- Physical medicine & rehabilitation & rheumatology or physiatry (rehabilitation medicine)

Содержание
- 2. Rehabilitation includes assisting the patient to compensate for deficits that cannot be reversed medically
- 3. Amputations, orthopedic injuries arthritis cardiac disease, cancer neurological problems, spinal cord injuries, stroke, & traumatic brain
- 4. GOALS Minimize functional deficits Use remaining function to maximum Prevent complications Minimize functional deficits Prevent complications
- 5. The key to Good Rehabilitation
- 6. Physician specialists head Rehabilitation teams including a The physical therapist. occupational therapist. The social workers. Rehabilitation
- 7. The physical therapist *The physical therapist assists the patient in functional restoration. *Tasks may include the
- 8. OCCUPATIONAL THERAPISTS Are responsible for those therapeutic activities associated with patient’s daily life, (ADL) from simple
- 10. Occupational therapy helps the patient regain the ability to do normal everyday tasks. This may be
- 11. Speech therapy helps the patient correct speech disorders or restore speech. Speech therapy may be prescribed
- 12. Key terms Orthotist — A health care professional who is skilled in making and fitting orthopedic
- 13. social worker A social worker help to Communicate the patient and family with the outside world.
- 14. Evaluation of the patient’s total Living Situation, Including Lifestyle, Family Finances, & Community resources.
- 15. Therapeutic Recreation Therapeutic Recreation implements various interventions as a form of treatment to increase physical, cognitive,
- 16. The Vocational rehabilitation program will assist in training and placing disabled persons in new jobs. Vocational
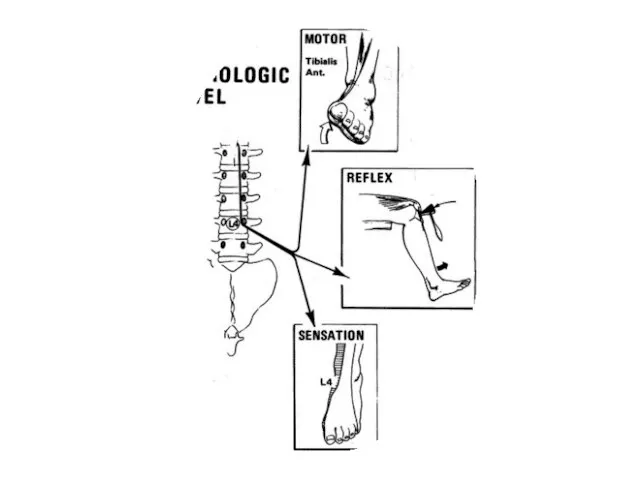
- 17. What diagnostic tools are used in physiatry medical history, physical examinations, X-rays. .Electromyography (EMG), nerve conduction
- 18. Physiatrists utilize Medications Injections. Physical modalities. Exercise. Education individualized to the patient`s needs. Assistive Devices
- 19. What Are Assistive الاجهزه المساعده Devices? Assistive devices can help a person function better and be
- 20. Many devices are available to help with activities of daily living (ADLs). ADLs are the normal
- 21. Hand Held Reacher Flexible Sock Aid Grip Drink Holder Grip Drink Holder
- 22. Bath Lift Bathroom Wheelchair Raised Toilet Seats Makes for an Easy On and Off the Toilet
- 23. What Are the Different Types of Mobility Aids? Mobility aids help with walking or moving from
- 24. Pediatric Walkers
- 26. NECK PAIN لواءاستاذ دكتور محمد رضا محمد عوض
- 31. Anatomy Head weighing 6:8 1b 7 cervical vertebrae 5 intervertebral discs 12 joints of Luschka 14
- 32. Prevalence Neck Stiffness 25 : 30 % Age 25-29 year Up to 50 % Age over
- 33. Musculosketetal Causes Osteoarthritis Diffuse idiopathic skeletal hyperstosis Cervical spondylosis Disk disease Rheumatoid arthritis Fracture Neoplasm Thoracic
- 34. Osteoarthritis
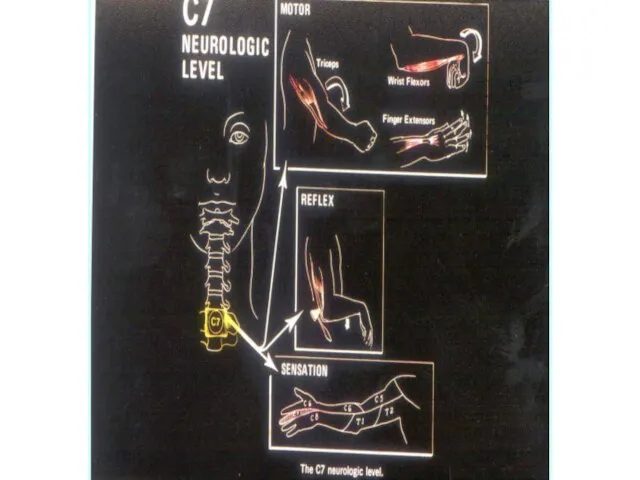
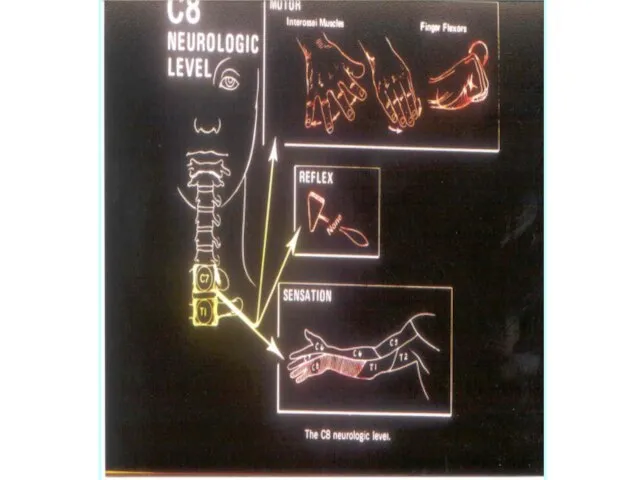
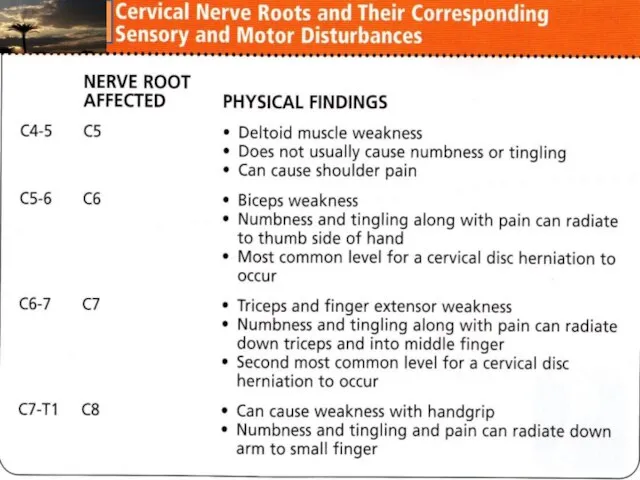
- 35. Neurological Causes Nerve root syndromes Cervical myelopathy Neuritis (brachial,occipital) Torticollis Meningitis Cord tumors
- 36. Soft tissue and muscular pain Acute cervical strain Cumulative trauma, overstrain syndromes Tendinitis, bursitis Postural disorders
- 37. whiplash injury or neck sprain injury The term “whiplash,” used to describe an injury mechanism of
- 38. The most common whiplash symptoms are neck pain, neck stiffness, headache, shoulder pain, back pain, and
- 39. Referred Pain Heart and coronary artery disease Apex of lung: Pancoast’s tumor Migraine Muscle tension and
- 40. Clinical Evaluation History Physical Examination Radiologic Evaluation Electro - Diagnosis (assist in confirming the clinical formulation)
- 41. Examination of Related Area Shoulder (Rotator Cuff Tendenitis – capsulitis) TMJ Upper Limb
- 47. Management
- 48. AIM Relief of pain and stiffness in the neck and arms Restore the function of neck
- 49. PATIENT EDUCATION various types of initial neck pain treatment with * analgesics, sedatives, antihistamines, nonsteroid anti-inflammatory
- 53. LUMBAR DISC PROLAPSE REDA AWAD
- 54. Second only to the common cold in frequency among adult ailments Fifth most common reason for
- 55. على المستوى المحلى 44 % من عمال الحديد والصلب . 34 % من سائقى أتوبيس النقل
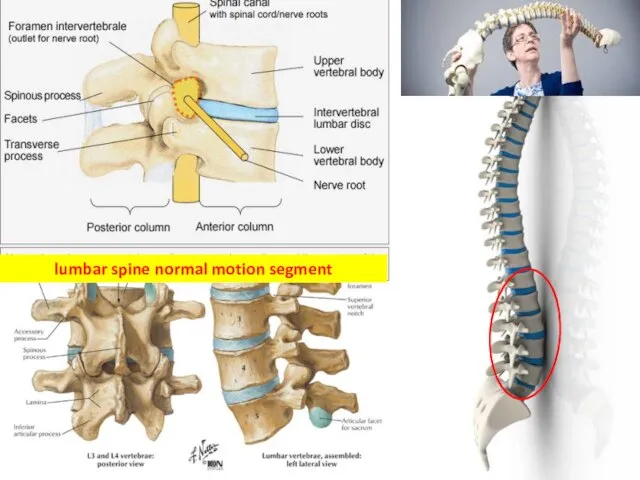
- 56. lumbar spine normal motion segment
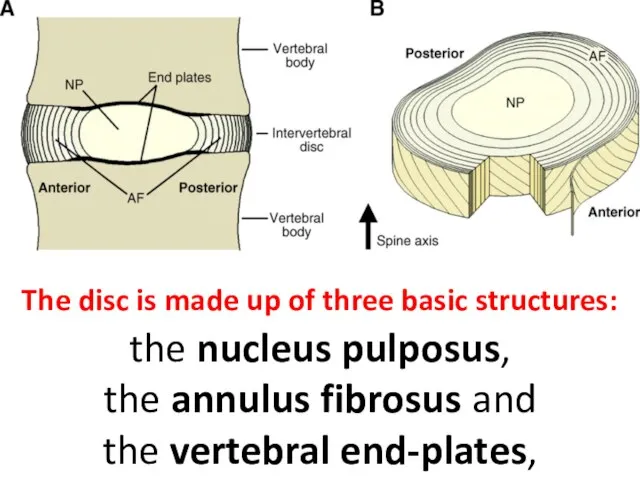
- 57. The disc is made up of three basic structures: the nucleus pulposus, the annulus fibrosus and
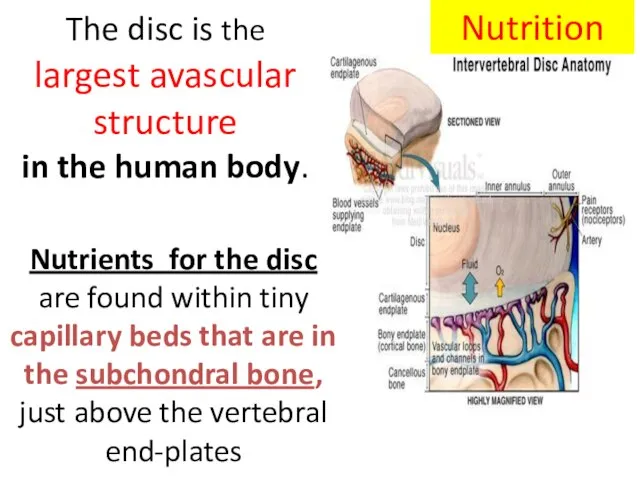
- 58. The disc is the largest avascular structure in the human body. Nutrition Nutrients for the disc
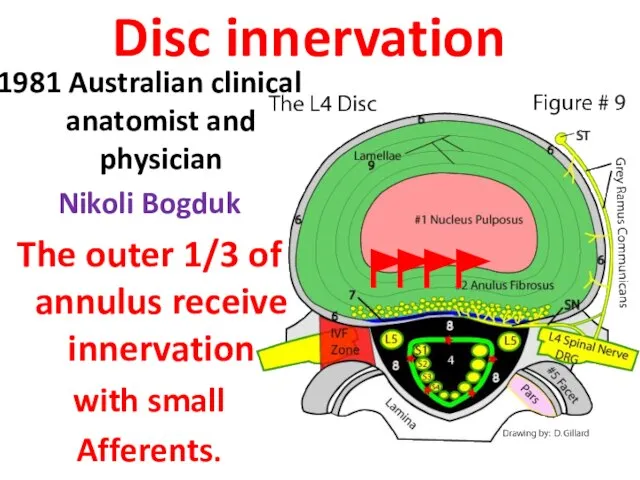
- 59. Disc innervation 1981 Australian clinical anatomist and physician Nikoli Bogduk The outer 1/3 of annulus receive
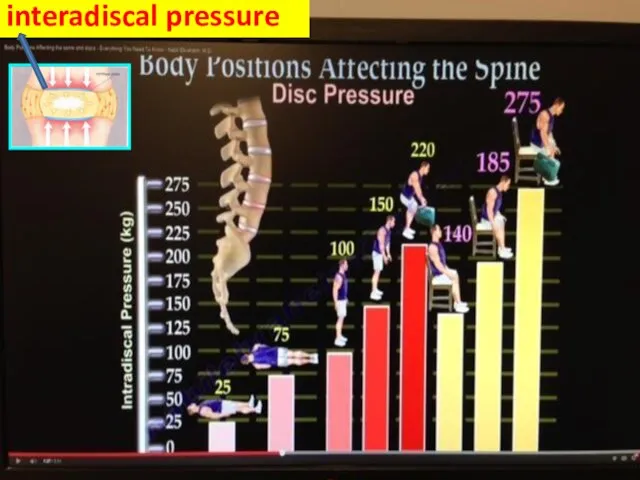
- 60. interadiscal pressure
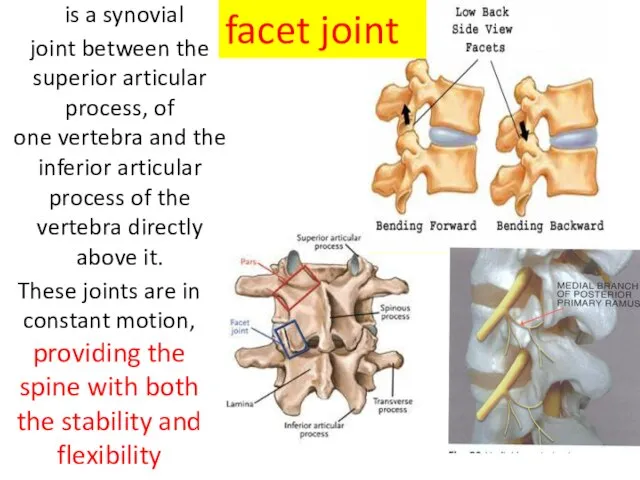
- 61. is a synovial joint between the superior articular process, of one vertebra and the inferior articular
- 62. Degeneration Before age 40 approximately 25%. Beyond age 40, more than 60% of people show evidence
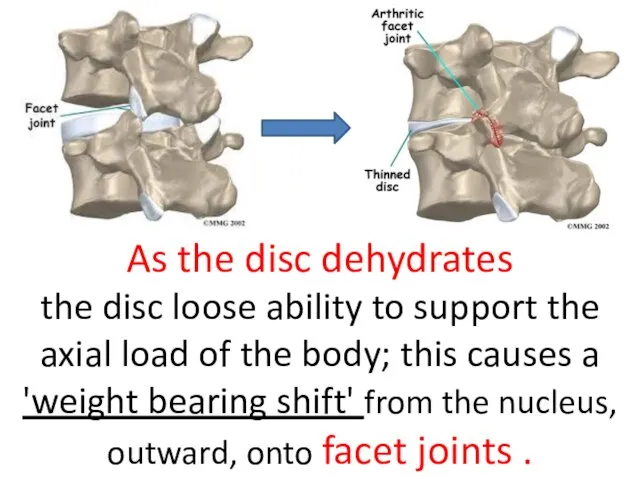
- 63. As the disc dehydrates the disc loose ability to support the axial load of the body;
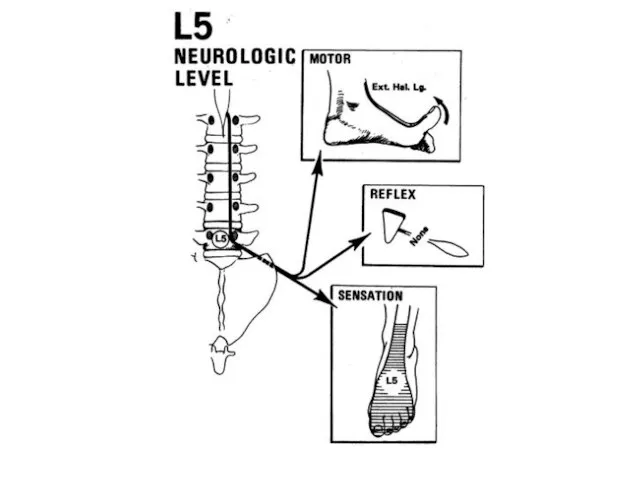
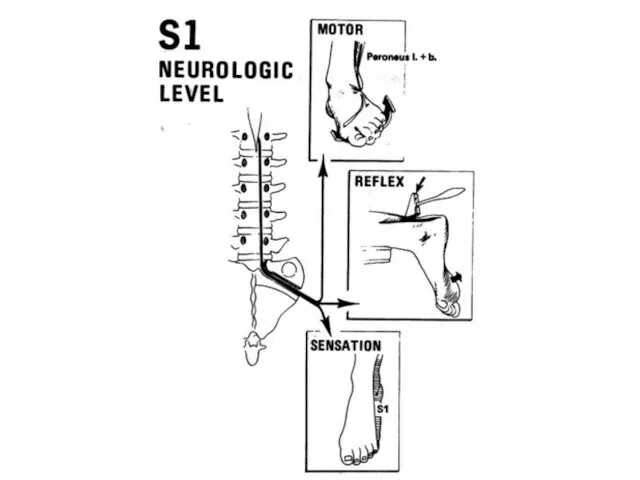
- 64. Recommendation 1 Clinicians should conduct a focused HISTORY& PHYSICAL EXAMINATION to help place patients with low
- 65. or back pain potentially associated with another Specific spinal causes 8% Nonspecific low back pain. 85%
- 66. Non-specific low back pain Pain, muscle tension, or stiffness that occurs between the( rib cage and
- 67. specific disorder,( 8%) such as cancer compression fracture spinal infection Ankylosing sp
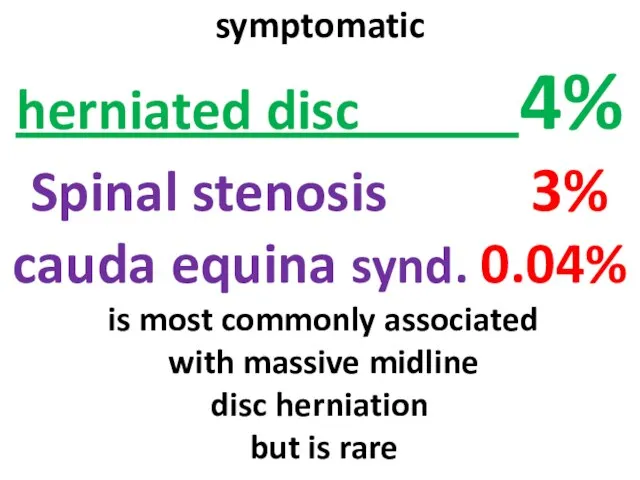
- 68. symptomatic herniated disc 4% Spinal stenosis 3% cauda equina synd. 0.04% is most commonly associated with
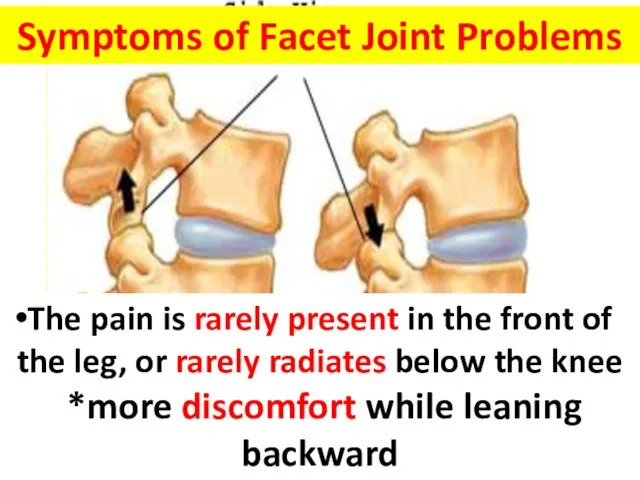
- 69. Symptoms of Facet Joint Problems a persisting point of tenderness overlying the inflamed facet pain from
- 70. History Physical Examination Radiologic Evaluation Electro - Diagnosis (assist in confirming the clinical formulation) Clinical Evaluation
- 74. The Diagnosis of back pain should be Based on a Good History and a Competent Physical
- 75. Imaging studies should be ordered in patient with : - progressive neurologic deficits - failure to
- 76. Goals *Relieve of pain *Restoration of physiological movements *Prevention of relapses
- 77. Surgery should be considered for * Individuals With Motor Weakness . * Persistant Radicular pain *Failure
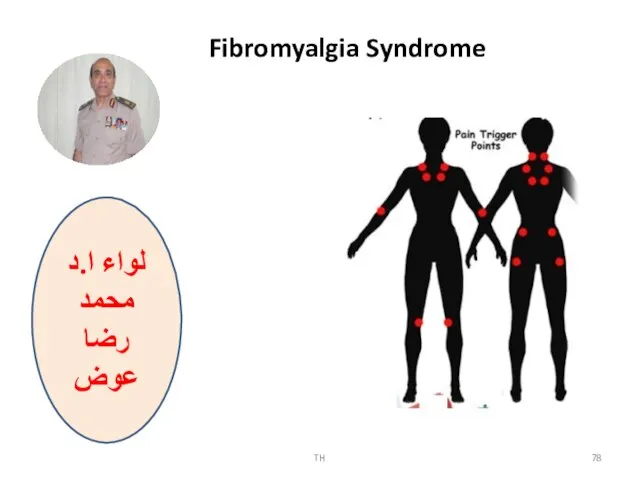
- 78. TH لواء ا.د محمد رضا عوض Fibromyalgia Syndrome
- 79. Typically presents with symptoms of diffuse body pain frequently involving the spinal region Neurologic Clinics -
- 80. Fibromyalgia is associated with : Fatigue Sleep disorder Anxiety , Depression Cognitive disturbance( memory and thinking
- 81. ACR 1990 Criteria for Fibromyalgia Widespread pain with a minimum duration of 3 months Both right
- 82. Enhanced central processing of painful stimuli is manifested by: Hyperalgesia (increased response to painful stimuli) and
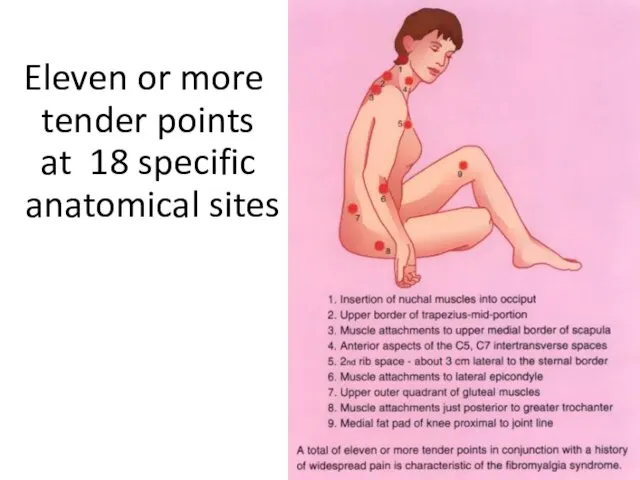
- 83. Eleven or more tender points at 18 specific anatomical sites
- 84. The Etiology of fibromyalgia remains unclear, Current hypotheses: Aberrant CNS processing of pain Dysfunction of the
- 85. Triggers of Fibromyalgia Physical trauma (car accidents) Infections such as hepatitis C, Epstein-Barr virus, parvovirus, or
- 86. Aggravating factors were: Emotional distress Weather changes Exertion
- 87. Healthy individuals with normal sleep and exercise patterns when deprived from Sleep and exercise Suffered from
- 88. Why should we know it better? It is the second most common diagnosis made in rheumatology
- 89. Why should we know it better? It is associated with substantial morbidity and disability It may
- 90. Why should we know it better? Co-existing fibromyalgia may be confused with a flare of SLE
- 91. It has to be differentiated from other serious causes of myalgia Polymylgia rheumatica Statins therapy Hypothyroidism
- 92. Optimal treatment of FMS mandates a multidisciplinary approach, including .Pharmacologic and Non- Pharmacologic interventions
- 93. Treatments should be specifically tailored to Patient reports of : Pain intensity Function Associated features such
- 94. Pharmacologic treatment: Strong evidence for Antidepressants: Dual re-uptake inhibitors TCA (amitryptiline, cyclobenzaprine) SNRIs ( milnacipram, duloxetine)
- 95. Non-Pharmacological therapies Strong evidence Education Aerobic exercises Cognitive behavioral therapies
- 96. Educational Points The patient must be reassured that fibromyalgia is a real illness, and not imagined
- 97. Aerobic Exercises General guidelines: Begin 2–3 months after start of drug therapy Begin with low impact
- 98. Take away message Patient Education Aerobic exercises Heated pool treatment Cognitive behavioral therapies Complement drug therapy.
- 103. Скачать презентацию
Слайд 3Amputations,
orthopedic injuries
arthritis
cardiac disease, cancer
neurological problems,
spinal cord injuries,
Amputations,
orthopedic injuries
arthritis
cardiac disease, cancer
neurological problems,
spinal cord injuries,
Слайд 4GOALS
Minimize functional deficits
Use remaining function to maximum
Prevent complications
Minimize functional deficits
Prevent complications
GOALS
Minimize functional deficits
Use remaining function to maximum
Prevent complications
Minimize functional deficits
Prevent complications

Слайд 5The key to Good
Rehabilitation
The key to Good
Rehabilitation
Слайд 6Physician specialists head Rehabilitation teams including a
The physical therapist.
occupational therapist.
The social workers.
Rehabilitation
Physician specialists head Rehabilitation teams including a
The physical therapist.
occupational therapist.
The social workers.
Rehabilitation
Слайд 7The physical therapist
*The physical therapist assists the patient in functional restoration.
*Tasks may
The physical therapist
*The physical therapist assists the patient in functional restoration.
*Tasks may

Слайд 8OCCUPATIONAL THERAPISTS Are responsible for those therapeutic activities associated with patient’s daily
OCCUPATIONAL THERAPISTS Are responsible for those therapeutic activities associated with patient’s daily

Слайд 10Occupational therapy
helps the patient regain the ability to do normal everyday tasks.
Occupational therapy
helps the patient regain the ability to do normal everyday tasks.
Слайд 11Speech therapy
helps the patient
correct speech disorders or restore speech.
Speech therapy
Speech therapy
helps the patient
correct speech disorders or restore speech.
Speech therapy
Слайд 12Key terms
Orthotist — A health care professional who is skilled
in making
Key terms
Orthotist — A health care professional who is skilled
in making
Слайд 13social worker
A social worker help to Communicate
the patient and family with
social worker
A social worker help to Communicate
the patient and family with
Слайд 14 Evaluation of the patient’s
total Living Situation,
Including
Lifestyle,
Family Finances,
Evaluation of the patient’s
total Living Situation,
Including
Lifestyle,
Family Finances,
Слайд 15Therapeutic Recreation
Therapeutic Recreation implements various interventions as a form of treatment
to
Therapeutic Recreation
Therapeutic Recreation implements various interventions as a form of treatment
to
Слайд 16The Vocational rehabilitation program will assist in training and placing disabled persons
The Vocational rehabilitation program will assist in training and placing disabled persons
Слайд 17What diagnostic tools are used in physiatry
medical history, physical examinations,
X-rays.
.Electromyography
What diagnostic tools are used in physiatry
medical history, physical examinations,
X-rays.
.Electromyography
Слайд 18 Physiatrists utilize
Medications
Injections.
Physical modalities.
Exercise.
Education individualized to the patient`s needs.
Assistive Devices
Physiatrists utilize
Medications
Injections.
Physical modalities.
Exercise.
Education individualized to the patient`s needs.
Assistive Devices
Слайд 19What Are Assistive الاجهزه المساعده Devices?
Assistive devices can help a person function
What Are Assistive الاجهزه المساعده Devices?
Assistive devices can help a person function
Слайд 20Many devices are available to help with activities of daily living (ADLs).
Many devices are available to help with activities of daily living (ADLs).
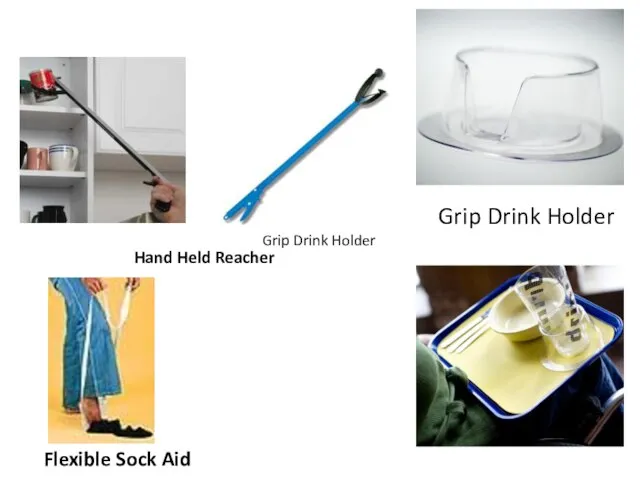
Слайд 21Hand Held Reacher
Flexible Sock Aid
Grip Drink Holder
Grip Drink Holder
Hand Held Reacher
Flexible Sock Aid
Grip Drink Holder
Grip Drink Holder
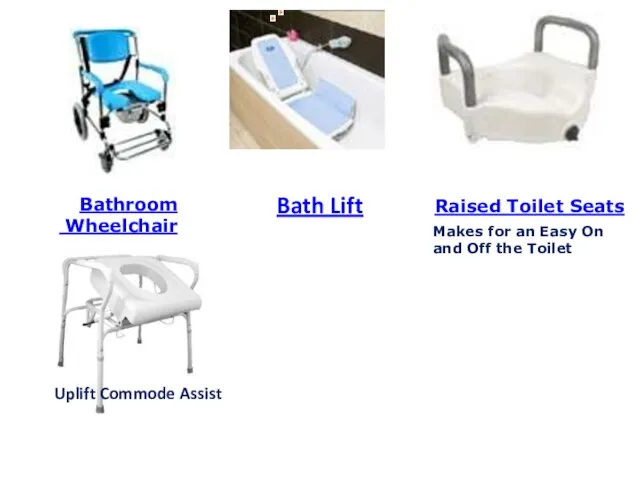
Слайд 22Bath Lift
Bathroom
Wheelchair
Raised Toilet Seats
Makes for an Easy
Bath Lift
Bathroom
Wheelchair
Raised Toilet Seats
Makes for an Easy
Слайд 23What Are the Different Types of Mobility Aids?
Mobility aids help with walking
What Are the Different Types of Mobility Aids?
Mobility aids help with walking
Слайд 24
Pediatric
Walkers
Pediatric
Walkers


Слайд 26NECK PAIN
لواءاستاذ دكتور
محمد رضا محمد عوض
NECK PAIN
لواءاستاذ دكتور
محمد رضا محمد عوض

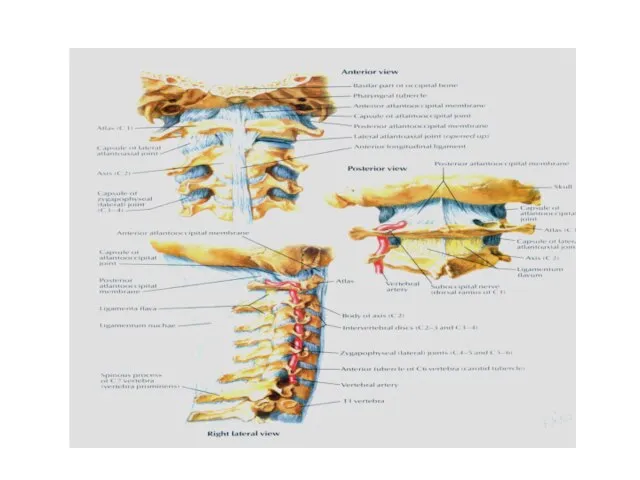
Слайд 31Anatomy
Head weighing 6:8 1b
7 cervical vertebrae
5 intervertebral discs
12 joints of Luschka
14 apophyseal
Anatomy
Head weighing 6:8 1b
7 cervical vertebrae
5 intervertebral discs
12 joints of Luschka
14 apophyseal
Слайд 32Prevalence
Neck Stiffness
25 : 30 % Age 25-29 year
Up to 50 % Age
Prevalence
Neck Stiffness
25 : 30 % Age 25-29 year
Up to 50 % Age
Слайд 33Musculosketetal Causes
Osteoarthritis
Diffuse idiopathic skeletal hyperstosis
Cervical spondylosis
Disk disease
Rheumatoid arthritis
Fracture
Neoplasm
Thoracic outlet syndrome (cervical rib,
Musculosketetal Causes
Osteoarthritis
Diffuse idiopathic skeletal hyperstosis
Cervical spondylosis
Disk disease
Rheumatoid arthritis
Fracture
Neoplasm
Thoracic outlet syndrome (cervical rib,
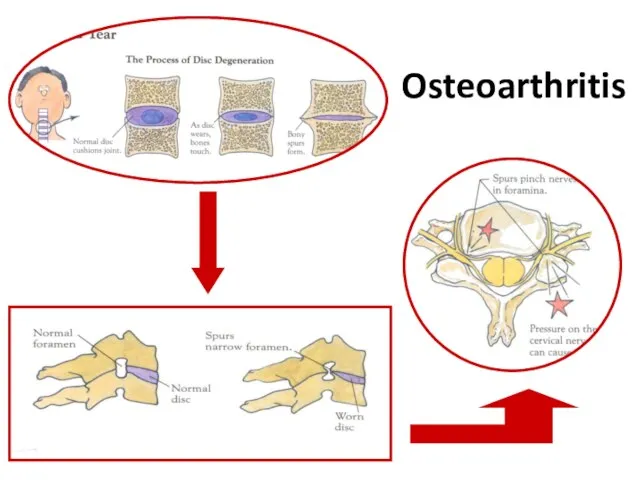
Слайд 34Osteoarthritis
Osteoarthritis
Слайд 35Neurological Causes
Nerve root syndromes
Cervical myelopathy
Neuritis (brachial,occipital)
Torticollis
Meningitis
Cord tumors
Neurological Causes
Nerve root syndromes
Cervical myelopathy
Neuritis (brachial,occipital)
Torticollis
Meningitis
Cord tumors
Слайд 36Soft tissue and muscular pain
Acute cervical strain
Cumulative trauma, overstrain syndromes
Tendinitis, bursitis
Postural disorders
Fibrositis,
Soft tissue and muscular pain
Acute cervical strain
Cumulative trauma, overstrain syndromes
Tendinitis, bursitis
Postural disorders
Fibrositis,
Слайд 37whiplash injury or neck sprain injury
The term “whiplash,” used to describe
whiplash injury or neck sprain injury
The term “whiplash,” used to describe
Слайд 38The most common
whiplash symptoms are
neck pain, neck stiffness, headache, shoulder pain, back
The most common
whiplash symptoms are
neck pain, neck stiffness, headache, shoulder pain, back
Слайд 39Referred Pain
Heart and coronary artery disease
Apex of lung: Pancoast’s tumor
Migraine
Muscle tension and
Referred Pain
Heart and coronary artery disease
Apex of lung: Pancoast’s tumor
Migraine
Muscle tension and
Слайд 40Clinical Evaluation
History
Physical Examination
Radiologic Evaluation
Electro - Diagnosis
(assist in confirming the clinical
Clinical Evaluation
History
Physical Examination
Radiologic Evaluation
Electro - Diagnosis
(assist in confirming the clinical
Слайд 41Examination of Related Area
Shoulder
(Rotator Cuff Tendenitis – capsulitis)
TMJ
Upper Limb
Examination of Related Area
Shoulder
(Rotator Cuff Tendenitis – capsulitis)
TMJ
Upper Limb
Слайд 47Management
Management

Слайд 48AIM
Relief of pain and stiffness in the neck and arms
Restore the
AIM
Relief of pain and stiffness in the neck and arms
Restore the
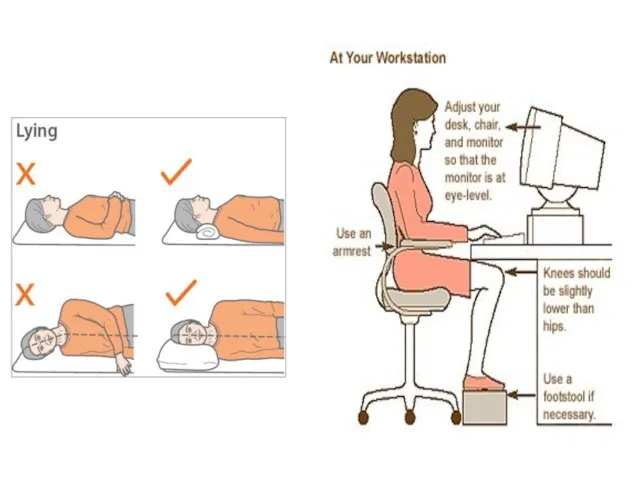
Слайд 49PATIENT EDUCATION
various types of initial neck pain treatment with
* analgesics, sedatives, antihistamines, nonsteroid
PATIENT EDUCATION
various types of initial neck pain treatment with
* analgesics, sedatives, antihistamines, nonsteroid


Слайд 53 LUMBAR DISC PROLAPSE
REDA AWAD
LUMBAR DISC PROLAPSE
REDA AWAD
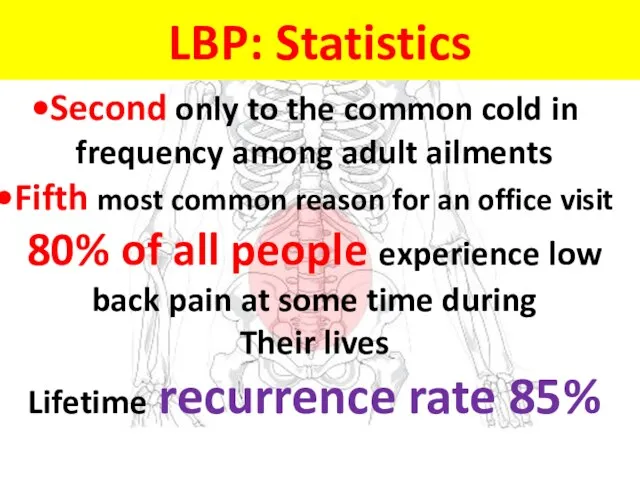
Слайд 54Second only to the common cold in frequency among adult ailments
Fifth most
Second only to the common cold in frequency among adult ailments
Fifth most
Слайд 55على المستوى المحلى
44 % من عمال الحديد والصلب
.
34 % من
على المستوى المحلى
44 % من عمال الحديد والصلب
.
34 % من

Слайд 56lumbar spine normal motion segment
lumbar spine normal motion segment
Слайд 57The disc is made up of three basic structures: the nucleus pulposus,
the annulus
The disc is made up of three basic structures: the nucleus pulposus,
the annulus
Слайд 58The disc is the
largest avascular structure
in the human body.
Nutrition
Nutrients
The disc is the
largest avascular structure
in the human body.
Nutrition
Nutrients
Слайд 59Disc innervation
1981 Australian clinical anatomist and physician
Nikoli Bogduk
The outer 1/3 of
Disc innervation
1981 Australian clinical anatomist and physician
Nikoli Bogduk
The outer 1/3 of
Слайд 60interadiscal pressure
interadiscal pressure
Слайд 61 is a synovial joint between the superior articular process, of one vertebra and the inferior articular process
is a synovial joint between the superior articular process, of one vertebra and the inferior articular process
Слайд 62Degeneration
Before age 40 approximately 25%. Beyond age 40, more than 60% of
Degeneration
Before age 40 approximately 25%. Beyond age 40, more than 60% of
Слайд 63As the disc dehydrates
the disc loose ability to support the axial
As the disc dehydrates
the disc loose ability to support the axial
Слайд 64Recommendation 1
Clinicians should conduct a focused
HISTORY&
PHYSICAL EXAMINATION
to help place patients with
Recommendation 1
Clinicians should conduct a focused
HISTORY&
PHYSICAL EXAMINATION
to help place patients with
Слайд 65or back pain potentially associated with another
Specific spinal causes 8%
Nonspecific low
or back pain potentially associated with another
Specific spinal causes 8%
Nonspecific low
Слайд 66Non-specific low back pain
Pain, muscle tension, or stiffness that occurs between
Non-specific low back pain
Pain, muscle tension, or stiffness that occurs between
Слайд 67specific disorder,( 8%)
such as
cancer
compression fracture
spinal infection
Ankylosing sp
specific disorder,( 8%)
such as
cancer
compression fracture
spinal infection
Ankylosing sp
Слайд 68
symptomatic
herniated disc 4%
Spinal stenosis 3%
cauda equina synd. 0.04%
is
symptomatic
herniated disc 4%
Spinal stenosis 3%
cauda equina synd. 0.04%
is
Слайд 69Symptoms of Facet Joint Problems
a persisting point of tenderness overlying the inflamed
Symptoms of Facet Joint Problems
a persisting point of tenderness overlying the inflamed
Слайд 70History
Physical Examination
Radiologic Evaluation
Electro - Diagnosis
(assist in confirming the clinical formulation)
Clinical
History
Physical Examination
Radiologic Evaluation
Electro - Diagnosis
(assist in confirming the clinical formulation)
Clinical
Слайд 74The Diagnosis of back pain should be
Based on a Good History
The Diagnosis of back pain should be
Based on a Good History
Слайд 75Imaging studies should be ordered in patient with :
- progressive neurologic deficits
-
- progressive neurologic deficits
-
Слайд 76Goals
*Relieve of pain
*Restoration
of physiological movements
*Prevention of relapses
Goals
*Relieve of pain
*Restoration
of physiological movements
*Prevention of relapses

Слайд 77 Surgery should be considered for
* Individuals With Motor Weakness
Surgery should be considered for
* Individuals With Motor Weakness
Слайд 78TH
لواء ا.د محمد رضا عوض
Fibromyalgia Syndrome
TH
لواء ا.د محمد رضا عوض
Fibromyalgia Syndrome
Слайд 79Typically presents with symptoms of diffuse body pain frequently involving the spinal
Typically presents with symptoms of diffuse body pain frequently involving the spinal
Слайд 80Fibromyalgia is associated with :
Fatigue
Sleep disorder
Anxiety , Depression
Cognitive disturbance(
Fibromyalgia is associated with :
Fatigue
Sleep disorder
Anxiety , Depression
Cognitive disturbance(
Слайд 81ACR 1990 Criteria for Fibromyalgia
Widespread pain with a minimum duration of 3
ACR 1990 Criteria for Fibromyalgia
Widespread pain with a minimum duration of 3
Слайд 82Enhanced central processing of painful stimuli is manifested by:
Hyperalgesia (increased response to
Enhanced central processing of painful stimuli is manifested by:
Hyperalgesia (increased response to
Слайд 83Eleven or more
tender points
at 18 specific
anatomical sites
Eleven or more
tender points
at 18 specific
anatomical sites
Слайд 84The Etiology of fibromyalgia remains unclear, Current hypotheses:
Aberrant CNS processing of pain
Dysfunction
The Etiology of fibromyalgia remains unclear, Current hypotheses:
Aberrant CNS processing of pain
Dysfunction
Слайд 85Triggers of Fibromyalgia
Physical trauma (car accidents)
Infections such as hepatitis C,
Triggers of Fibromyalgia
Physical trauma (car accidents)
Infections such as hepatitis C,
Слайд 86Aggravating factors were:
Emotional distress
Weather changes
Exertion
Aggravating factors were:
Emotional distress
Weather changes
Exertion
Слайд 87Healthy individuals with normal sleep and exercise patterns when deprived from Sleep
Healthy individuals with normal sleep and exercise patterns when deprived from Sleep
Слайд 88Why should we know it better?
It is the second most common diagnosis
Why should we know it better?
It is the second most common diagnosis
Слайд 89 Why should we know it better?
It is associated with substantial
Why should we know it better?
It is associated with substantial
Слайд 90Why should we know it better?
Co-existing fibromyalgia may be confused with a
Why should we know it better?
Co-existing fibromyalgia may be confused with a
Слайд 91It has to be differentiated from other serious causes of myalgia
Polymylgia rheumatica
It has to be differentiated from other serious causes of myalgia
Polymylgia rheumatica
Слайд 92Optimal treatment of FMS mandates a multidisciplinary approach, including
.Pharmacologic and
Non- Pharmacologic interventions
Optimal treatment of FMS mandates a multidisciplinary approach, including
.Pharmacologic and
Non- Pharmacologic interventions
Слайд 93Treatments should be specifically tailored to Patient reports of :
Pain intensity
Treatments should be specifically tailored to Patient reports of :
Pain intensity
Слайд 94Pharmacologic treatment:
Strong evidence for
Antidepressants:
Dual re-uptake inhibitors
TCA (amitryptiline, cyclobenzaprine)
SNRIs ( milnacipram, duloxetine)
Anticonvulsants
Pharmacologic treatment:
Strong evidence for
Antidepressants:
Dual re-uptake inhibitors
TCA (amitryptiline, cyclobenzaprine)
SNRIs ( milnacipram, duloxetine)
Anticonvulsants
Слайд 95Non-Pharmacological therapies
Strong evidence
Education
Aerobic exercises
Cognitive behavioral therapies
Non-Pharmacological therapies
Strong evidence
Education
Aerobic exercises
Cognitive behavioral therapies
Слайд 96 Educational Points
The patient must be reassured that fibromyalgia is a real
Educational Points
The patient must be reassured that fibromyalgia is a real
Слайд 97
Aerobic Exercises
General guidelines:
Begin 2–3 months after start of drug therapy
Begin with
Aerobic Exercises
General guidelines:
Begin 2–3 months after start of drug therapy
Begin with
Слайд 98Take away message
Patient Education
Aerobic exercises
Heated pool treatment
Cognitive behavioral therapies
Take away message
Patient Education
Aerobic exercises
Heated pool treatment
Cognitive behavioral therapies



 Аутосомно-доминантное наследование
Аутосомно-доминантное наследование Метеоризм. Профилактика метеоризма
Метеоризм. Профилактика метеоризма Раны, кровотечения. Правила первой помощи
Раны, кровотечения. Правила первой помощи Правила наложения повязок при кровотечениях
Правила наложения повязок при кровотечениях Диагностика инфекционных стоматитов у стоматологических больных
Диагностика инфекционных стоматитов у стоматологических больных группа крови
группа крови Лекарственные растения
Лекарственные растения Пролапс железы третьего века
Пролапс железы третьего века Гинекологическая и акушерская патология
Гинекологическая и акушерская патология Вторичный и третичный периоды сифилиса. 1 часть. Лекция 7
Вторичный и третичный периоды сифилиса. 1 часть. Лекция 7 Психотропные средства
Психотропные средства IV Международный студенческий турнир медиков 2018 года. Региональный этап. Финальные бои. Команда “Во весь спектр”
IV Международный студенческий турнир медиков 2018 года. Региональный этап. Финальные бои. Команда “Во весь спектр” Самопомощь при сердечном приступе
Самопомощь при сердечном приступе Клиническая фармация
Клиническая фармация Особенности клинического течения, диагностика и терапия аллергического риносинуита, сочетанного с бронхиальной астмой
Особенности клинического течения, диагностика и терапия аллергического риносинуита, сочетанного с бронхиальной астмой Кишечный иерсиниоз
Кишечный иерсиниоз Развитие равновесия у обучающихся младшего школьного возраста с нарушением слуха на занятиях гимнастикой
Развитие равновесия у обучающихся младшего школьного возраста с нарушением слуха на занятиях гимнастикой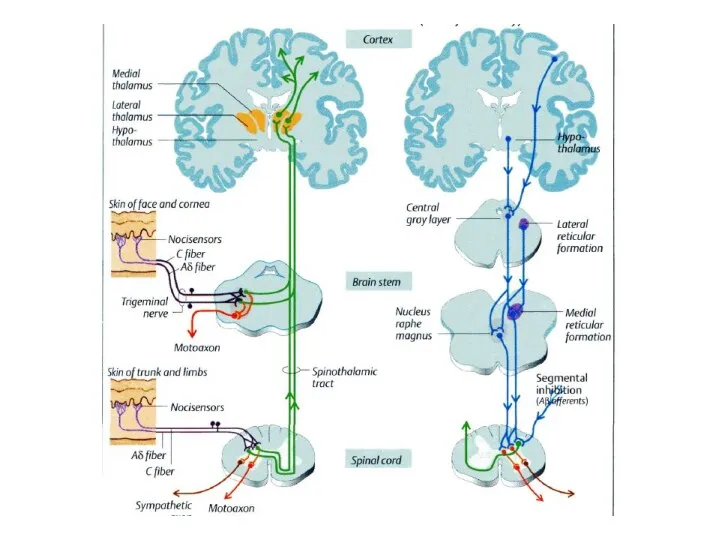 Боль. Локализация боли
Боль. Локализация боли Кератотопография роговицы (топография роговицы)
Кератотопография роговицы (топография роговицы) Здоровье детей в наших руках
Здоровье детей в наших руках Гемофилия. Проклятие королевы Виктории. История на биологии
Гемофилия. Проклятие королевы Виктории. История на биологии Принципы лечения инфекционных заболеваний
Принципы лечения инфекционных заболеваний Заболевания щитовидной железы
Заболевания щитовидной железы Бредовые психозы позднего возраста
Бредовые психозы позднего возраста Правила личной гигиены и здоровье
Правила личной гигиены и здоровье Паратиф А. Особенности возбудителя
Паратиф А. Особенности возбудителя Симпатомиметики. Эфедрин
Симпатомиметики. Эфедрин Лечебная физическая культура при повреждениях нижних конечностей
Лечебная физическая культура при повреждениях нижних конечностей