- GI Hemorrhage

Содержание
- 2. LOWER GI BLEEDING Definition: LGIB is defined as bleeding from a source distal to the ligament
- 3. LGI hemorrhage Sites Colon – 95-97% Small bowel – 3-5% Only 15% of massive GI bleeding
- 4. LGI hemorrhage Etiology Diverticulosis – 40-55% Right sided lesions > left 90% stop spontaneously 10% rebleed
- 5. LGI hemorrhage diagnostics Large caliber NGT on admission Colonoscopy Within 12 hours in stable patients without
- 7. CONCLUSION LGIB requires pre op localization to detect the bleeding source , including rectoscopy, colonoscopy,angography and
- 9. Скачать презентацию
Слайд 3LGI hemorrhage
Sites
Colon – 95-97%
Small bowel – 3-5%
Only 15% of massive GI bleeding
Finding
LGI hemorrhage
Sites
Colon – 95-97%
Small bowel – 3-5%
Only 15% of massive GI bleeding
Finding
Слайд 4LGI hemorrhage
Etiology
Diverticulosis – 40-55%
Right sided lesions > left
90% stop spontaneously
10% rebleed in
LGI hemorrhage
Etiology
Diverticulosis – 40-55%
Right sided lesions > left
90% stop spontaneously
10% rebleed in
Слайд 5LGI hemorrhage diagnostics
Large caliber NGT on admission
Colonoscopy
Within 12 hours in stable patients
LGI hemorrhage diagnostics
Large caliber NGT on admission
Colonoscopy
Within 12 hours in stable patients

Слайд 7CONCLUSION
LGIB requires pre op localization to detect the bleeding source ,
CONCLUSION
LGIB requires pre op localization to detect the bleeding source ,
 Ренгенологічна діагностика сечової системи
Ренгенологічна діагностика сечової системи Коронавирусная инфекция. Меры профилактики
Коронавирусная инфекция. Меры профилактики Основы питания. Рекомендовано для обучающихся модульной программы основа ЗОЖ. 4 класс. Часть 1
Основы питания. Рекомендовано для обучающихся модульной программы основа ЗОЖ. 4 класс. Часть 1 Искусственный интеллект в медицине
Искусственный интеллект в медицине Кумбс пен Джелл бойынша жоғары сезімталдық механизмдері
Кумбс пен Джелл бойынша жоғары сезімталдық механизмдері Синдром Меллори-Вейса
Синдром Меллори-Вейса Невынашивание беременности. Преждевременные роды. Перенашивание беременности
Невынашивание беременности. Преждевременные роды. Перенашивание беременности Варикозное расширение вен органов малого таза у женщин
Варикозное расширение вен органов малого таза у женщин Возможности лечения БАС на современном этапе. Прогноз
Возможности лечения БАС на современном этапе. Прогноз Бронхиальная астма. Часть 2
Бронхиальная астма. Часть 2 Здоровый образ жизни - основа укрепления и сохранения личного здоровья
Здоровый образ жизни - основа укрепления и сохранения личного здоровья GEPATITY_ZAKLYuChITEL
GEPATITY_ZAKLYuChITEL Сальмонеллез
Сальмонеллез Проявления общих заболеваний в полости рта
Проявления общих заболеваний в полости рта Важность покрытия имплантата в стоматологии
Важность покрытия имплантата в стоматологии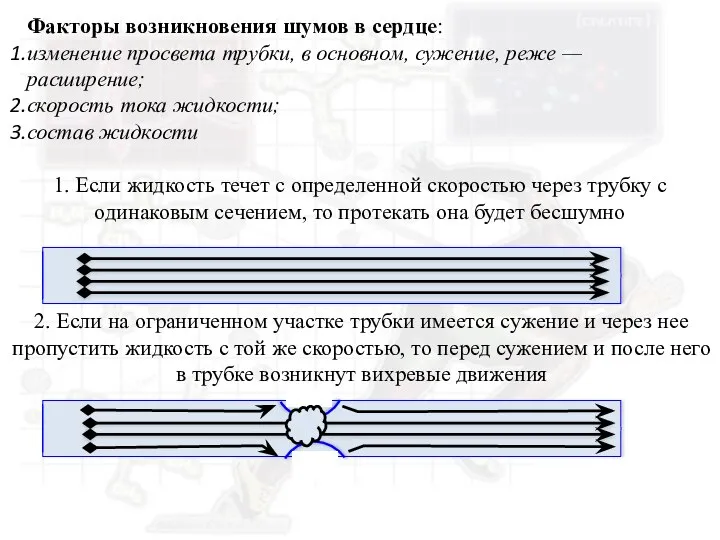 Факторы возникновения шумов в сердце
Факторы возникновения шумов в сердце Психопатологическая семиотика
Психопатологическая семиотика Туберкулез. Эпизоотология и инфекционные болезни
Туберкулез. Эпизоотология и инфекционные болезни Влияние психологических факторов на иммунитет и методы его восстановления
Влияние психологических факторов на иммунитет и методы его восстановления Наружные кровотечения. Лекция 3
Наружные кровотечения. Лекция 3 Речевые нарушения: Дислалия и дизартрия
Речевые нарушения: Дислалия и дизартрия Профилактика наркомании
Профилактика наркомании Образовательная программа профилактика ВИЧ-инфекции. Что должен знать о ВИЧ/СПИДе каждый?
Образовательная программа профилактика ВИЧ-инфекции. Что должен знать о ВИЧ/СПИДе каждый? БА -– это хроническое воспалительное заболевание дыхательных путей
БА -– это хроническое воспалительное заболевание дыхательных путей Компьютердін даму тарихы дулат
Компьютердін даму тарихы дулат Ноотропы и их применение в спорте
Ноотропы и их применение в спорте Синдром Клайнфельтера
Синдром Клайнфельтера Глаукома. Что такое глаукома?
Глаукома. Что такое глаукома?