is isolated rounded focus in lung tissue. It's typical for
- 65. Differential diagnostics It is necessary to collect detailed anamnesis, carefully examine all organs and systems of
- 66. Differential diagnostics For diagnosis of tuberculoma, Computer tomography bronchological examination with catheter biopsy and puncture of
- 67. Pat. T., May
- 68. Pat. T., December
- 69. Pat. T., February
- 70. Pat. T., September
- 71. Pat. T., September
- 72. Pat. T., September
- 73. Benign tumor
- 74. Pat. L., tomogram
- 75. Pat. L., 6 years later
- 76. Pat. L., Tomogram 6 years later
- 77. Pat. L., Profile X-ray
- 78. Pat. K. Echinococcus
- 79. Pat. K. Echinococcus Tomogram
- 80. Pat. G. Echinococcus
- 81. Pat. G. Echinococcus
- 82. Pat. G. Echinococcus Profile FiLm
- 83. Pat. G.. After operation
- 84. Pat. B. Echinococcus
- 85. Pat. L. Echinococcus Profile Film
- 86. Pat. Sh. . Enchondroma
- 87. Pat. Sh. . Enchondroma
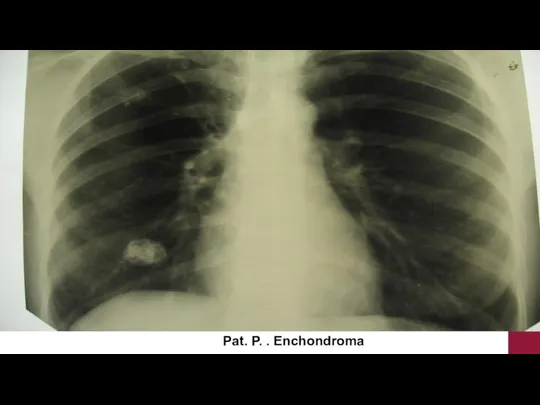
- 88. Pat. P. . Enchondroma
- 91. Скачать презентацию
Слайд 2Lung tuberculoma
Lung tuberculoma unites etiologically various capsulated caseous foci of more than
Lung tuberculoma
Lung tuberculoma unites etiologically various capsulated caseous foci of more than
Слайд 4THE LUNG TUBERCULOMA
The lung tuberculoma has the distinctive original clinical and anatomical
THE LUNG TUBERCULOMA
The lung tuberculoma has the distinctive original clinical and anatomical
Слайд 5 CONDITIONS FOR FORMATION OF TUBERCULOMAS
Physically active people.
Decreased virulence and pathogenicity of
CONDITIONS FOR FORMATION OF TUBERCULOMAS
Physically active people.
Decreased virulence and pathogenicity of
Слайд 6The source of tuberculoma formation
is mainly of two forms of pulmonary
The source of tuberculoma formation
is mainly of two forms of pulmonary
Слайд 7PATHOMORPHOLOGICAL CLASSIFICATION OF TUBERCULOMAS.
Infiltrative-pneumonic tuberculoma
Caseoma
Pseudotuberculoma
PATHOMORPHOLOGICAL CLASSIFICATION OF TUBERCULOMAS.
Infiltrative-pneumonic tuberculoma
Caseoma
Pseudotuberculoma
Слайд 8INFILTRATIVE-PNEUMONIC TUBERCULOMA
Presents as a round focus of pneumonia, containing masses of clotty
INFILTRATIVE-PNEUMONIC TUBERCULOMA
Presents as a round focus of pneumonia, containing masses of clotty
Слайд 9CASEOMA
Big focus of caseous pneumonia surrounded by a fresh capsule.
Types:
Solitary homogenic caseoma
CASEOMA
Big focus of caseous pneumonia surrounded by a fresh capsule.
Types:
Solitary homogenic caseoma
Слайд 10Тuberculoma (solitary (homogeneous) and lauered)
Тuberculoma (solitary (homogeneous) and lauered)
Слайд 11Тuberculoma
(solitary)
(homogeneous)
Тuberculoma
(solitary)
(homogeneous)
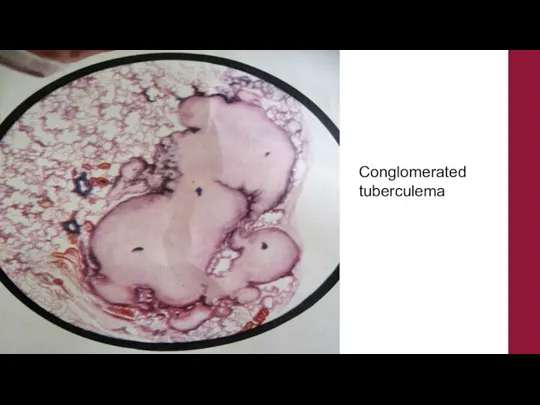
Слайд 12Conglomerated tuberculema
Conglomerated tuberculema
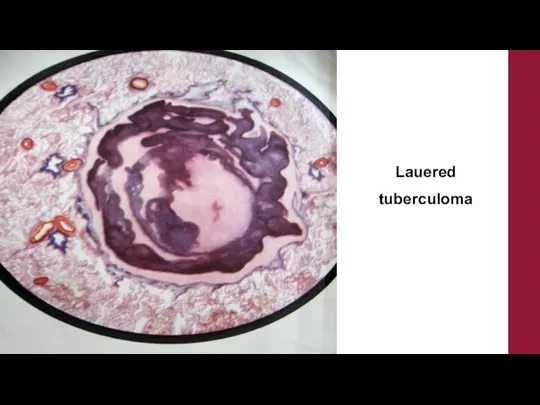
Слайд 13Lauered
tuberculoma
Lauered
tuberculoma
Слайд 14PSEUDOTUBERCULOMA
Only revealed in case of dynamic observation of the patient and histological
PSEUDOTUBERCULOMA
Only revealed in case of dynamic observation of the patient and histological
Слайд 15There are three clinical variants of tuberculoma course:
1. progressing,
described by
There are three clinical variants of tuberculoma course:
1. progressing,
described by
Слайд 16Variants of the tuberculema aggravation:
1) development of the perifocal inflammation;
2) cavitation - discharge of
Variants of the tuberculema aggravation:
1) development of the perifocal inflammation;
2) cavitation - discharge of
Слайд 17
2. stable –
absence of tuberculoma X-ray changes
or rare aggravations without signs
2. stable –
absence of tuberculoma X-ray changes
or rare aggravations without signs
Слайд 183. regressing tuberculoma
is characterized by its
slow reduction in size,
with
3. regressing tuberculoma
is characterized by its
slow reduction in size,
with
Слайд 19PREVALENCE OF TUBERCULOMA
The prevalence of tuberculoma among all forms of pulmonary tuberculosis
PREVALENCE OF TUBERCULOMA
The prevalence of tuberculoma among all forms of pulmonary tuberculosis
Слайд 20Clinical pattern
As tuberculoma itself is a parameter of high body resistance, patients
Clinical pattern
As tuberculoma itself is a parameter of high body resistance, patients
Слайд 21Physical examination
At physical examination of a patient, there are no pathological signs
Physical examination
At physical examination of a patient, there are no pathological signs
Слайд 22CURRENT OF THE DISEASE
Start of the disease:
Debut of the disease is asymptomatic.
The
CURRENT OF THE DISEASE
Start of the disease:
Debut of the disease is asymptomatic.
The
Слайд 23CURRENT OF THE DISEASE
Period of progression:
Moderate expression of symptoms of tuberculous intoxication.
Appearance
CURRENT OF THE DISEASE
Period of progression:
Moderate expression of symptoms of tuberculous intoxication.
Appearance
Слайд 24CURRENT OF THE DISEASE
Period of regression:
Reversal of symptoms.
The tuberculoma gradually decreases in
CURRENT OF THE DISEASE
Period of regression:
Reversal of symptoms.
The tuberculoma gradually decreases in
Слайд 25Physical examination
At physical examination of a patient, there are no pathological signs
Physical examination
At physical examination of a patient, there are no pathological signs
Слайд 26X-ray picture of tuberculoma
X-ray image of tuberculoma looks like rounded shadow with
X-ray picture of tuberculoma
X-ray image of tuberculoma looks like rounded shadow with
Слайд 28Tuberculomas of the right lung upper lobe
Tuberculomas of the right lung upper lobe
Слайд 29TUBERCULOMA IN THE PHASE OF DISINTERGRATION
Characterised by eccentric locaiisation of semi-lunar shaped
TUBERCULOMA IN THE PHASE OF DISINTERGRATION
Characterised by eccentric locaiisation of semi-lunar shaped
Слайд 31Tuberculoma of the left lung (upper lobe)
Tuberculoma of the left lung (upper lobe)
Слайд 32Tuberculoma of the left lung (upper lobe)
Tuberculoma of the left lung (upper lobe)
Слайд 33 Tuberculoma of the right lung (upper lobe)
Tuberculoma of the right lung (upper lobe)
Слайд 34Tuberculoma of the right lung (upper lobe) in the phase of disintegration
Tuberculoma of the right lung (upper lobe) in the phase of disintegration
Слайд 36Tuberculoma of the left lung in the phase of disintegration
Tuberculoma of the left lung in the phase of disintegration
Слайд 37Tuberculoma of the right lung upper lobe
Tuberculoma of the right lung upper lobe
Слайд 38Tuberculoma of the left lung
(upper lobe)
Tuberculoma of the left lung
(upper lobe)
Слайд 39Tuberculomas of the lungs (upper lobes) in the phase of disintegration
Tuberculomas of the lungs (upper lobes) in the phase of disintegration
Слайд 40Tuberculomas (multiple)of the lungs in the phase of disintegration
Tuberculomas (multiple)of the lungs in the phase of disintegration
Слайд 41Tuberculoma of the left lung (upper lobe)
Tuberculoma of the left lung (upper lobe)
Слайд 42Tuberculoma of the right lung upper lobe
Tuberculoma of the right lung upper lobe
Слайд 43 Pat. I.A.A, June. Tuberculoma of the left lung (upper lobe)
Pat. I.A.A, June. Tuberculoma of the left lung (upper lobe)
Слайд 44 Pat. I.A.A.
Tuberculoma of thе left lung upper lobe
Pat. I.A.A.
Tuberculoma of thе left lung upper lobe
Слайд 45Pat. I.A.A, October. Tuberculoma of the left lung In the phase of
Pat. I.A.A, October. Tuberculoma of the left lung In the phase of
Слайд 46Tomogram
Tuberculoma of the left lung upper lobe
Tomogram
Tuberculoma of the left lung upper lobe
Слайд 47Pat E. Мultiple Tuberculomas. Diabetes Mellitiuos. MDR
Pat E. Мultiple Tuberculomas. Diabetes Mellitiuos. MDR
Слайд 48Pat E Negative Dynamics Diabetes Mellitius. MDR
Pat E Negative Dynamics Diabetes Mellitius. MDR
Слайд 49Tuberculoma of the right lung
(upper lobe)
Pat M. (July)
Tuberculoma of the right lung
(upper lobe)
Pat M. (July)
Слайд 50 Pat M. March, ( 8 months later).
Pat M. March, ( 8 months later).
Слайд 51 Pat M. March.
Tomogram.
Pat M. March.
Tomogram.
Слайд 52 Pat M. March. Dynamics March - May
Pat M. March. Dynamics March - May
Слайд 53Tuberculoma of the left lung (upper lobe) Pat. G., May.
Tuberculoma of the left lung (upper lobe) Pat. G., May.
Слайд 54LABORATORY FINDINGS
General blood analysis may reveal no significant changes:
Lymphocytosis in 20%
LABORATORY FINDINGS
General blood analysis may reveal no significant changes:
Lymphocytosis in 20%
Слайд 55BLOOD PICTURE
Blood picture is also without peculiarities.
Sometimes moderate elevation of ESR
BLOOD PICTURE
Blood picture is also without peculiarities.
Sometimes moderate elevation of ESR
Слайд 56Mycobacterium tuberculosis
Mycobacterium tuberculosis is not found in sputum at stable course of
Mycobacterium tuberculosis
Mycobacterium tuberculosis is not found in sputum at stable course of
Слайд 57Tuberculin tests
Patients with lung tuberculoma in most cases positively react to
Tuberculin tests
Patients with lung tuberculoma in most cases positively react to
Слайд 58Treatment
Before the discovery of antituberculosis drugs, the forecast of tuberculoma was
Treatment
Before the discovery of antituberculosis drugs, the forecast of tuberculoma was
Слайд 59Treatment
When tuberculoma is diagnosed the patient must be hospitalized for long term
Treatment
When tuberculoma is diagnosed the patient must be hospitalized for long term
Слайд 60TREATMENT
General principles of treatment of TB patients but the antiTB drugs do
TREATMENT
General principles of treatment of TB patients but the antiTB drugs do
Слайд 61Chemotherapy
Chemotherapy

Слайд 62Surgical treatment.
Usually operation is made with minimal removal of lung tissue. It
Surgical treatment.
Usually operation is made with minimal removal of lung tissue. It
Слайд 63Differential diagnostics
Differential diagnostics
Слайд 64Differential diagnostics
X-ray picture of tuberculoma is isolated rounded focus in lung
Differential diagnostics
X-ray picture of tuberculoma is isolated rounded focus in lung
Слайд 65Differential diagnostics
It is necessary
to collect detailed anamnesis,
carefully examine all
Differential diagnostics
It is necessary
to collect detailed anamnesis,
carefully examine all
Слайд 66Differential diagnostics
For diagnosis of tuberculoma,
Computer tomography
bronchological examination with catheter biopsy and
Differential diagnostics
For diagnosis of tuberculoma,
Computer tomography
bronchological examination with catheter biopsy and
Слайд 67Pat. T., May
Pat. T., May
Слайд 68Pat. T., December
Pat. T., December
Слайд 69 Pat. T., February
Pat. T., February
Слайд 70 Pat. T.,
September
Pat. T.,
September
Слайд 71 Pat. T.,
September
Pat. T.,
September
Слайд 72 Pat. T.,
September
Pat. T.,
September
Слайд 73Benign tumor
Слайд 74 Pat. L.,
tomogram
Pat. L.,
tomogram

Слайд 75 Pat. L.,
6 years later
Pat. L.,
6 years later
Слайд 76 Pat. L.,
Tomogram
6 years later
Pat. L.,
Tomogram
6 years later
Слайд 77 Pat. L.,
Profile X-ray
Pat. L.,
Profile X-ray
Слайд 78Pat. K.
Echinococcus
Pat. K.
Echinococcus
Слайд 79Pat. K.
Echinococcus
Tomogram
Pat. K.
Echinococcus
Tomogram
Слайд 80Pat. G.
Echinococcus
Pat. G.
Echinococcus
Слайд 81Pat. G.
Echinococcus
Pat. G.
Echinococcus
Слайд 82Pat. G.
Echinococcus
Profile FiLm
Pat. G.
Echinococcus
Profile FiLm
Слайд 83Pat. G..
After operation
Pat. G..
After operation
Слайд 84Pat. B. Echinococcus
Pat. B. Echinococcus
Слайд 85Pat. L. Echinococcus
Profile Film
Pat. L. Echinococcus
Profile Film
Слайд 86Pat. Sh. . Enchondroma
Pat. Sh. . Enchondroma
Слайд 87Pat. Sh. . Enchondroma
Pat. Sh. . Enchondroma
Слайд 88Pat. P. . Enchondroma
Pat. P. . Enchondroma

 Общая психология. Тест по темам: воображение, мышление, речь, внимание
Общая психология. Тест по темам: воображение, мышление, речь, внимание Дом моей мечты
Дом моей мечты Аппаратные новинки ПК
Аппаратные новинки ПК Бизнес план
Бизнес план 12 психотипов, которые живут рядом с нами
12 психотипов, которые живут рядом с нами Программирование на стороне сервера
Программирование на стороне сервера Марс
Марс Многочлены с одной переменной
Многочлены с одной переменной Благотворные и зловредные планеты
Благотворные и зловредные планеты Исполнитель Робот
Исполнитель Робот Магнитогорский государственный университет
Магнитогорский государственный университет г.о. Тольятти 2012 г.
г.о. Тольятти 2012 г. Ультразвуковое сверление металла
Ультразвуковое сверление металла Питание является основным фактором, определяющим самочувствие
Питание является основным фактором, определяющим самочувствие Основной закон государства
Основной закон государства Половое размножение растений
Половое размножение растений 102-р сургууль Ж. Нарантуяа
102-р сургууль Ж. Нарантуяа Деньги. Виды денег
Деньги. Виды денег Развитие многоязычия в Интернете – новое направление деятельности Российского комитета Программы ЮНЕСКО «Информация для всех»
Развитие многоязычия в Интернете – новое направление деятельности Российского комитета Программы ЮНЕСКО «Информация для всех»  Вентиляционная труба DN300
Вентиляционная труба DN300 Проведение собеседований
Проведение собеседований Тест по произведению М.Ю.Лермонтова «Песня про царя Ивана Васильевича, молодого опричника и удалого купца Калашникова
Тест по произведению М.Ю.Лермонтова «Песня про царя Ивана Васильевича, молодого опричника и удалого купца Калашникова Воскресная школа для детей
Воскресная школа для детей Влияние ЕГЭна систему образования: доступность, эффективность, качество
Влияние ЕГЭна систему образования: доступность, эффективность, качество СТАНДАРТЫ ВТОРОГО ПОКОЛЕНИЯ
СТАНДАРТЫ ВТОРОГО ПОКОЛЕНИЯ СОЗДАНИЕ НАЦИОНАЛЬНОЙ СИСТЕМЫ АККРЕДИТАЦИИВ ОБЛАСТИ ПОДТВЕРЖДЕНИЯ СООТВЕТСТВИЯ В РОССИЙСКОЙ ФЕДЕРАЦИИ
СОЗДАНИЕ НАЦИОНАЛЬНОЙ СИСТЕМЫ АККРЕДИТАЦИИВ ОБЛАСТИ ПОДТВЕРЖДЕНИЯ СООТВЕТСТВИЯ В РОССИЙСКОЙ ФЕДЕРАЦИИ Приостановление выпуска товаров, содержащих объекты интеллектуальной собственности Подготовила студентка 3 курса ЮФ группы Ю-113Б
Приостановление выпуска товаров, содержащих объекты интеллектуальной собственности Подготовила студентка 3 курса ЮФ группы Ю-113Б Конкурс цифровых образовательных ресурсов
Конкурс цифровых образовательных ресурсов