- Infective endocarditis

Содержание
- 2. Infection most commonly involves heart valves (either native or prostatic) but may also occur on the
- 3. Incidence – 2.6-7:100,000 in the western world. Increasing among elderly. Predisposition – congenital heart disease, rheumatic
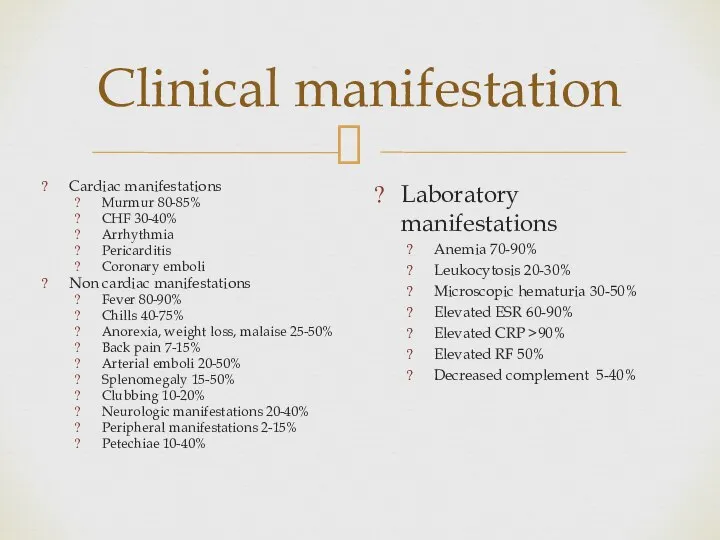
- 4. Clinical manifestation Cardiac manifestations Murmur 80-85% CHF 30-40% Arrhythmia Pericarditis Coronary emboli Non cardiac manifestations Fever
- 5. Clinical manifestations
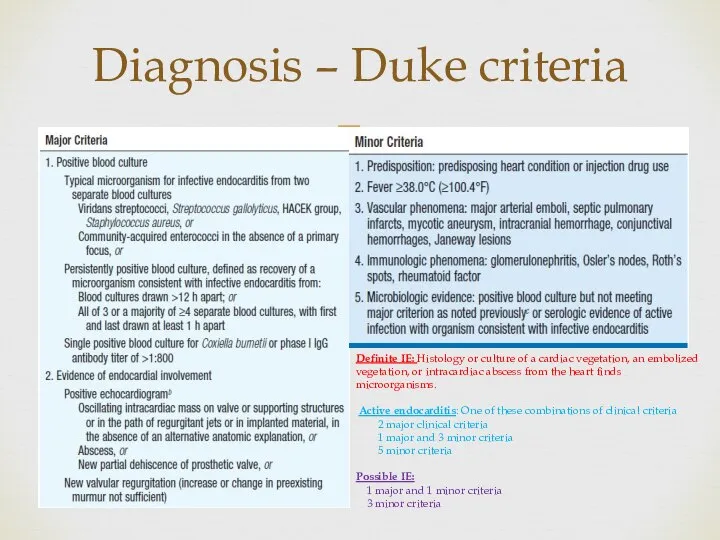
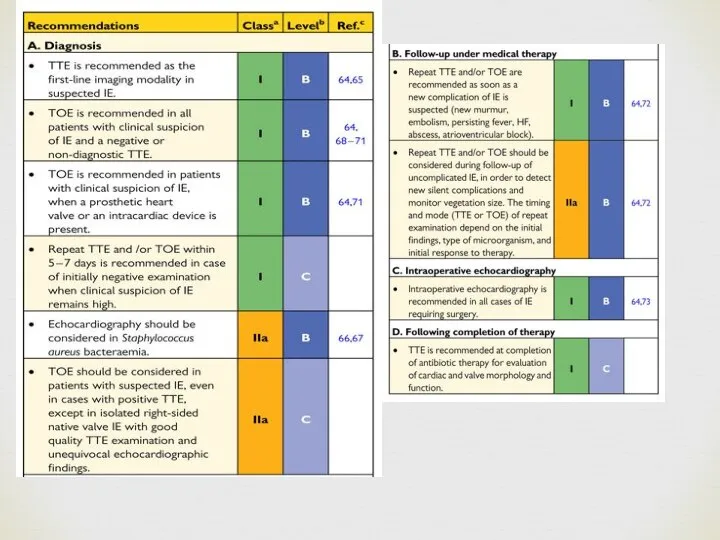
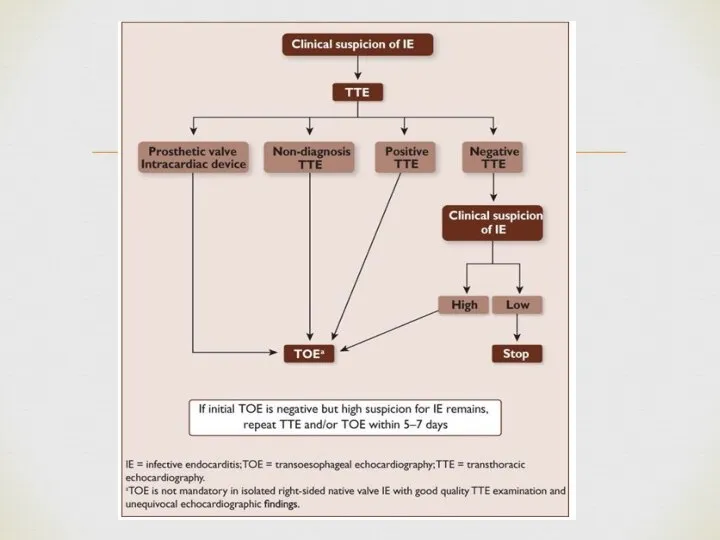
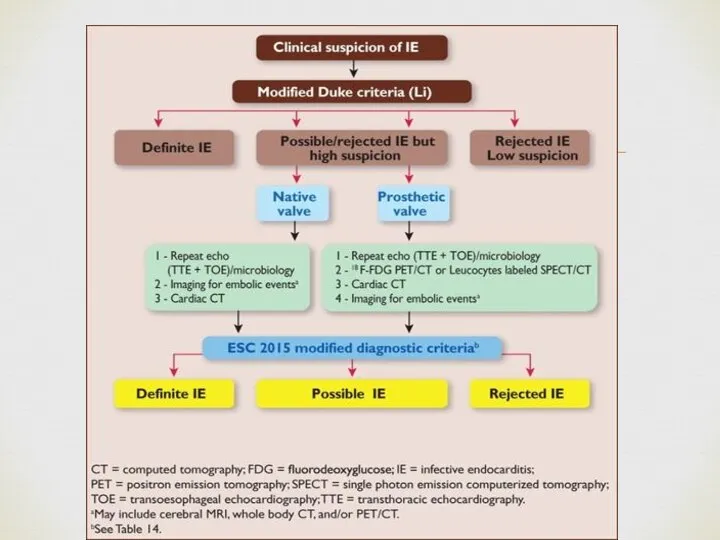
- 6. Diagnosis – Duke criteria Definite IE: Histology or culture of a cardiac vegetation, an embolized vegetation,
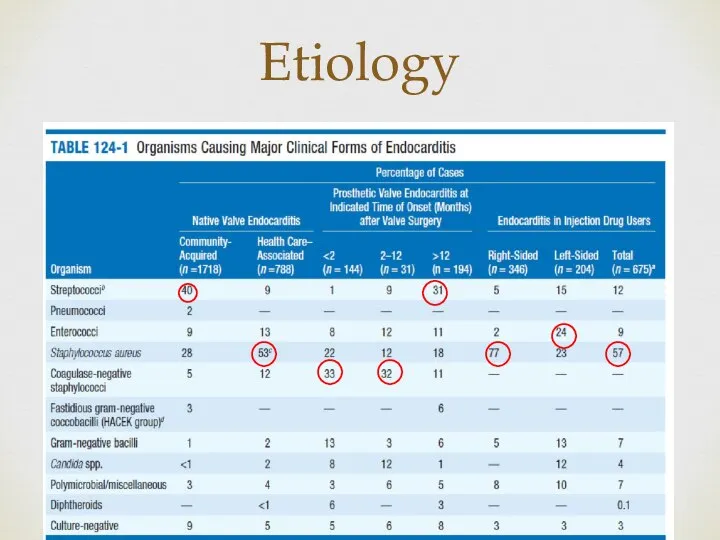
- 10. Etiology
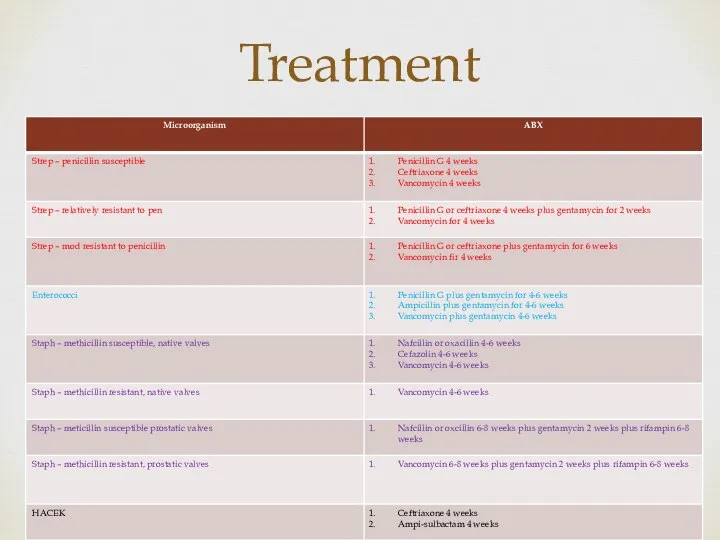
- 11. Treatment
- 12. B. quintana and B. henselae are the most common bartonella spp. implicated in endocarditis. Native valves
- 13. C. brunetti Gram neg cocco-bacillus Primary sources – cattle, sheep and goats Incidence – 24-54 cases
- 14. Main complications of left-sided valve infective endocarditis and their management HF is the most frequent and
- 15. Uncontrolled infection Perivalvular extension of IE is the most frequent cause of uncontrolled infection and is
- 16. Neurological complications Symptomatic neurological events develop in 15–30% of all patients with IE and additional silent
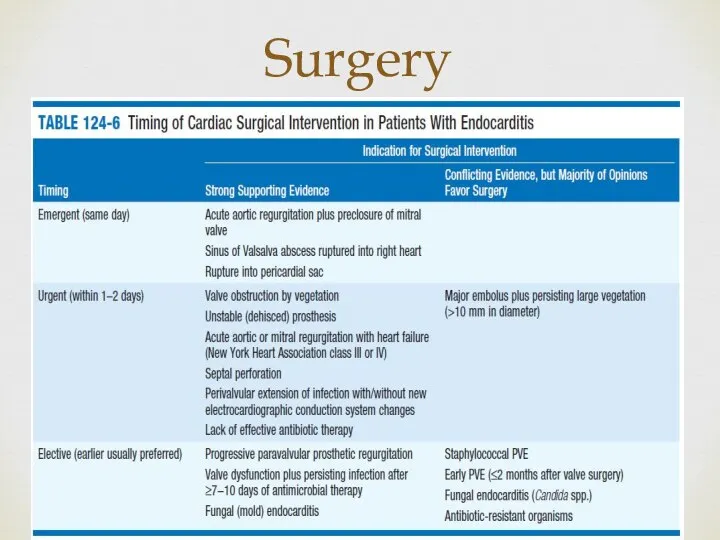
- 17. Surgery
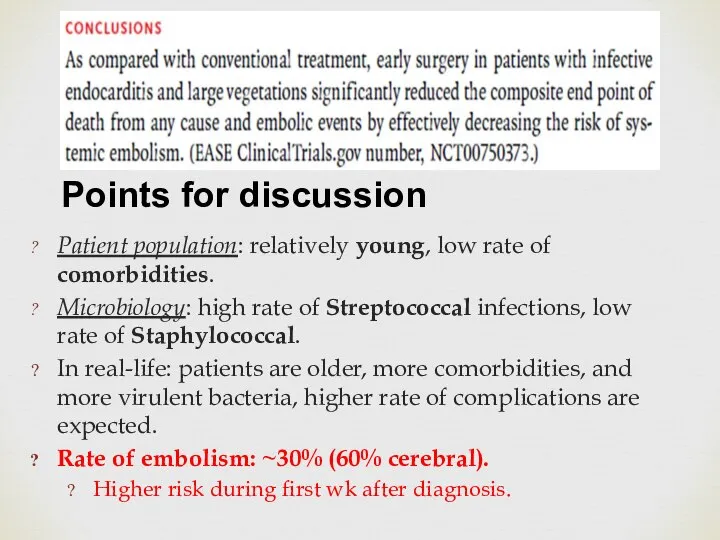
- 24. Patient population: relatively young, low rate of comorbidities. Microbiology: high rate of Streptococcal infections, low rate
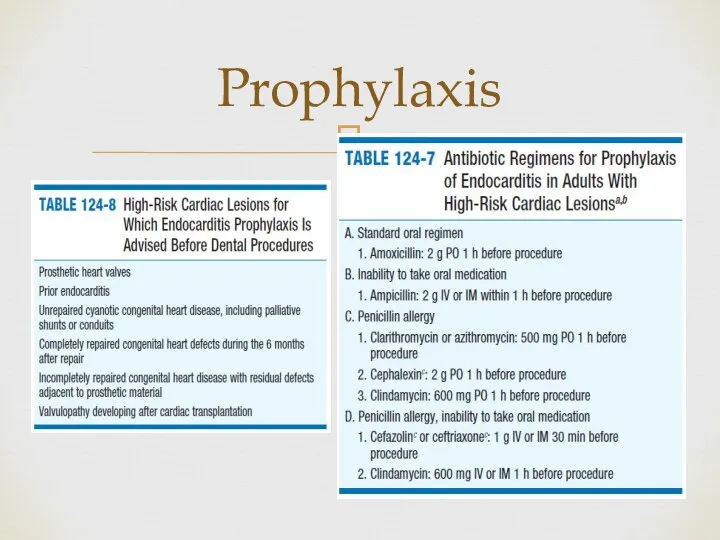
- 25. Prophylaxis
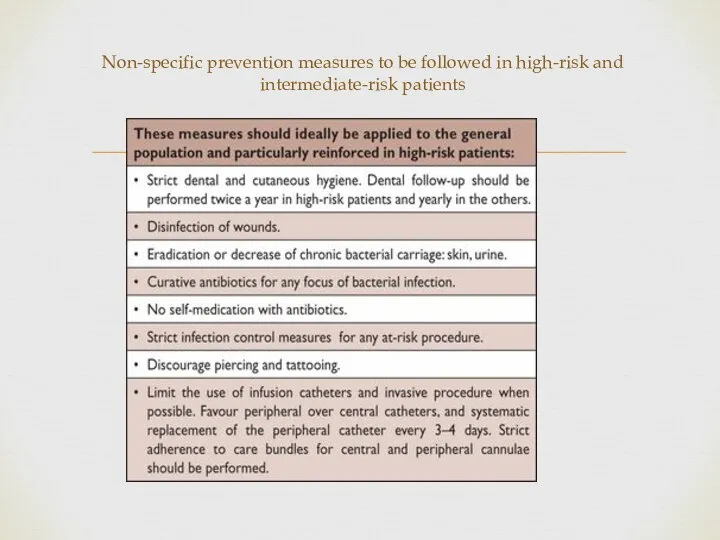
- 26. Non-specific prevention measures to be followed in high-risk and intermediate-risk patients
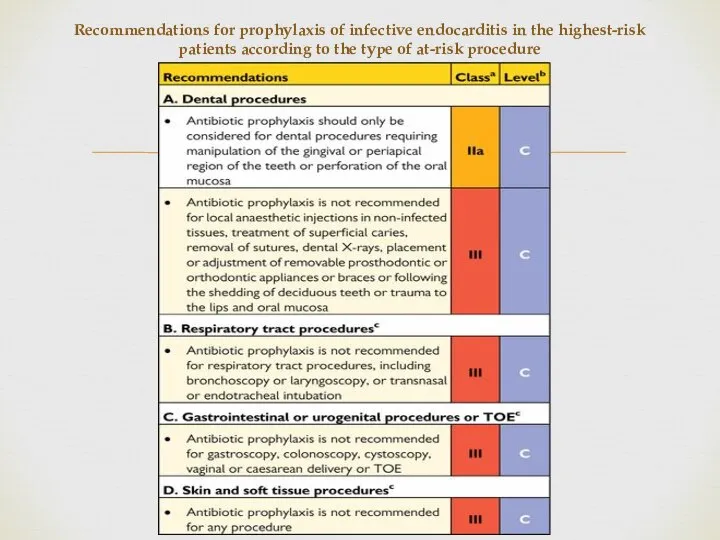
- 27. Recommendations for prophylaxis of infective endocarditis in the highest-risk patients according to the type of at-risk
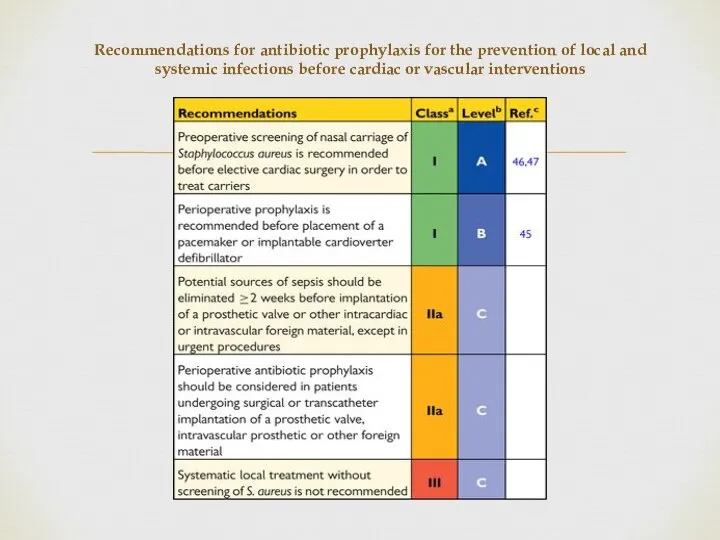
- 28. Recommendations for antibiotic prophylaxis for the prevention of local and systemic infections before cardiac or vascular
- 29. 49y male Staphylococcus aureus NVE 3 weeks of IV antibiotics Undergoing MVR due to ruptured chorda
- 30. How do you count the duration of therapy? It is reasonable that the counting of days
- 32. Скачать презентацию
Слайд 3Incidence – 2.6-7:100,000 in the western world. Increasing among elderly.
Predisposition –
Incidence – 2.6-7:100,000 in the western world. Increasing among elderly.
Predisposition –
Слайд 4Clinical manifestation
Cardiac manifestations
Murmur 80-85%
CHF 30-40%
Arrhythmia
Pericarditis
Coronary emboli
Non cardiac manifestations
Fever 80-90%
Chills 40-75%
Anorexia, weight
Clinical manifestation
Cardiac manifestations
Murmur 80-85%
CHF 30-40%
Arrhythmia
Pericarditis
Coronary emboli
Non cardiac manifestations
Fever 80-90%
Chills 40-75%
Anorexia, weight
Слайд 5Clinical manifestations
Clinical manifestations

Слайд 6Diagnosis – Duke criteria
Definite IE: Histology or culture of a cardiac vegetation,
Diagnosis – Duke criteria
Definite IE: Histology or culture of a cardiac vegetation,
Слайд 10Etiology
Etiology
Слайд 11Treatment
Treatment
Слайд 12B. quintana and B. henselae are the most common bartonella spp. implicated
Слайд 13C. brunetti
Gram neg cocco-bacillus
Primary sources – cattle, sheep and goats
Incidence – 24-54
C. brunetti
Gram neg cocco-bacillus
Primary sources – cattle, sheep and goats
Incidence – 24-54
Слайд 14Main complications of left-sided valve infective endocarditis and their management
HF is the
Main complications of left-sided valve infective endocarditis and their management
HF is the
Слайд 15Uncontrolled infection
Perivalvular extension of IE is the most frequent cause of uncontrolled
Uncontrolled infection
Perivalvular extension of IE is the most frequent cause of uncontrolled
Слайд 16Neurological complications
Symptomatic neurological events develop in 15–30% of all patients with IE
Neurological complications
Symptomatic neurological events develop in 15–30% of all patients with IE
Слайд 17Surgery
Surgery
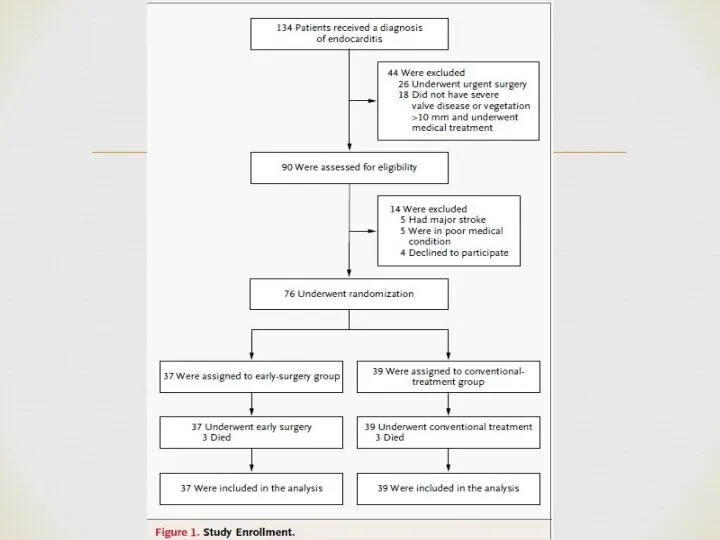
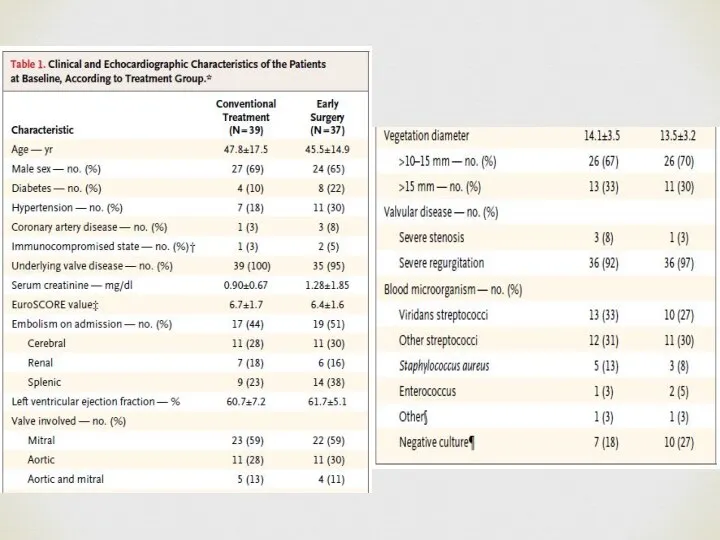
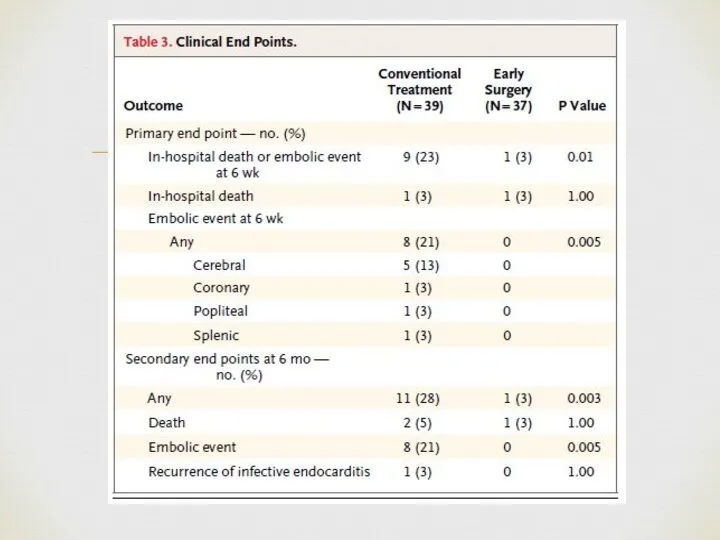
Слайд 24Patient population: relatively young, low rate of comorbidities.
Microbiology: high rate of Streptococcal
Patient population: relatively young, low rate of comorbidities.
Microbiology: high rate of Streptococcal
Слайд 25Prophylaxis
Prophylaxis
Слайд 26Non-specific prevention measures to be followed in high-risk and intermediate-risk patients
Non-specific prevention measures to be followed in high-risk and intermediate-risk patients
Слайд 27Recommendations for prophylaxis of infective endocarditis in the highest-risk patients according to
Recommendations for prophylaxis of infective endocarditis in the highest-risk patients according to
Слайд 28Recommendations for antibiotic prophylaxis for the prevention of local and systemic infections
Recommendations for antibiotic prophylaxis for the prevention of local and systemic infections
Слайд 2949y male
Staphylococcus aureus NVE
3 weeks of IV antibiotics
Undergoing MVR due to ruptured
49y male
Staphylococcus aureus NVE
3 weeks of IV antibiotics
Undergoing MVR due to ruptured
Слайд 30How do you count the duration of therapy?
It is reasonable that the
How do you count the duration of therapy?
It is reasonable that the
 Санитарно – эпидемиологический режим
Санитарно – эпидемиологический режим Синдром раздраженного кишечника
Синдром раздраженного кишечника Методы выявления туберкулеза
Методы выявления туберкулеза Аллергические заболевания и их профилактика
Аллергические заболевания и их профилактика NK-клетки (natural killer cells) и их эффекторные функции
NK-клетки (natural killer cells) и их эффекторные функции Изменение свойств пыльцы (часть 2)
Изменение свойств пыльцы (часть 2) Про туберкульоз
Про туберкульоз Майлардың алмасуынан пайда болатын аурулар
Майлардың алмасуынан пайда болатын аурулар Анатомия коленного сустава
Анатомия коленного сустава Профилактика и лечение послеоперационного гипопаратиреоза
Профилактика и лечение послеоперационного гипопаратиреоза Современные аспекты лабораторной диагностики поражений печени при хронических вирусных гепатитах В, С, D
Современные аспекты лабораторной диагностики поражений печени при хронических вирусных гепатитах В, С, D Cystic fibrosis
Cystic fibrosis Логопедические технологии формирования плавной речи
Логопедические технологии формирования плавной речи Методика для исследования мышления больных, процессов анализа и синтеза
Методика для исследования мышления больных, процессов анализа и синтеза Группы крови. Переливание крови
Группы крови. Переливание крови Хирургическая агрессология
Хирургическая агрессология Комбинированные и хронические лучевые поражения
Комбинированные и хронические лучевые поражения Шкала радиомагнитных волн
Шкала радиомагнитных волн Витамины
Витамины Профессия врача
Профессия врача Ксенобиотики и их роль в экологически обусловленных заболеваниях жителей Центрального Черноземья
Ксенобиотики и их роль в экологически обусловленных заболеваниях жителей Центрального Черноземья Гемотрансфузия
Гемотрансфузия Питание и здоровье
Питание и здоровье akro
akro Еңбек гигиенасы
Еңбек гигиенасы Проблемы сидячей работы
Проблемы сидячей работы Эффективность Гипорамина (Эребра) в лечении и профилактике вирусных заболеваний у детей
Эффективность Гипорамина (Эребра) в лечении и профилактике вирусных заболеваний у детей Гемолитическая болезнь новорожденных
Гемолитическая болезнь новорожденных