Слайд 2Have you got an allergy on medicines?
Do you do physical exercises in
the morning?
Do you take cold shower in the morning?
Do you sleep well?
At what time do you usually wake up?
Слайд 3At what time do you usually go to bed?
How often do you

visit a doctor?
How often do you have low or high blood pressure?
Do you smoke?
Do you take drugs?
Слайд 4How often do you feel sick?
How often do you feel stressed?
Do you
do sport activities on a daily basis?
Do you train by yourself or with a help of a trainer?
How many cups of coffee do you drink everyday?
Слайд 5Do you drink enough water everyday?
Do you live in clean area with
fresh air?
How often do you use your car instead of going to a supermarket near house?
Do you try to reduce your bad habits?
How often do you eat junk food?

 Types of vaccines
Types of vaccines Пневмония. Виды пневмонии
Пневмония. Виды пневмонии Aliis inserviendo consumor
Aliis inserviendo consumor Правильное поведение в родах
Правильное поведение в родах Класс - суперабсорбирующие полимеры
Класс - суперабсорбирующие полимеры Патогены. Пищевые инфекции и отравления
Патогены. Пищевые инфекции и отравления Kosti_nizhnikh_konechnostei_774
Kosti_nizhnikh_konechnostei_774 Алгоритм назначения противоэпилептических препаратов на платформе Telegram и Viber
Алгоритм назначения противоэпилептических препаратов на платформе Telegram и Viber Лимфогранулематоз
Лимфогранулематоз Возможные причины и механизмы отклонений результатов КЛИ
Возможные причины и механизмы отклонений результатов КЛИ Планирование здравоохранения
Планирование здравоохранения Правильное питание - основа здорового образа жизни
Правильное питание - основа здорового образа жизни Виды медицинского страхования
Виды медицинского страхования Злокачественная гипертермия
Злокачественная гипертермия Симптомы аутизма в поведении
Симптомы аутизма в поведении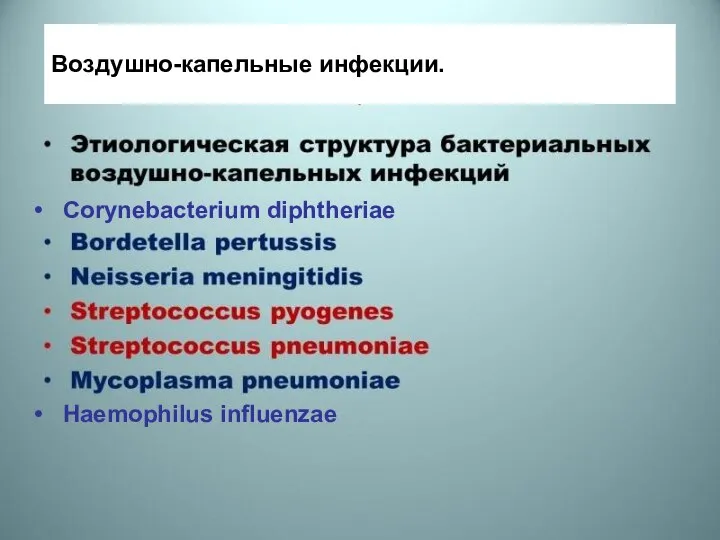 Воздушно-капельные инфекции
Воздушно-капельные инфекции Болезни сердечно-сосудистой системы. Перикардит
Болезни сердечно-сосудистой системы. Перикардит ВИЧ-инфекция, СПИД
ВИЧ-инфекция, СПИД Хейлиты метеорологические
Хейлиты метеорологические Қатерлі ісік сілекей бездері
Қатерлі ісік сілекей бездері Фурункулы. Источники инфекции
Фурункулы. Источники инфекции Введение в валеологию. Понятие здоровья. Лекция 1
Введение в валеологию. Понятие здоровья. Лекция 1 Медикаментозное лечение в сестринской практике (часть 1)
Медикаментозное лечение в сестринской практике (часть 1) Патология как наука. Понятие о здоровье и болезни. Основные категории патологии
Патология как наука. Понятие о здоровье и болезни. Основные категории патологии Вирусные пневмонии
Вирусные пневмонии COVID-19 за 2 сентября
COVID-19 за 2 сентября Отклонения. Что негативно влияет на содружество глазных яблок?
Отклонения. Что негативно влияет на содружество глазных яблок? Гнойно - септические заболевания в акушерстве и гинекологии
Гнойно - септические заболевания в акушерстве и гинекологии