- Polycystic Ovary Syndrome (PCOS)

Содержание
- 2. Objectives Describe PCOS and associated pathophysiology Identify risk factors of and conditions related to PCOS Diagnose
- 3. Polycystic Ovary SYNDROME 1800s: polycystic ovaries “cystic oophoritis”; “sclerocystic” Stein & Leventhal (1953) Enlarged ovaries, hirsutism,
- 4. PCOS PCOS Collection of signs and symptoms May be difficult to diagnose Heterogeneous presentation Features change
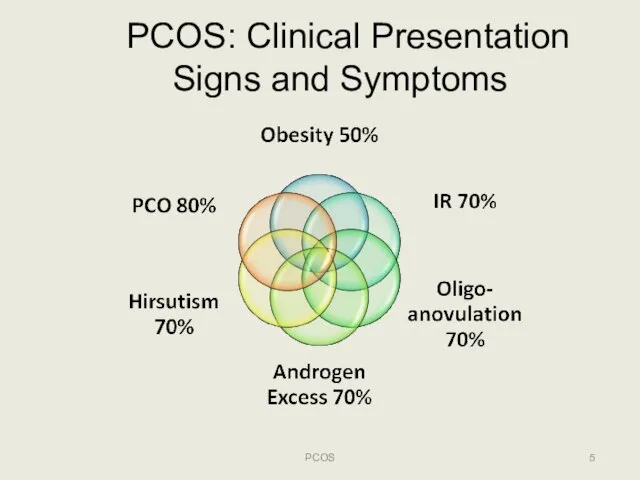
- 5. PCOS: Clinical Presentation Signs and Symptoms PCOS
- 6. Epidemiology PCOS Most common endocrine abnormality in reproductive aged women 5‐15% women affected – with ethnic
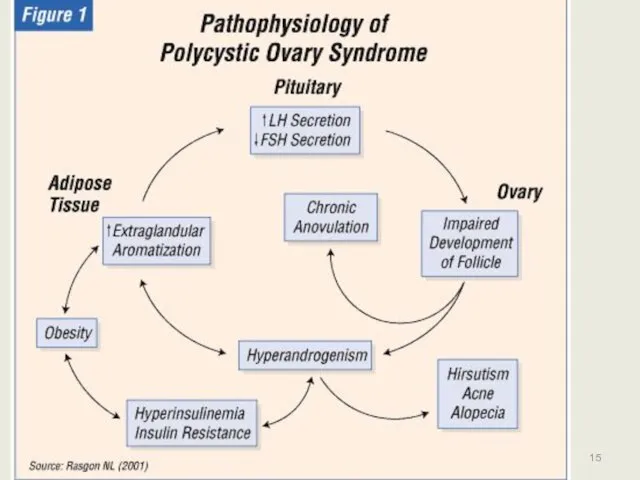
- 7. Polycystic Ovary Syndrome (PCOS) ETIOLOGY & PATHOPHYSIOLOGY PCOS
- 8. PCOS: Etiology PCOS Neuroendocrine derangement: ↑LH relative to FSH Hyperinsulinemia: defect in insulin action or secretion
- 9. Normal Menstrual Cycle PCOS LH FSH PCOS Cycle day Cycle day
- 10. Effects of Hyperinsulinemia Decrease binding proteins (ie., SHBG, IGFBP‐I) Increase unbound androgens Reduce HDL [good] cholesterol
- 11. PCOS: Androgen Excess Worse with hyperinsulinemia Hirsutism: 80% PCOS Acne: 20% PCOS Androgenic alopecia: 10% PCOS
- 12. PCOS Etiology: Unifying theory? PCOS
- 13. PCOS: Phenotypic & Genetic Variation Susceptibility Genes Modifier Genes Environment PCOS
- 14. 14 PCOS Adapted from Luque-Ramirez et al, Clinica Chimica Acta, 2006.
- 15. PCOS 15
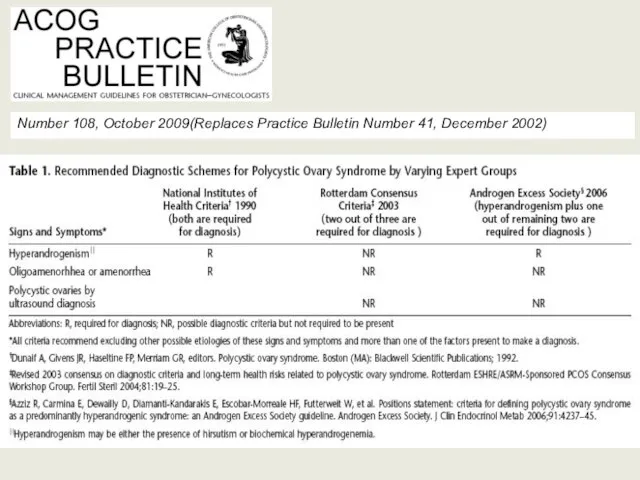
- 16. PCOS: Diagnostic Criteria PCOS NIH/NICHD: USA, 1990 ESHRE/ASRM: Rotterdam, 2004 Androgen Excess‐PCOS Intl Society: 2006
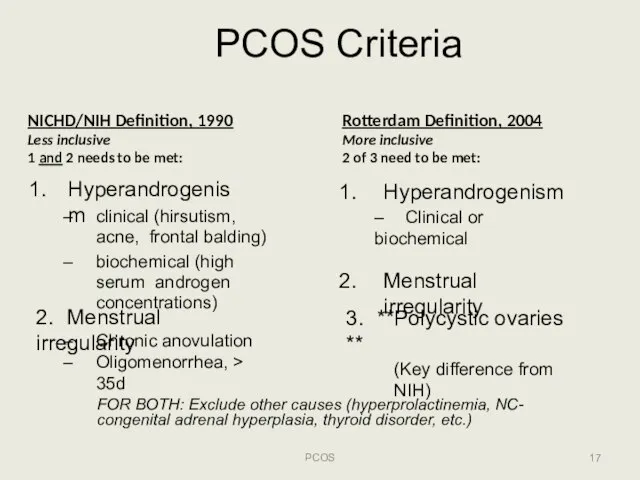
- 17. PCOS Criteria PCOS NICHD/NIH Definition, 1990 Less inclusive 1 and 2 needs to be met: Hyperandrogenism
- 18. AE‐PCOS Society, 2006 PCOS Hyperandrogenism**: Hirsutism and/or hyperandrogenemia AND Ovarian Dysfunction: Oligo‐anovulation and/or polycystic ovaries Exclusion
- 19. Number 108, October 2009(Replaces Practice Bulletin Number 41, December 2002)
- 20. Polycystic Ovary Syndrome (PCOS) EVALUATION PCOS
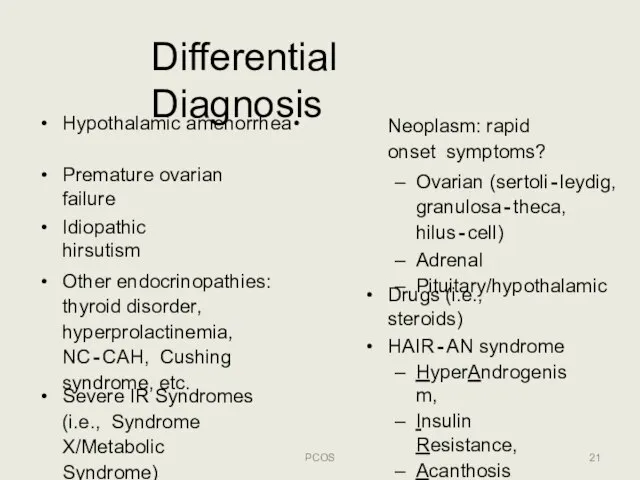
- 21. Differential Diagnosis PCOS Premature ovarian failure Idiopathic hirsutism Other endocrinopathies: thyroid disorder, hyperprolactinemia, NC‐CAH, Cushing syndrome,
- 22. PCOS: Menstrual Dysfunction PCOS 25‐30% of women with oligo‐anovulation have PCOS ≥35 day intervals or 2/3
- 23. Polycystic ovaries ≠ PCO syndrome Transvaginal sono is best Incidence decreases with age Sonogram Morphology: >12
- 24. Assessing Hirsutism Hirsutism vs virilization: rapidly developing virilization or certain virilizing symptoms (i.e., clitoromegaly, voice deepening)
- 25. PCOS: Physical Exam PCOS Blood pressure Body mass index (kg/m2) >25 overweight >30 obese Waist circumference
- 26. PCOS: Basic Work‐up PCOS FSH & estradiol (E2) +/‐ LH: premature ovarian failure (low E2; high
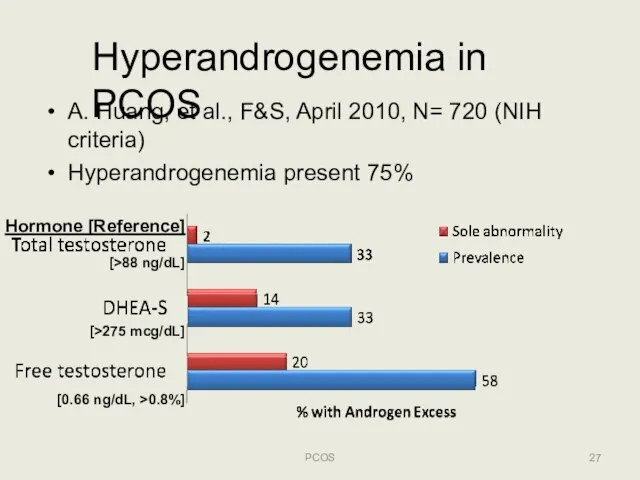
- 27. Hyperandrogenemia in PCOS A. Huang, et al., F&S, April 2010, N= 720 (NIH criteria) Hyperandrogenemia present
- 28. PCOS: Evaluation PCOS DHEA‐S Mildly elevated in 30‐40% PCOS adrenal tumors >700 mcg/dL € Pelvic/Adrenal contrast
- 29. PCOS: Optional Evaluation PCOS Total testosterone Ovarian tumors >200ng/dL € get imaging PCOS: upper limit of
- 30. PCOS: Obesity PCOS NOT part of diagnostic criteria Common in PCOS, affects between 50 to 80%
- 31. PCOS: Overweight? PCOS Screen impaired glucose tolerance or Diabetes oral GTT: Fasting glucose € drink 75
- 32. Metabolic Syndrome 15% of U.S. population 33% of PCOS!! Adult Treatment Panel III (others exist): Elevated
- 33. Polycystic Ovary Syndrome (PCOS) TREATMENT: GOAL SPECIFIC PCOS
- 34. PCOS: Goal Specific Therapy PCOS Screen and manage comorbidities Hirsutism/acne/hair loss Protect/monitor endometrium Ultrasound +/‐ endometrial
- 35. PCOS: Co‐morbidities! PCOS Insulin resistance, ~30% Type‐II DM, ~10% (3‐5x) Gestational diabetes (2.5x) Endometrial hyperplasia/ atypia/cancer
- 36. PCOS: Probable Links PCOS Coronary artery disease Dyslipidemia Hypertension Ovarian cancer (?) Miscarriage (?) Pregnancy induced
- 37. Prevention of CVD and DM PCOS Lifestyle: weightloss and exercise!! Metformin 1500‐2000 mg daily if documented
- 38. PCOS: Endometrial CA PCOS 56 obese PCOS women (Cheung,2001) 36% hyperplasia € 2% cancer without tx
- 39. Summary: Sequelae of biochemical aberrations PCOS
- 40. Treatment of Hirsutism PCOS Multi‐step approach is most‐effective: Hair removal: wax, laser, eflornithine, etc. OCPs for
- 41. Treating PCOS anovulatory infertility PCOS
- 42. PCOS: Weight Loss PCOS Frequency of obesity in women with anovulation and PCO: 30%‐75% ‐‐ most
- 43. PCOS and Infertility: Metformin? PCOS Metformin (biguanide ): improves insulin resistance reduce hepatic glucose production &
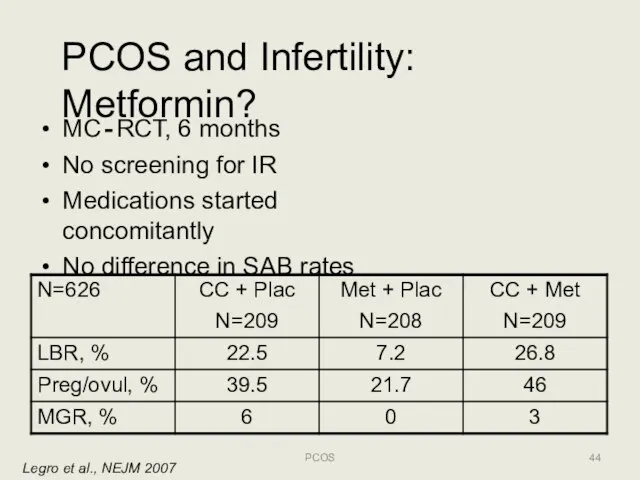
- 44. PCOS and Infertility: Metformin? Legro et al., NEJM 2007 MC‐RCT, 6 months No screening for IR
- 45. PCOS Fertility Options: Ovulation Induction (OI)/Superovulation (SO) Clomiphene Citrate: non‐steroidal weak estrogen related to diethystilbestrol, SERM
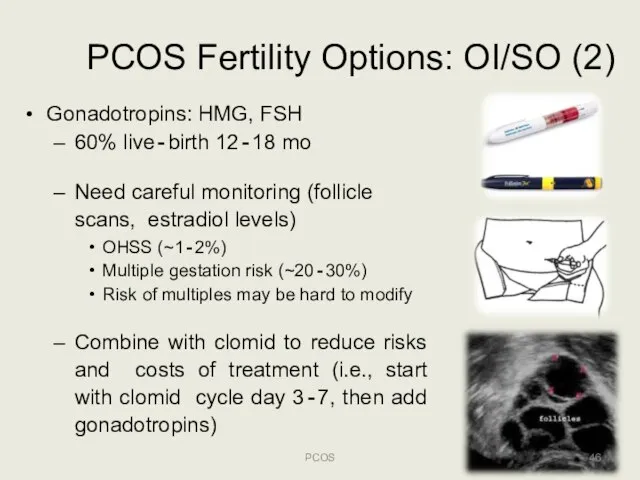
- 46. PCOS Fertility Options: OI/SO (2) Gonadotropins: HMG, FSH 60% live‐birth 12‐18 mo Need careful monitoring (follicle
- 47. PCOS Fertility Options: ART PCOS Assisted Reproductive Technologies (ie, IVF/ICSI) PROS Highly successful in PCOS: >60%
- 48. PCOS Fertility Options: Surgery PCOS Laparoscopic wedge resection or ovarian drilling PROS May avoid fertility treatment
- 49. PCOS: Pharmacotherapy summary PCOS
- 50. PCOS: Conclusions (1) PCOS Multifaceted condition with varying presentation No clearly accepted basis for diagnosis Significantly
- 52. Скачать презентацию
Слайд 2Objectives
Describe PCOS and associated pathophysiology
Identify risk factors of and conditions related to
Objectives
Describe PCOS and associated pathophysiology
Identify risk factors of and conditions related to
Слайд 3Polycystic Ovary SYNDROME
1800s: polycystic ovaries
“cystic oophoritis”; “sclerocystic”
Stein & Leventhal (1953)
Enlarged ovaries, hirsutism,
Polycystic Ovary SYNDROME
1800s: polycystic ovaries
“cystic oophoritis”; “sclerocystic”
Stein & Leventhal (1953)
Enlarged ovaries, hirsutism,
Слайд 4PCOS
PCOS
Collection of signs and symptoms
May be difficult to diagnose
Heterogeneous presentation
Features change with
PCOS
PCOS
Collection of signs and symptoms
May be difficult to diagnose
Heterogeneous presentation
Features change with
Слайд 5PCOS: Clinical Presentation Signs and Symptoms
PCOS
PCOS: Clinical Presentation Signs and Symptoms
PCOS
Слайд 6Epidemiology
PCOS
Most common endocrine abnormality in reproductive aged women
5‐15% women affected – with
Epidemiology
PCOS
Most common endocrine abnormality in reproductive aged women
5‐15% women affected – with
Слайд 7Polycystic Ovary Syndrome (PCOS)
ETIOLOGY & PATHOPHYSIOLOGY
PCOS
Polycystic Ovary Syndrome (PCOS)
ETIOLOGY & PATHOPHYSIOLOGY
PCOS
Слайд 8PCOS: Etiology
PCOS
Neuroendocrine derangement: ↑LH relative to FSH
Hyperinsulinemia: defect in insulin action or
PCOS: Etiology
PCOS
Neuroendocrine derangement: ↑LH relative to FSH
Hyperinsulinemia: defect in insulin action or
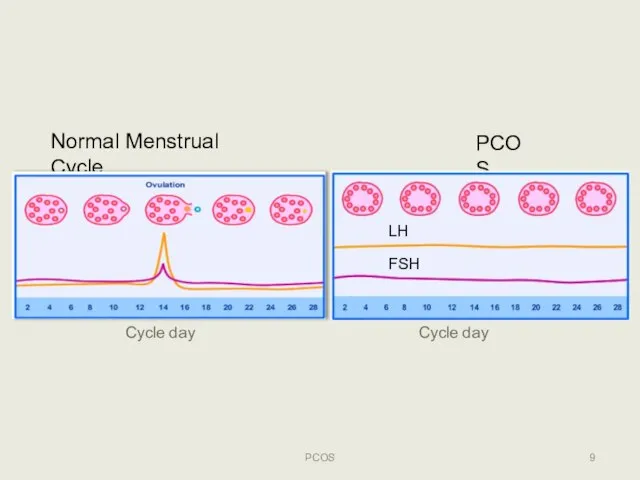
Слайд 9Normal Menstrual Cycle
PCOS
LH
FSH
PCOS
Cycle day
Cycle day
Normal Menstrual Cycle
PCOS
LH
FSH
PCOS
Cycle day
Cycle day
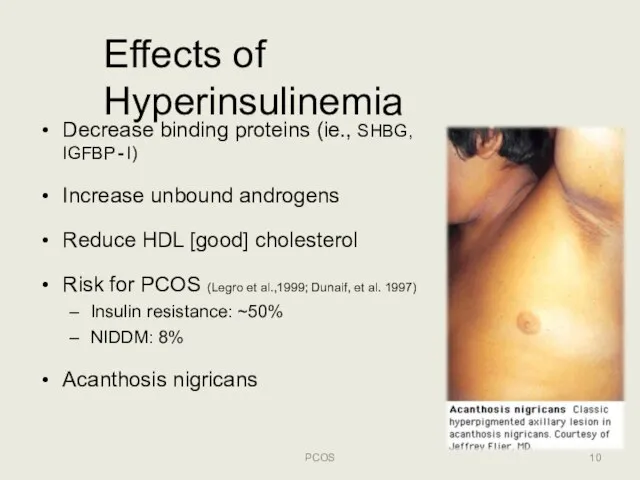
Слайд 10Effects of Hyperinsulinemia
Decrease binding proteins (ie., SHBG, IGFBP‐I)
Increase unbound androgens
Reduce HDL [good]
Effects of Hyperinsulinemia
Decrease binding proteins (ie., SHBG, IGFBP‐I)
Increase unbound androgens
Reduce HDL [good]
Слайд 11PCOS: Androgen Excess
Worse with hyperinsulinemia
Hirsutism: 80% PCOS
Acne: 20% PCOS
Androgenic alopecia: 10% PCOS
PCOS
PCOS: Androgen Excess
Worse with hyperinsulinemia
Hirsutism: 80% PCOS
Acne: 20% PCOS
Androgenic alopecia: 10% PCOS
PCOS

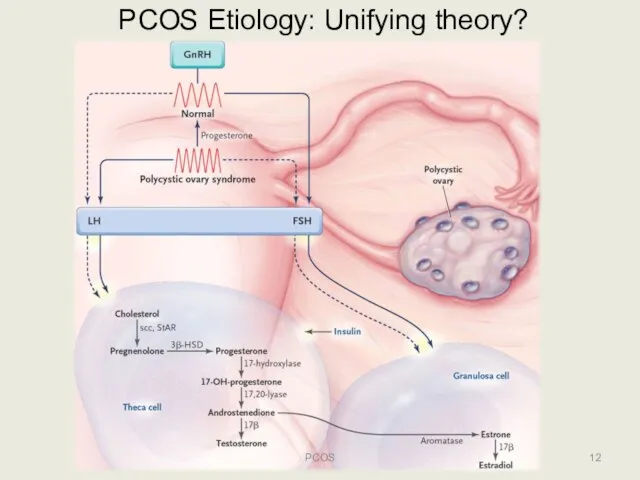
Слайд 12PCOS Etiology: Unifying theory?
PCOS
PCOS Etiology: Unifying theory?
PCOS
Слайд 13PCOS: Phenotypic & Genetic Variation
Susceptibility Genes
Modifier Genes
Environment
PCOS
PCOS: Phenotypic & Genetic Variation
Susceptibility Genes
Modifier Genes
Environment
PCOS
Слайд 1414
PCOS
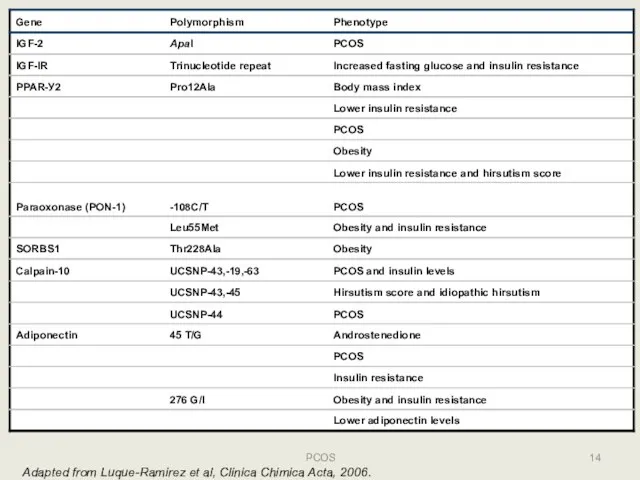
Adapted from Luque-Ramirez et al, Clinica Chimica Acta, 2006.
14
PCOS
Adapted from Luque-Ramirez et al, Clinica Chimica Acta, 2006.
Слайд 15PCOS
15
PCOS
15
Слайд 16PCOS: Diagnostic Criteria
PCOS
NIH/NICHD: USA, 1990
ESHRE/ASRM: Rotterdam, 2004
Androgen Excess‐PCOS Intl Society: 2006
PCOS: Diagnostic Criteria
PCOS
NIH/NICHD: USA, 1990
ESHRE/ASRM: Rotterdam, 2004
Androgen Excess‐PCOS Intl Society: 2006
Слайд 17PCOS Criteria
PCOS
NICHD/NIH Definition, 1990
Less inclusive
1 and 2 needs to be met:
Hyperandrogenism
clinical (hirsutism,
PCOS Criteria
PCOS
NICHD/NIH Definition, 1990
Less inclusive
1 and 2 needs to be met:
Hyperandrogenism
clinical (hirsutism,
Слайд 18AE‐PCOS Society, 2006
PCOS
Hyperandrogenism**: Hirsutism and/or hyperandrogenemia
AND
Ovarian Dysfunction: Oligo‐anovulation and/or polycystic ovaries
Exclusion of
AE‐PCOS Society, 2006
PCOS
Hyperandrogenism**: Hirsutism and/or hyperandrogenemia
AND
Ovarian Dysfunction: Oligo‐anovulation and/or polycystic ovaries
Exclusion of
Слайд 19Number 108, October 2009(Replaces Practice Bulletin Number 41, December 2002)
Number 108, October 2009(Replaces Practice Bulletin Number 41, December 2002)
Слайд 20Polycystic Ovary Syndrome (PCOS)
EVALUATION
PCOS
Polycystic Ovary Syndrome (PCOS)
EVALUATION
PCOS
Слайд 21Differential Diagnosis
PCOS
Premature ovarian failure
Idiopathic hirsutism
Other endocrinopathies: thyroid disorder, hyperprolactinemia, NC‐CAH, Cushing syndrome,
Differential Diagnosis
PCOS
Premature ovarian failure
Idiopathic hirsutism
Other endocrinopathies: thyroid disorder, hyperprolactinemia, NC‐CAH, Cushing syndrome,
Слайд 22PCOS: Menstrual Dysfunction
PCOS
25‐30% of women with oligo‐anovulation have PCOS
≥35 day intervals or
PCOS: Menstrual Dysfunction
PCOS
25‐30% of women with oligo‐anovulation have PCOS
≥35 day intervals or
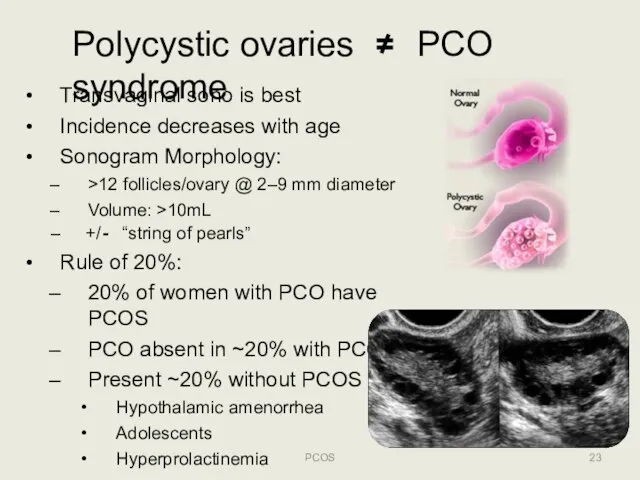
Слайд 23Polycystic ovaries ≠ PCO syndrome
Transvaginal sono is best
Incidence decreases with age
Sonogram Morphology:
>12
Polycystic ovaries ≠ PCO syndrome
Transvaginal sono is best
Incidence decreases with age
Sonogram Morphology:
>12
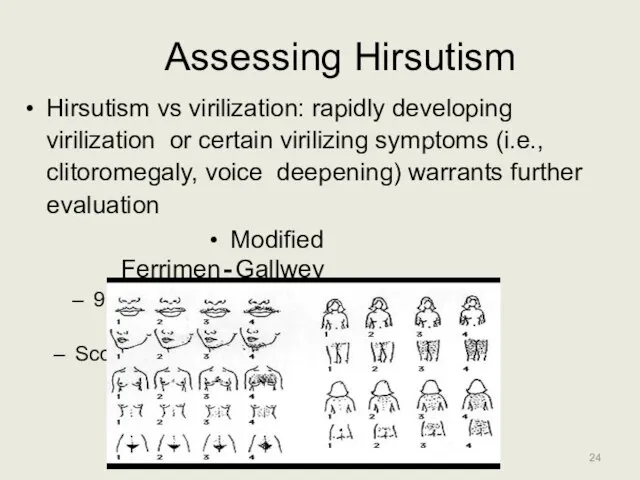
Слайд 24Assessing Hirsutism
Hirsutism vs virilization: rapidly developing virilization or certain virilizing symptoms (i.e.,
Assessing Hirsutism
Hirsutism vs virilization: rapidly developing virilization or certain virilizing symptoms (i.e.,
Слайд 25PCOS: Physical Exam
PCOS
Blood pressure
Body mass index (kg/m2)
>25 overweight
>30 obese
Waist circumference > 35
PCOS: Physical Exam
PCOS
Blood pressure
Body mass index (kg/m2)
>25 overweight
>30 obese
Waist circumference > 35
Слайд 26PCOS: Basic Work‐up
PCOS
FSH & estradiol (E2) +/‐ LH:
premature ovarian failure (low E2;
PCOS: Basic Work‐up
PCOS
FSH & estradiol (E2) +/‐ LH:
premature ovarian failure (low E2;
Слайд 27Hyperandrogenemia in PCOS
A. Huang, et al., F&S, April 2010, N= 720 (NIH
Hyperandrogenemia in PCOS
A. Huang, et al., F&S, April 2010, N= 720 (NIH
Слайд 28PCOS: Evaluation
PCOS
DHEA‐S
Mildly elevated in 30‐40% PCOS
adrenal tumors >700 mcg/dL € Pelvic/Adrenal contrast
PCOS: Evaluation
PCOS
DHEA‐S
Mildly elevated in 30‐40% PCOS
adrenal tumors >700 mcg/dL € Pelvic/Adrenal contrast
Слайд 29PCOS: Optional Evaluation
PCOS
Total testosterone
Ovarian tumors >200ng/dL € get imaging
PCOS: upper limit of
PCOS: Optional Evaluation
PCOS
Total testosterone
Ovarian tumors >200ng/dL € get imaging
PCOS: upper limit of
Слайд 30PCOS: Obesity
PCOS
NOT part of diagnostic criteria
Common in PCOS, affects between 50 to
PCOS: Obesity
PCOS
NOT part of diagnostic criteria
Common in PCOS, affects between 50 to
Слайд 31PCOS: Overweight?
PCOS
Screen impaired glucose tolerance or Diabetes
oral GTT: Fasting glucose € drink
PCOS: Overweight?
PCOS
Screen impaired glucose tolerance or Diabetes
oral GTT: Fasting glucose € drink
Слайд 32Metabolic Syndrome
15% of U.S. population
33% of PCOS!!
Adult Treatment Panel III (others exist):
Elevated
Metabolic Syndrome
15% of U.S. population
33% of PCOS!!
Adult Treatment Panel III (others exist):
Elevated
Слайд 33Polycystic Ovary Syndrome (PCOS)
TREATMENT: GOAL SPECIFIC
PCOS
Polycystic Ovary Syndrome (PCOS)
TREATMENT: GOAL SPECIFIC
PCOS
Слайд 34PCOS: Goal Specific Therapy
PCOS
Screen and manage comorbidities
Hirsutism/acne/hair loss
Protect/monitor endometrium
Ultrasound +/‐ endometrial sampling
HRT/OCP
PCOS: Goal Specific Therapy
PCOS
Screen and manage comorbidities
Hirsutism/acne/hair loss
Protect/monitor endometrium
Ultrasound +/‐ endometrial sampling
HRT/OCP
Слайд 35PCOS: Co‐morbidities!
PCOS
Insulin resistance, ~30%
Type‐II DM, ~10% (3‐5x)
Gestational diabetes (2.5x)
Endometrial hyperplasia/ atypia/cancer
Metabolic syndrome/syndrome X
Sleep
PCOS: Co‐morbidities!
PCOS
Insulin resistance, ~30%
Type‐II DM, ~10% (3‐5x)
Gestational diabetes (2.5x)
Endometrial hyperplasia/ atypia/cancer
Metabolic syndrome/syndrome X
Sleep
Слайд 36PCOS: Probable Links
PCOS
Coronary artery disease
Dyslipidemia
Hypertension
Ovarian cancer (?)
Miscarriage (?)
Pregnancy induced hypertension/PIH (?)
PCOS: Probable Links
PCOS
Coronary artery disease
Dyslipidemia
Hypertension
Ovarian cancer (?)
Miscarriage (?)
Pregnancy induced hypertension/PIH (?)
Слайд 37Prevention of CVD and DM
PCOS
Lifestyle: weightloss and exercise!!
Metformin 1500‐2000 mg daily if
Prevention of CVD and DM
PCOS
Lifestyle: weightloss and exercise!!
Metformin 1500‐2000 mg daily if
Слайд 38PCOS: Endometrial CA
PCOS
56 obese PCOS women (Cheung,2001)
36% hyperplasia € 2% cancer without
PCOS: Endometrial CA
PCOS
56 obese PCOS women (Cheung,2001)
36% hyperplasia € 2% cancer without
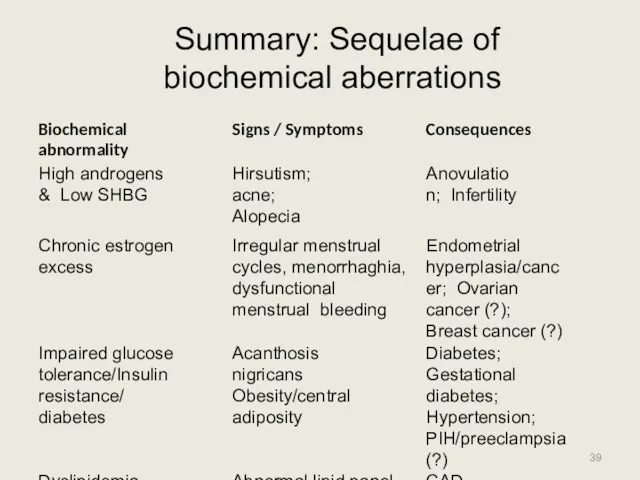
Слайд 39Summary: Sequelae of biochemical aberrations
PCOS
Summary: Sequelae of biochemical aberrations
PCOS
Слайд 40Treatment of Hirsutism
PCOS
Multi‐step approach is most‐effective:
Hair removal: wax, laser, eflornithine, etc.
OCPs for
Treatment of Hirsutism
PCOS
Multi‐step approach is most‐effective:
Hair removal: wax, laser, eflornithine, etc.
OCPs for

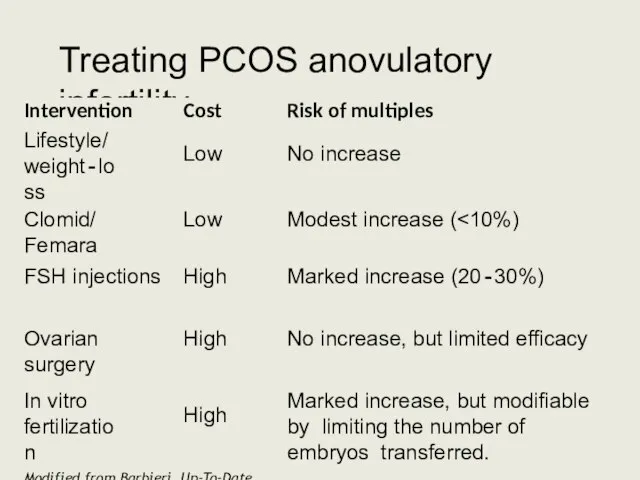
Слайд 41Treating PCOS anovulatory infertility
PCOS
Treating PCOS anovulatory infertility
PCOS
Слайд 42PCOS: Weight Loss
PCOS
Frequency of obesity in women with anovulation and PCO: 30%‐75%
PCOS: Weight Loss
PCOS
Frequency of obesity in women with anovulation and PCO: 30%‐75%
Слайд 43PCOS and Infertility: Metformin?
PCOS
Metformin (biguanide ): improves insulin resistance
reduce hepatic glucose production
PCOS and Infertility: Metformin?
PCOS
Metformin (biguanide ): improves insulin resistance
reduce hepatic glucose production
Слайд 44PCOS and Infertility: Metformin?
Legro et al., NEJM 2007
MC‐RCT, 6 months
No screening for
PCOS and Infertility: Metformin?
Legro et al., NEJM 2007
MC‐RCT, 6 months
No screening for
Слайд 45PCOS Fertility Options: Ovulation Induction (OI)/Superovulation (SO)
Clomiphene Citrate: non‐steroidal weak estrogen related
PCOS Fertility Options: Ovulation Induction (OI)/Superovulation (SO)
Clomiphene Citrate: non‐steroidal weak estrogen related
Слайд 46PCOS Fertility Options: OI/SO (2)
Gonadotropins: HMG, FSH
60% live‐birth 12‐18 mo
Need careful monitoring
PCOS Fertility Options: OI/SO (2)
Gonadotropins: HMG, FSH
60% live‐birth 12‐18 mo
Need careful monitoring
Слайд 47PCOS Fertility Options: ART
PCOS
Assisted Reproductive Technologies (ie, IVF/ICSI)
PROS
Highly successful in PCOS: >60%
PCOS Fertility Options: ART
PCOS
Assisted Reproductive Technologies (ie, IVF/ICSI)
PROS
Highly successful in PCOS: >60%
Слайд 48PCOS Fertility Options: Surgery
PCOS
Laparoscopic wedge resection or ovarian drilling
PROS
May avoid fertility treatment
PCOS Fertility Options: Surgery
PCOS
Laparoscopic wedge resection or ovarian drilling
PROS
May avoid fertility treatment
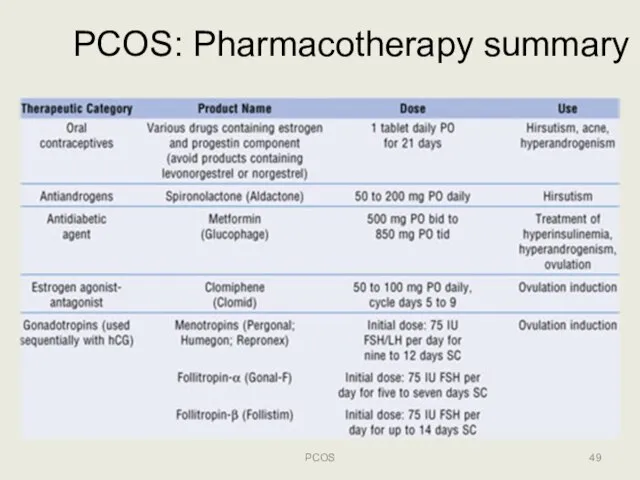
Слайд 49PCOS: Pharmacotherapy summary
PCOS
PCOS: Pharmacotherapy summary
PCOS
Слайд 50PCOS: Conclusions (1)
PCOS
Multifaceted condition with varying presentation
No clearly accepted basis for diagnosis
Significantly
PCOS: Conclusions (1)
PCOS
Multifaceted condition with varying presentation
No clearly accepted basis for diagnosis
Significantly
 Ревматоидный артрит
Ревматоидный артрит Капли для глаз Relins®
Капли для глаз Relins® Инфузионная терапия в педиатрии
Инфузионная терапия в педиатрии Диагностические критерии и тактика врача при кашле неврогенного характера
Диагностические критерии и тактика врача при кашле неврогенного характера Коронавирусная инфекция COVID-19
Коронавирусная инфекция COVID-19 Болезнь Паркинсона
Болезнь Паркинсона Антагонисты лейкотриеновых рецепторов
Антагонисты лейкотриеновых рецепторов Наркотики и их влияние на развитие полноценной личности
Наркотики и их влияние на развитие полноценной личности Акушерство. Анатомия внутренних женских половых органов
Акушерство. Анатомия внутренних женских половых органов Параметрит. Этиология
Параметрит. Этиология PSO_sterilizatsia (1)
PSO_sterilizatsia (1) Нома. Клиническая картина номы
Нома. Клиническая картина номы Тест по теме: Эндокринная система
Тест по теме: Эндокринная система Вирусология. Клиническая и экологическая микробиология. Вирусы иммунодефицита человека. (Модуль 3.25)
Вирусология. Клиническая и экологическая микробиология. Вирусы иммунодефицита человека. (Модуль 3.25) Медико-биологическая характеристика действия физических факторов окружающей и производственной среды на организм человека
Медико-биологическая характеристика действия физических факторов окружающей и производственной среды на организм человека Ожоги различной степени
Ожоги различной степени Құс тұмауы.Шошқа тұмауы
Құс тұмауы.Шошқа тұмауы Апоплексия яичника
Апоплексия яичника Жұмсақ тіндердің жарақаты
Жұмсақ тіндердің жарақаты Санитария и гигиена парикмахерских услуг: Кожные заболевания
Санитария и гигиена парикмахерских услуг: Кожные заболевания Острый и хронический миелолейкоз – сходства и различия
Острый и хронический миелолейкоз – сходства и различия Заболевания нервной системы, их предупреждение
Заболевания нервной системы, их предупреждение Ерте және жасырын түрдегі ауруларды
Ерте және жасырын түрдегі ауруларды Возможности скрининга заболеваний ЖКТ у учащихся школы и средних учебных заведений
Возможности скрининга заболеваний ЖКТ у учащихся школы и средних учебных заведений Мониторинг и аудит клинических исследований
Мониторинг и аудит клинических исследований Интерлейкины семейства интерлейкина-1
Интерлейкины семейства интерлейкина-1 Атеросклероз
Атеросклероз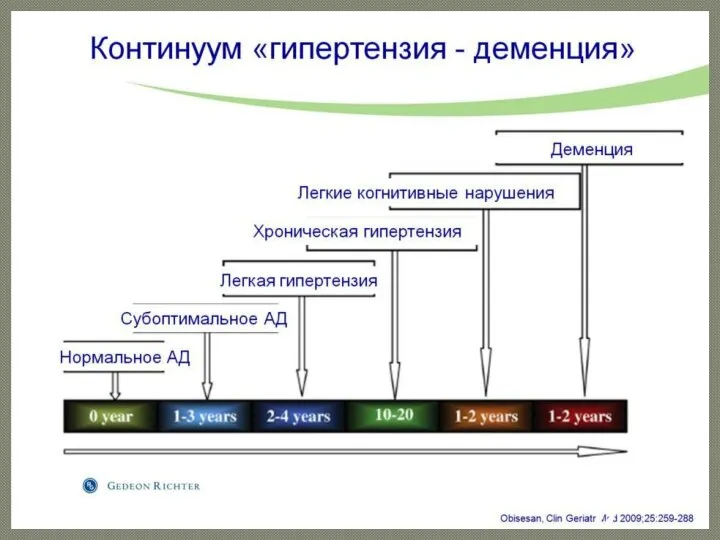 Влияние АГ на сосудистую систему мозга
Влияние АГ на сосудистую систему мозга