- Dermatology

Содержание
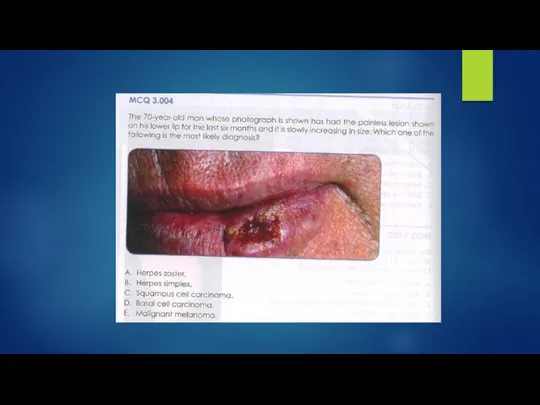
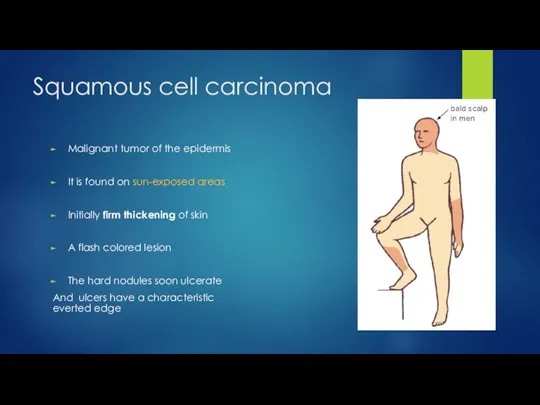
- 5. Squamous cell carcinoma Malignant tumor of the epidermis It is found on sun-exposed areas Initially firm
- 6. Squamous cell carcinoma
- 7. Basal cell carcinoma Slowly growing plaque or nodule Skin coloured, pink or pigmented Varies in size
- 8. Basal Cell Carcinoma
- 9. Basal Cell Carcinoma
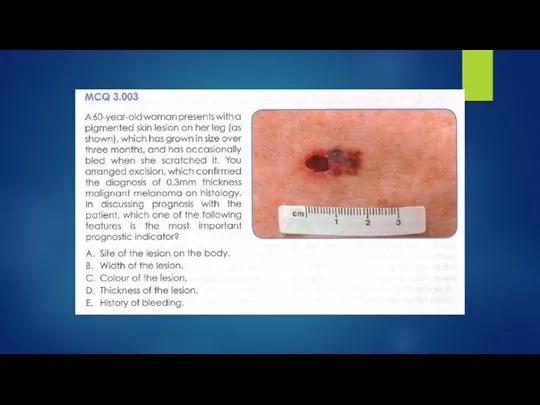
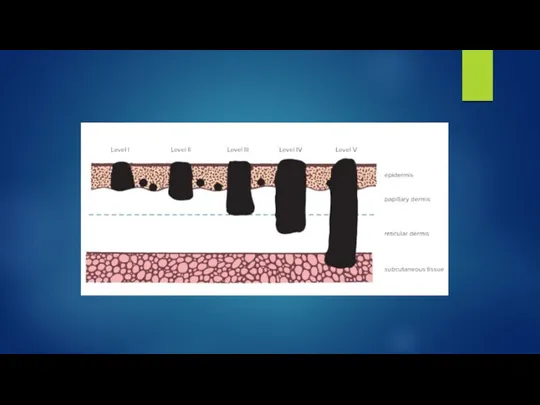
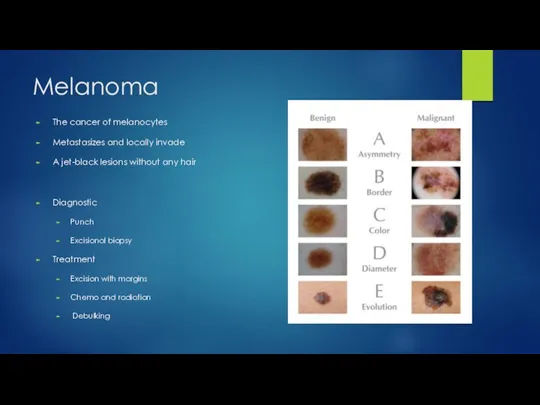
- 10. Melanoma The cancer of melanocytes Metastasizes and locally invade A jet-black lesions without any hair Diagnostic
- 11. Melanoma
- 12. Melanoma Red flag pointers
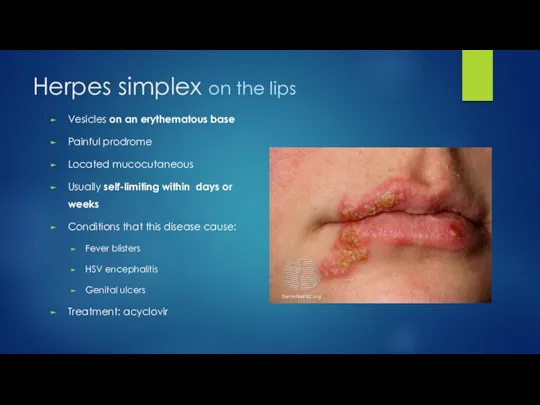
- 13. Herpes simplex on the lips Vesicles on an erythematous base Painful prodrome Located mucocutaneous Usually self-limiting
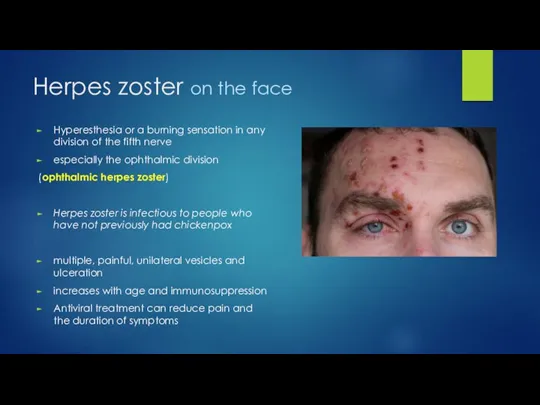
- 14. Herpes zoster on the face Hyperesthesia or a burning sensation in any division of the fifth
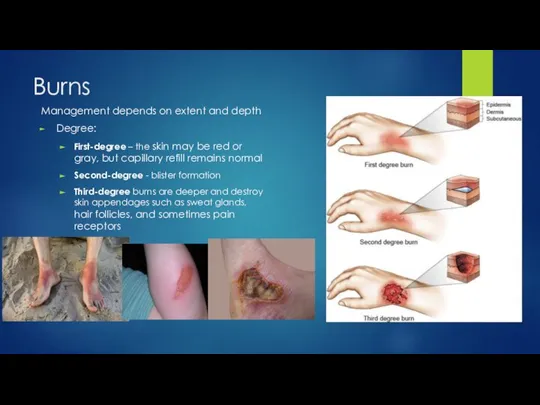
- 16. Burns Management depends on extent and depth Degree: First-degree – the skin may be red or
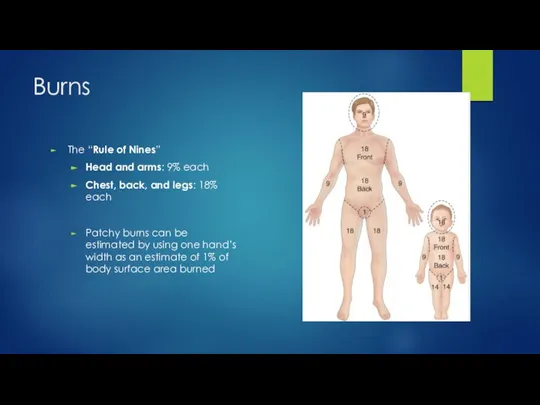
- 17. Burns The “Rule of Nines” Head and arms: 9% each Chest, back, and legs: 18% each
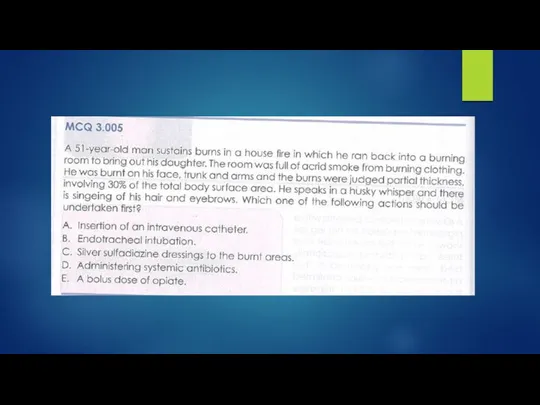
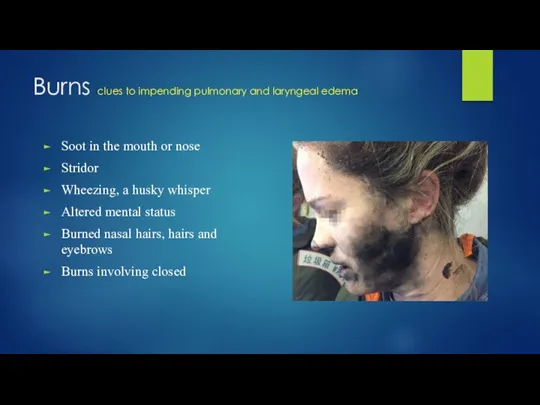
- 18. Burns clues to impending pulmonary and laryngeal edema Soot in the mouth or nose Stridor Wheezing,
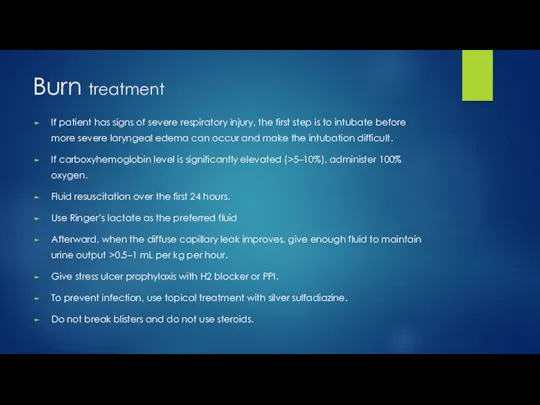
- 19. Burn treatment If patient has signs of severe respiratory injury, the first step is to intubate
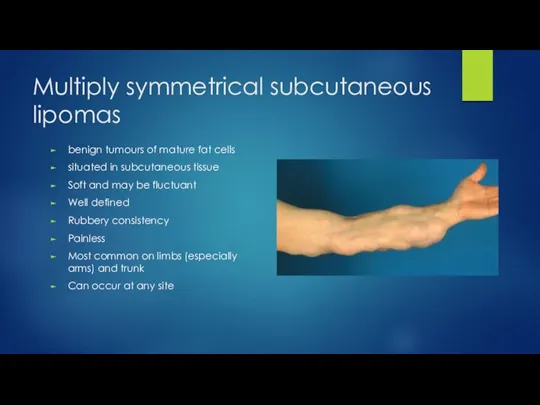
- 21. Multiply symmetrical subcutaneous lipomas benign tumours of mature fat cells situated in subcutaneous tissue Soft and
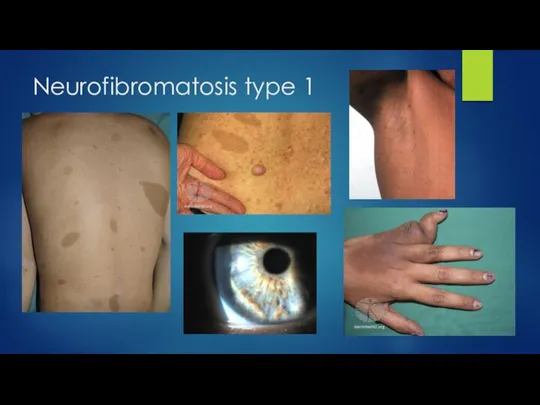
- 22. Neurofibromatosis type 1 von Recklinghausen disorder Clinical features Six or more café-au-lait spots Freckling in the
- 23. Neurofibromatosis type 1
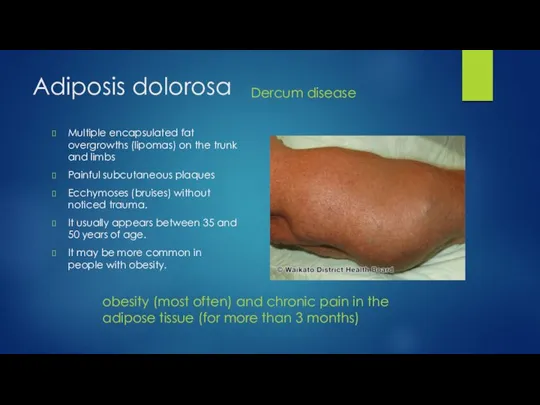
- 24. Adiposis dolorosa obesity (most often) and chronic pain in the adipose tissue (for more than 3
- 25. Dermoid cyst The most common location for dermoid cysts is the lateral third of the eyebrows;
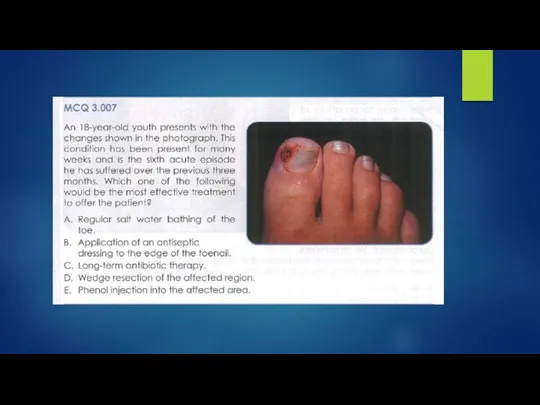
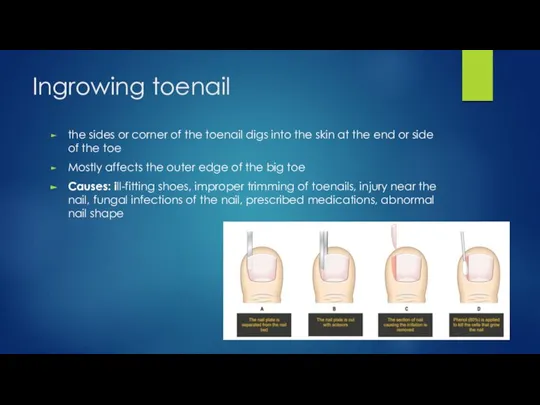
- 27. Ingrowing toenail the sides or corner of the toenail digs into the skin at the end
- 28. Ingrowing toenail
- 29. The end
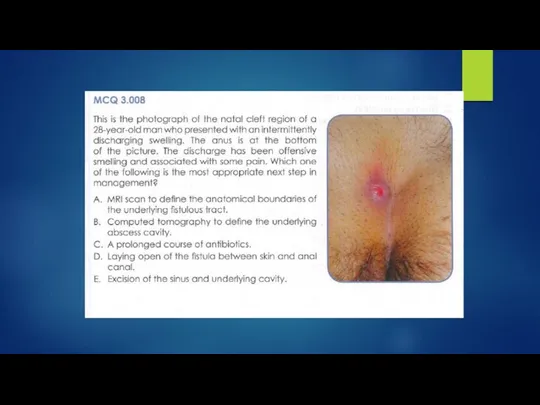
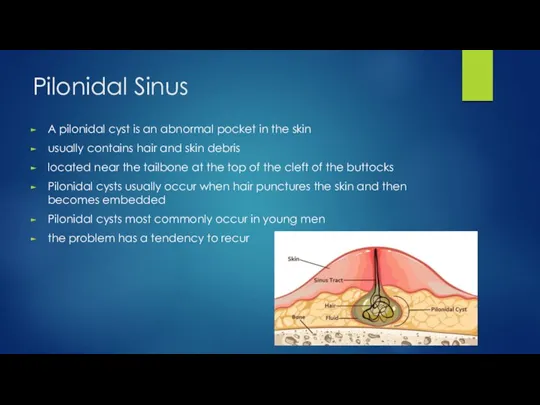
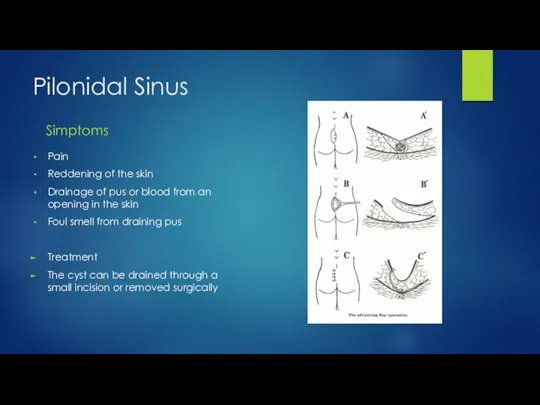
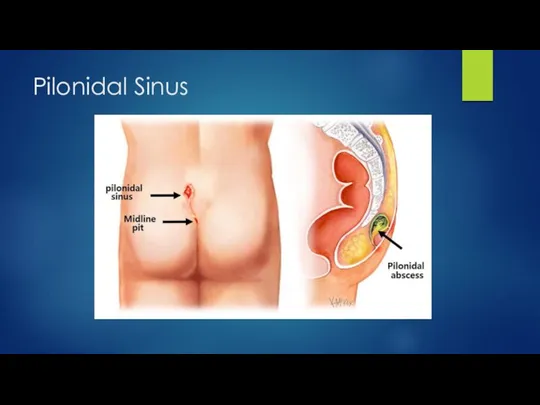
- 32. Pilonidal Sinus A pilonidal cyst is an abnormal pocket in the skin usually contains hair and
- 33. Pilonidal Sinus Simptoms Pain Reddening of the skin Drainage of pus or blood from an opening
- 34. Pilonidal Sinus
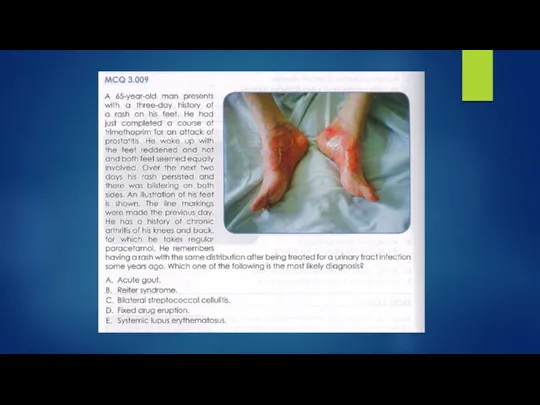
- 36. Fixed drug eruption trimethoprim Treatment To recognise the offending agent and withdraw it The rash should
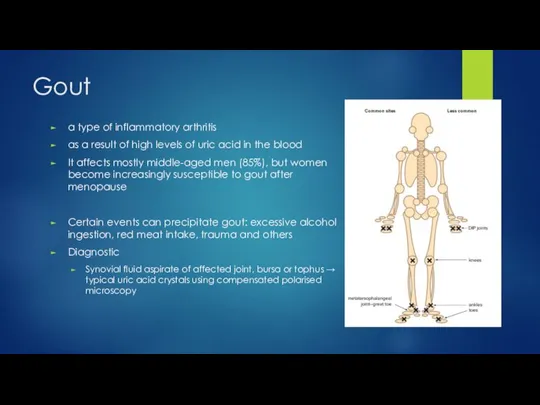
- 37. Gout a type of inflammatory arthritis as a result of high levels of uric acid in
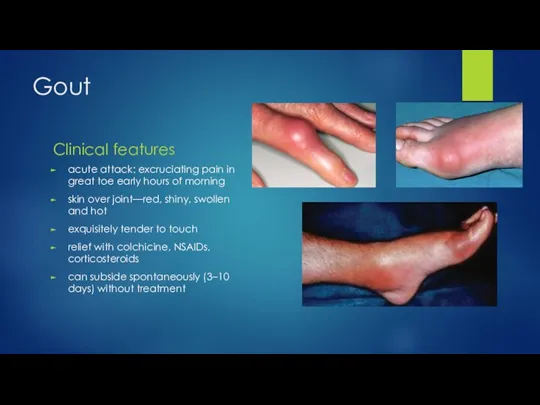
- 38. Gout Clinical features acute attack: excruciating pain in great toe early hours of morning skin over
- 39. Gout good advice and patient education information provision of rapid pain relief preventing further attacks prevention
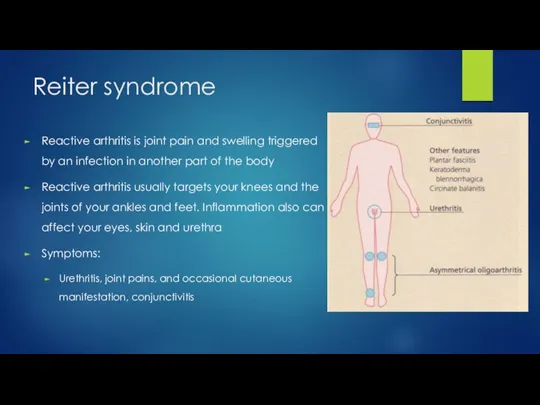
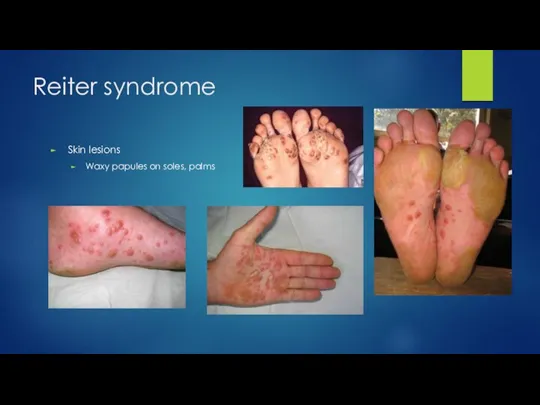
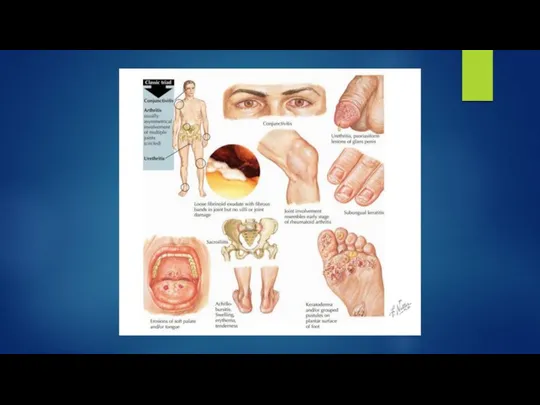
- 40. Reiter syndrome Reactive arthritis is joint pain and swelling triggered by an infection in another part
- 41. Reiter syndrome Skin lesions Waxy papules on soles, palms
- 43. Bilateral streptococcal cellulitis Cellulitis is a common bacterial infection a localised area of red, painful, swollen
- 44. Cellulitis
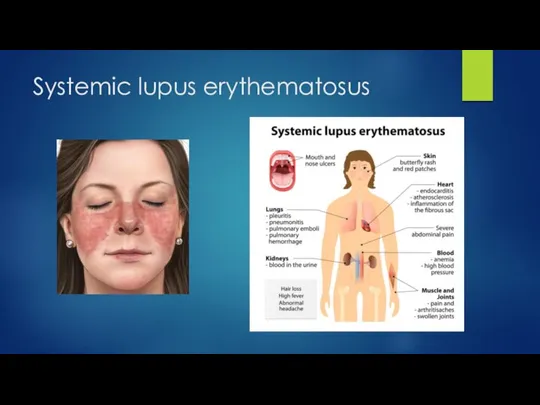
- 45. Systemic lupus erythematosus
- 46. Systemic lupus erythematosus DxT Polyarthritis + fatigue + skin lesion
- 48. Bairnsdale’ ulcer (Buruli ulcer) by the bacterium Mycobacterium ulcerans usually begins as a painless papule or
- 49. Actinic keratosis Seborhhoeic keratosis
- 50. Actinic keratosis Seborhhoeic keratosis Actinic keratosis is a scaly spot found on sun-damaged skin It is
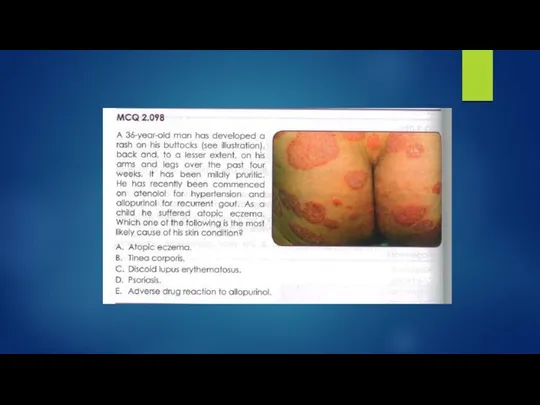
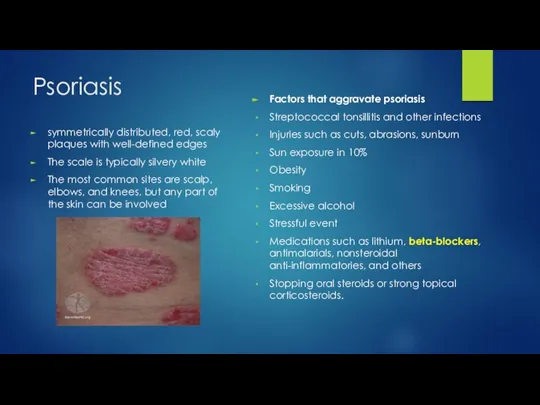
- 52. Psoriasis symmetrically distributed, red, scaly plaques with well-defined edges The scale is typically silvery white The
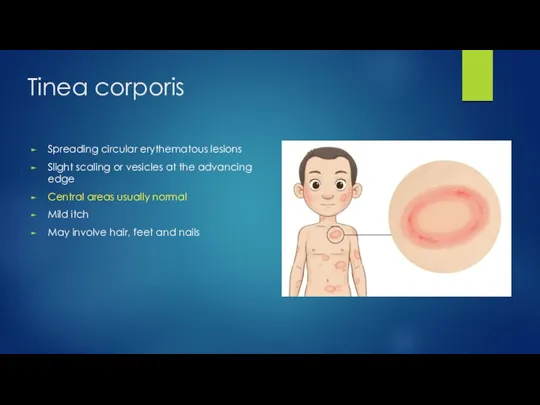
- 53. Tinea corporis Spreading circular erythematous lesions Slight scaling or vesicles at the advancing edge Central areas
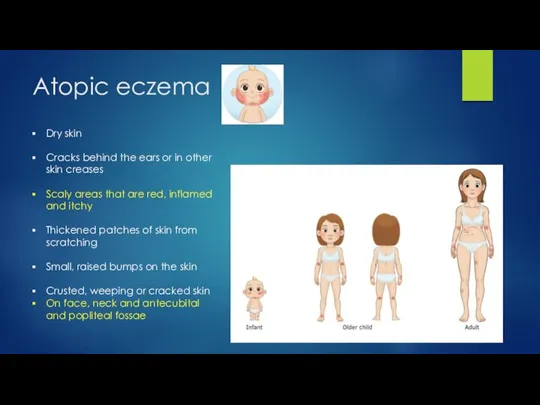
- 54. Atopic eczema Dry skin Cracks behind the ears or in other skin creases Scaly areas that
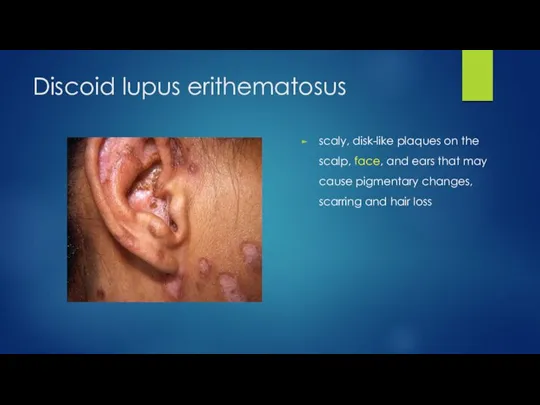
- 55. Discoid lupus erithematosus scaly, disk-like plaques on the scalp, face, and ears that may cause pigmentary
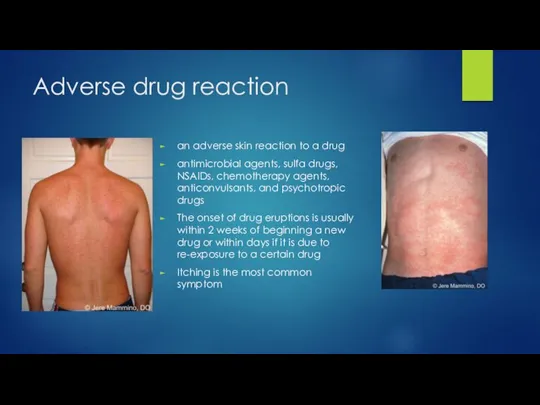
- 56. Adverse drug reaction an adverse skin reaction to a drug antimicrobial agents, sulfa drugs, NSAIDs, chemotherapy
- 59. Скачать презентацию
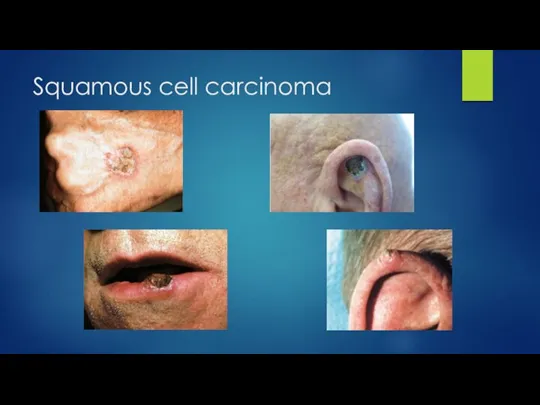
Слайд 5Squamous cell carcinoma
Malignant tumor of the epidermis
It is found on sun-exposed areas
Initially
Squamous cell carcinoma
Malignant tumor of the epidermis
It is found on sun-exposed areas
Initially
Слайд 6Squamous cell carcinoma
Squamous cell carcinoma
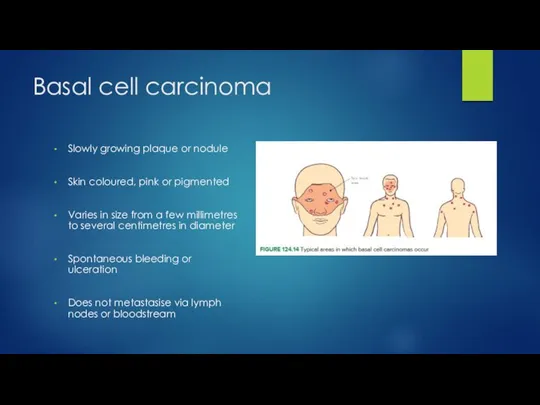
Слайд 7Basal cell carcinoma
Slowly growing plaque or nodule
Skin coloured, pink or pigmented
Varies in
Basal cell carcinoma
Slowly growing plaque or nodule
Skin coloured, pink or pigmented
Varies in
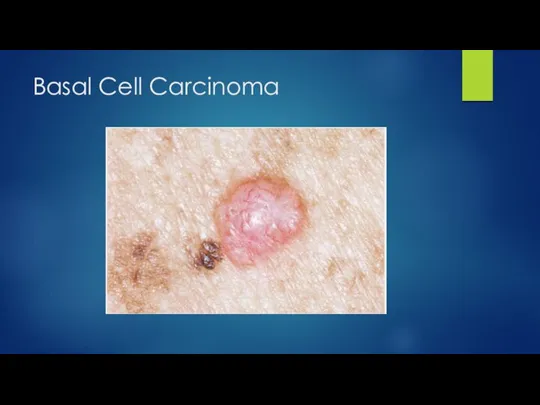
Слайд 8Basal Cell Carcinoma
Basal Cell Carcinoma
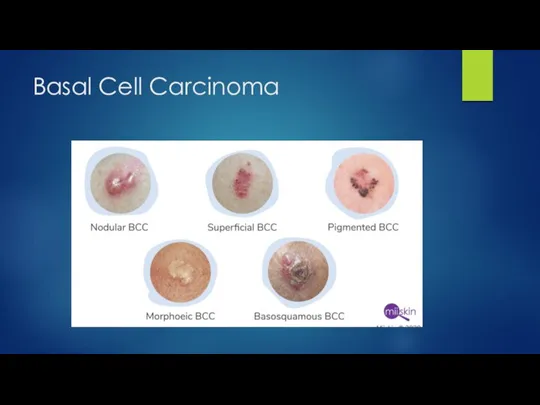
Слайд 9Basal Cell Carcinoma
Basal Cell Carcinoma
Слайд 10Melanoma
The cancer of melanocytes
Metastasizes and locally invade
A jet-black lesions without any hair
Diagnostic
Punch
Excisional
Melanoma
The cancer of melanocytes
Metastasizes and locally invade
A jet-black lesions without any hair
Diagnostic
Punch
Excisional
Слайд 11Melanoma
Melanoma
Слайд 12Melanoma
Red flag pointers
Melanoma
Red flag pointers

Слайд 13Herpes simplex on the lips
Vesicles on an erythematous base
Painful prodrome
Located mucocutaneous
Usually self-limiting
Herpes simplex on the lips
Vesicles on an erythematous base
Painful prodrome
Located mucocutaneous
Usually self-limiting
Слайд 14Herpes zoster on the face
Hyperesthesia or a burning sensation in any division
Herpes zoster on the face
Hyperesthesia or a burning sensation in any division
Слайд 16Burns
Management depends on extent and depth
Degree:
First-degree – the skin may be red
Burns
Management depends on extent and depth
Degree:
First-degree – the skin may be red
Слайд 17Burns
The “Rule of Nines”
Head and arms: 9% each
Chest, back, and legs:
Burns
The “Rule of Nines”
Head and arms: 9% each
Chest, back, and legs:
Слайд 18Burns clues to impending pulmonary and laryngeal edema
Soot in the mouth or
Burns clues to impending pulmonary and laryngeal edema
Soot in the mouth or
Слайд 19Burn treatment
If patient has signs of severe respiratory injury, the first
Burn treatment
If patient has signs of severe respiratory injury, the first
Слайд 21Multiply symmetrical subcutaneous lipomas
benign tumours of mature fat cells
situated in subcutaneous tissue
Soft
Multiply symmetrical subcutaneous lipomas
benign tumours of mature fat cells
situated in subcutaneous tissue
Soft
Слайд 22Neurofibromatosis type 1
von Recklinghausen disorder
Clinical features
Six or more café-au-lait spots
Freckling
Neurofibromatosis type 1
von Recklinghausen disorder
Clinical features
Six or more café-au-lait spots
Freckling
Слайд 23Neurofibromatosis type 1
Neurofibromatosis type 1
Слайд 24Adiposis dolorosa
obesity (most often) and chronic pain in the adipose tissue
Adiposis dolorosa
obesity (most often) and chronic pain in the adipose tissue
Слайд 25Dermoid cyst
The most common location for dermoid cysts is the lateral third
Dermoid cyst
The most common location for dermoid cysts is the lateral third
Слайд 27Ingrowing toenail
the sides or corner of the toenail digs into the skin
Ingrowing toenail
the sides or corner of the toenail digs into the skin
Слайд 28Ingrowing toenail
Ingrowing toenail

Слайд 29The end
The end

Слайд 32Pilonidal Sinus
A pilonidal cyst is an abnormal pocket in the skin
usually contains
Pilonidal Sinus
A pilonidal cyst is an abnormal pocket in the skin
usually contains
Слайд 33Pilonidal Sinus
Simptoms
Pain
Reddening of the skin
Drainage of pus or blood from an opening
Pilonidal Sinus
Simptoms
Pain
Reddening of the skin
Drainage of pus or blood from an opening
Слайд 34Pilonidal Sinus
Pilonidal Sinus
Слайд 36Fixed drug eruption
trimethoprim
Treatment
To recognise the offending agent
and withdraw it
The rash should
Fixed drug eruption
trimethoprim
Treatment
To recognise the offending agent
and withdraw it
The rash should
Слайд 37Gout
a type of inflammatory arthritis
as a result of high levels of uric
Gout
a type of inflammatory arthritis
as a result of high levels of uric
Слайд 38Gout
Clinical features
acute attack: excruciating pain in great toe early hours of morning
skin
Gout
Clinical features
acute attack: excruciating pain in great toe early hours of morning
skin
Слайд 39Gout
good advice and patient education information
provision of rapid pain relief
preventing further attacks
prevention
Gout
good advice and patient education information
provision of rapid pain relief
preventing further attacks
prevention
Слайд 40Reiter syndrome
Reactive arthritis is joint pain and swelling triggered by an infection
Reiter syndrome
Reactive arthritis is joint pain and swelling triggered by an infection
Слайд 41Reiter syndrome
Skin lesions
Waxy papules on soles, palms
Reiter syndrome
Skin lesions
Waxy papules on soles, palms
Слайд 43Bilateral streptococcal cellulitis
Cellulitis is a common bacterial infection
a localised area of red,
Bilateral streptococcal cellulitis
Cellulitis is a common bacterial infection
a localised area of red,
Слайд 44Cellulitis
Cellulitis

Слайд 45Systemic lupus erythematosus
Systemic lupus erythematosus
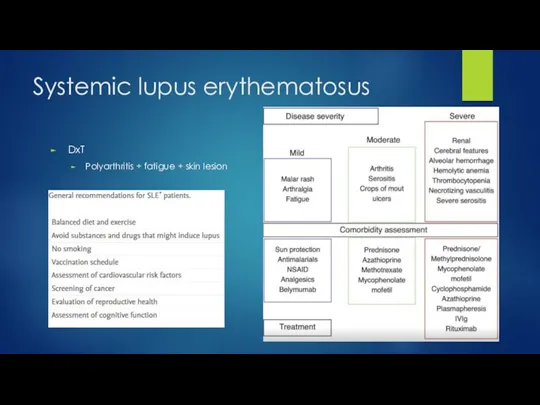
Слайд 46Systemic lupus erythematosus
DxT
Polyarthritis + fatigue + skin lesion
Systemic lupus erythematosus
DxT
Polyarthritis + fatigue + skin lesion
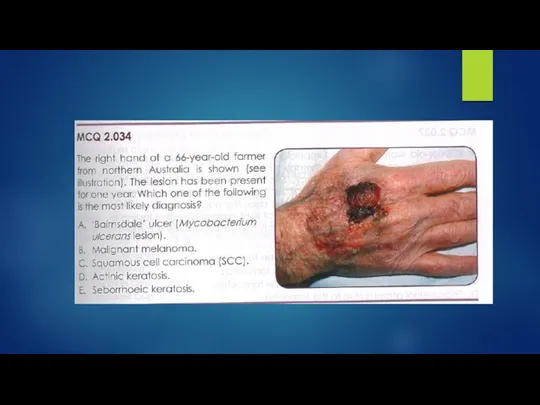
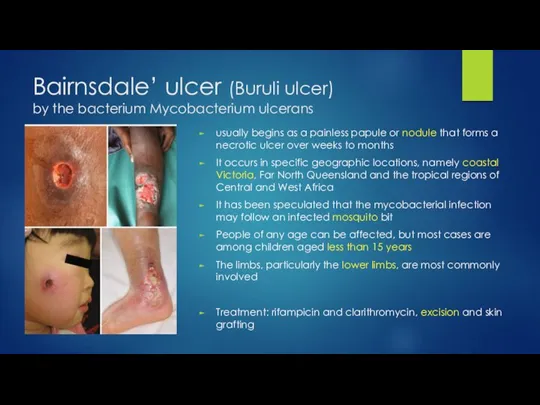
Слайд 48Bairnsdale’ ulcer (Buruli ulcer)
by the bacterium Mycobacterium ulcerans
usually begins as a painless
Bairnsdale’ ulcer (Buruli ulcer)
by the bacterium Mycobacterium ulcerans
usually begins as a painless
Слайд 49Actinic keratosis
Seborhhoeic keratosis
Actinic keratosis
Seborhhoeic keratosis

Слайд 50Actinic keratosis
Seborhhoeic keratosis
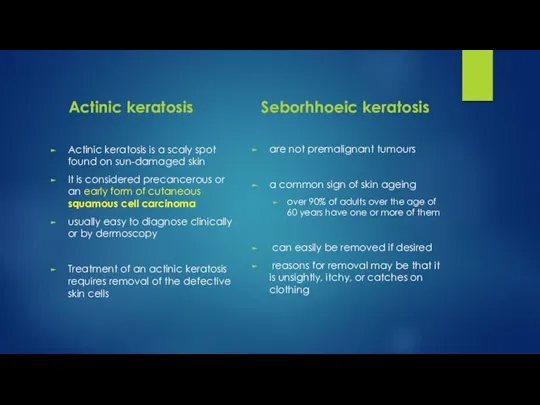
Actinic keratosis is a scaly spot found on sun-damaged skin
It
Actinic keratosis
Seborhhoeic keratosis
Actinic keratosis is a scaly spot found on sun-damaged skin
It
Слайд 52Psoriasis
symmetrically distributed, red, scaly plaques with well-defined edges
The scale is typically silvery
Psoriasis
symmetrically distributed, red, scaly plaques with well-defined edges
The scale is typically silvery
Слайд 53Tinea corporis
Spreading circular erythematous lesions
Slight scaling or vesicles at the advancing edge
Central
Tinea corporis
Spreading circular erythematous lesions
Slight scaling or vesicles at the advancing edge
Central
Слайд 54Atopic eczema
Dry skin
Cracks behind the ears or in other skin creases
Scaly areas
Atopic eczema
Dry skin
Cracks behind the ears or in other skin creases
Scaly areas
Слайд 55Discoid lupus erithematosus
scaly, disk-like plaques on the scalp, face, and ears that
Discoid lupus erithematosus
scaly, disk-like plaques on the scalp, face, and ears that
Слайд 56Adverse drug reaction
an adverse skin reaction to a drug
antimicrobial agents, sulfa drugs,
Adverse drug reaction
an adverse skin reaction to a drug
antimicrobial agents, sulfa drugs,
 5 ярких представителей профессии: врач
5 ярких представителей профессии: врач Генетика олигофрений. Клинически очерченные генетические синдромы с неясным ходом наследия
Генетика олигофрений. Клинически очерченные генетические синдромы с неясным ходом наследия Артериальное давление и пульс – показатели состояния сердечно – сосудистой системы
Артериальное давление и пульс – показатели состояния сердечно – сосудистой системы Лекарственные растения содержащие флавоноиды. Onosis arvensis (стальник полевой)
Лекарственные растения содержащие флавоноиды. Onosis arvensis (стальник полевой) Создание новой модели организации, оказывающей первичную медико-санитарную помощь по системе 5S
Создание новой модели организации, оказывающей первичную медико-санитарную помощь по системе 5S Ятрогении, основные понятия, классификация, профилактика
Ятрогении, основные понятия, классификация, профилактика Адаптационные изменения в организме женщины при беременности. Нормы беременности (Лекция № 3 для студентов 4 курса)
Адаптационные изменения в организме женщины при беременности. Нормы беременности (Лекция № 3 для студентов 4 курса) Нарколепсия. Описание клинического наблюдения
Нарколепсия. Описание клинического наблюдения Обследование ребенка с РАС
Обследование ребенка с РАС Тип фигуры
Тип фигуры Доврачебная медицинская помощь и особенности проведения реанимационных мероприятий
Доврачебная медицинская помощь и особенности проведения реанимационных мероприятий Вскармливание детей до 1 года. Грудное (естественное). Смешанное. Искусственное
Вскармливание детей до 1 года. Грудное (естественное). Смешанное. Искусственное Критерии персонализированного подхода к выбору режима высокообъёмной гемофильтрации при лечении пациентов с сепсисом
Критерии персонализированного подхода к выбору режима высокообъёмной гемофильтрации при лечении пациентов с сепсисом Медицинская арахноэнтомология. Лекция 08
Медицинская арахноэнтомология. Лекция 08 Гинекологичексий сепсис
Гинекологичексий сепсис Анатомия коленного сустава
Анатомия коленного сустава Острая кишечная непроходимость
Острая кишечная непроходимость Профилактика акушерского травматизма. Реабилитация родильниц
Профилактика акушерского травматизма. Реабилитация родильниц Поражение органов-мишеней
Поражение органов-мишеней Приемное отделение. Выполнение установленных объемов (случаи госпитализации)
Приемное отделение. Выполнение установленных объемов (случаи госпитализации) Патография Фридриха Ницше (1844-1900)
Патография Фридриха Ницше (1844-1900) Әсемділікті қалыптастыратын факторлар
Әсемділікті қалыптастыратын факторлар Сонный паралич
Сонный паралич Отморожения. Электротравма
Отморожения. Электротравма Иркутский государственный медицинский университет. Кафедра анестезиологии-реаниматологии
Иркутский государственный медицинский университет. Кафедра анестезиологии-реаниматологии Опиоиды как адъюванты для регионарной анестезии
Опиоиды как адъюванты для регионарной анестезии Фитоэстрин. Негормональный комплекс для женщин
Фитоэстрин. Негормональный комплекс для женщин Методы диагностики хронического пиелонефрита
Методы диагностики хронического пиелонефрита