- ABG case studies & interpretation

Содержание
- 2. It’s not magic understanding ABG’s, it just takes a little practice!
- 3. Acid-base imbalances Metabolic acidosis Metabolic alkalosis Respiratory acidosis Respiratory alkalosis
- 4. Metabolic • METABOLIC ACIDOSIS: Decrease the HCO3 - --> the pH goes down. • Compensation: Respiratory
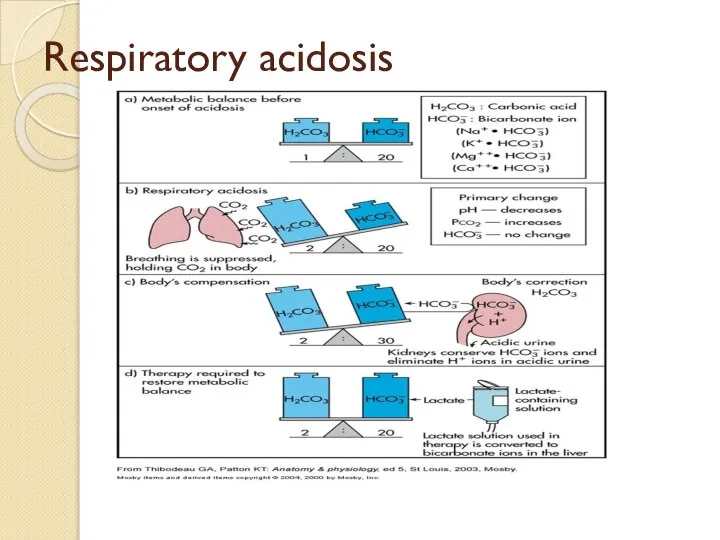
- 5. Respiratory RESPIRATORY ACIDOSIS: Increase the PCO2---> the pH goes down. Hypoventilation. Compensation: Metabolic Alkalosis can help
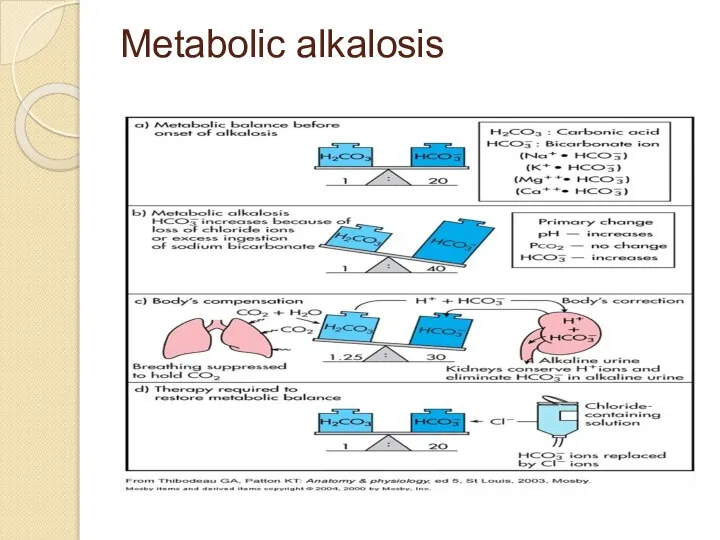
- 6. METABOLIC ALKALOSIS CAUSES: • Vomiting: Lose enough stomach acid to produce alkalosis. • Diuretics: Loop diuretics
- 7. RESPIRATORY ACIDOSIS: causes: CNS DEPRESSION DRUGS:Opiates,sedatives,anaesthetics OBESITY HYPOVENTILATION SYNDROME STROKE NEUROMUSCULAR DISORDERS: NEUROLOGIC: POLIO,GBS,TETANUS,BOTULISM MUSCULAR DYSTROPHY
- 8. RESPIRATORY ALKALOSIS Causes: High altitude. Neuromuscular disease Respiratory center depression Inadequate mechanical ventilation Sepsis Burns
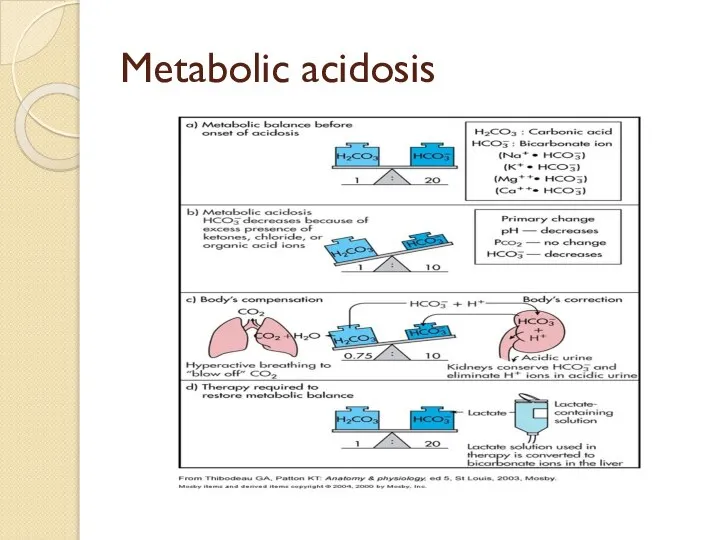
- 9. Metabolic acidosis Metabolic acidosis: Is caused by a decrease in HCO3- concentration in blood. Causes: Increased
- 10. Compensation of Metabolic acidosis: Respiratory compensation: decrease in pH stimulates respiratory center causing hyperventilation which produces
- 13. Metabolic alkalosis
- 14. Metabolic acidosis
- 15. Respiratory acidosis
- 16. Respiratory Alkalosis
- 17. Metabolic Acidosis pH 7.30 PaCO2 40 HCO3 15
- 18. Metabolic Alkalosis pH 7.50 PCO2 40 HCO3 30
- 19. Respiratory Acidosis pH 7.30 PaCO2 60 HCO3 26
- 20. Respiratory Alkalosis pH 7.50 PaCO2 25 HCO3 23
- 21. What are the compensations? • Respiratory acidosis --metabolic alkalosis • Respiratory alkalosis --metabolic acidosis • In
- 22. Buffers kick in within minutes. Respiratory compensation is rapid and starts within minutes and complete within
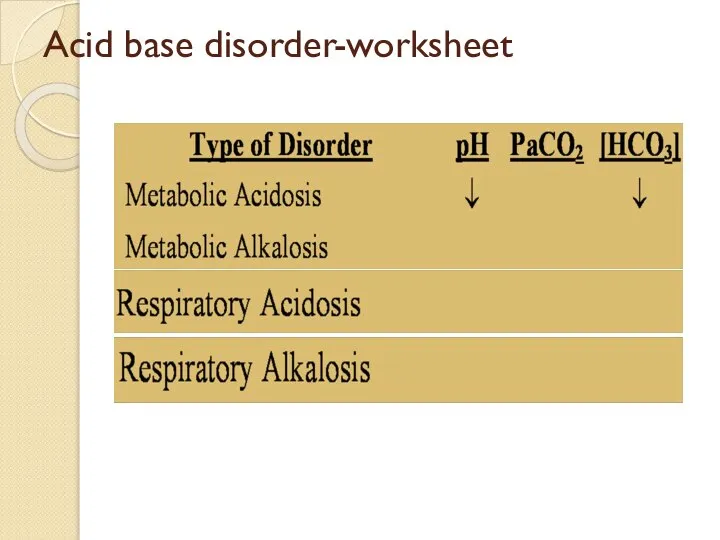
- 23. Acid base disorder-worksheet
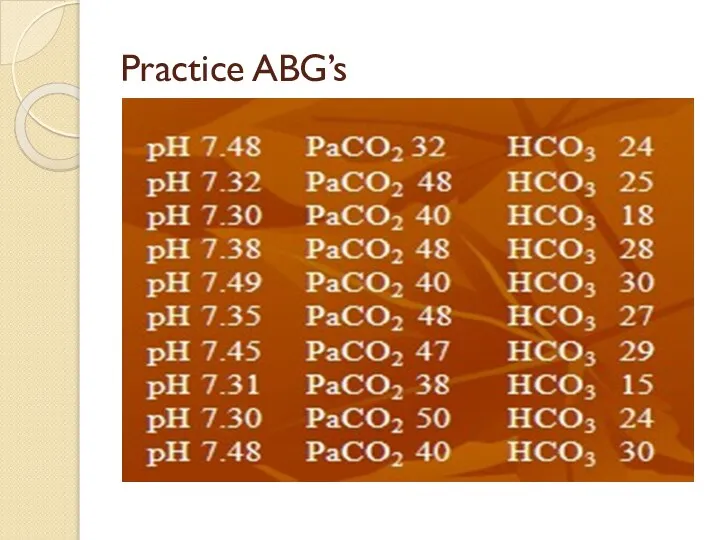
- 24. Acid base disorder-worksheet Practice ABG’s
- 25. Answers: 1. Respiratory alkalosis 2. Respiratory acidosis 3. Metabolic acidosis 4.Compensated Respiratory acidosis 5. Metabolic alkalosis
- 26. STEPS OF ASSESSING ABG STEP 1: Diagnose whether it is acidosis or alkalosis- (pH will help)
- 27. Work sheet Diarrhea may lead to----------? Acid loss due to vomiting and gastric suction may lead
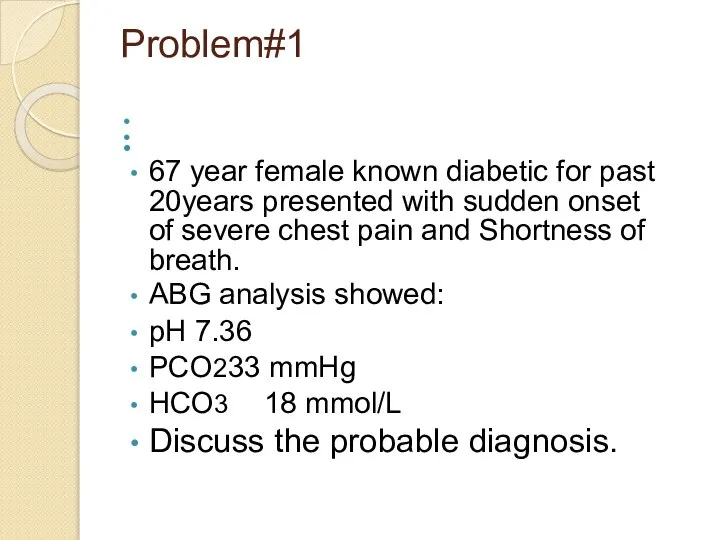
- 28. Problem#1 67 year female known diabetic for past 20years presented with sudden onset of severe chest
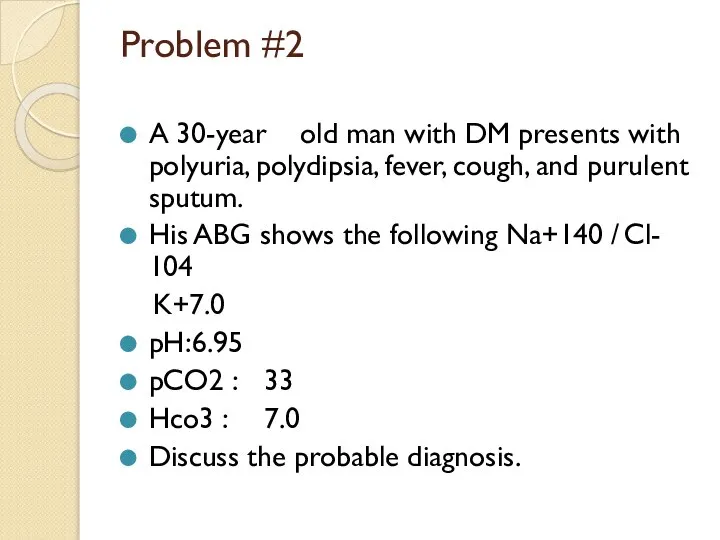
- 29. Problem #2 A 30-year old man with DM presents with polyuria, polydipsia, fever, cough, and purulent
- 30. Problem#3 45 year old male was admitted to the emergency room with complaints of mild vomiting,
- 31. Problem #4 60 year male presents to the ED from a nursing home. You have no
- 32. Problem # 5 60year old man was admitted with severe abdominal pain, which started some 2
- 34. Скачать презентацию
Слайд 3Acid-base imbalances
Metabolic acidosis
Metabolic alkalosis
Respiratory acidosis
Respiratory alkalosis
Acid-base imbalances
Metabolic acidosis
Metabolic alkalosis
Respiratory acidosis
Respiratory alkalosis
Слайд 4Metabolic
• METABOLIC ACIDOSIS: Decrease the
HCO3 - --> the pH goes down.
• Compensation: Respiratory Alkalosis
Metabolic
• METABOLIC ACIDOSIS: Decrease the
HCO3 - --> the pH goes down.
• Compensation: Respiratory Alkalosis
Слайд 5Respiratory
RESPIRATORY ACIDOSIS: Increase the PCO2---> the pH goes down. Hypoventilation. Compensation: Metabolic
Respiratory
RESPIRATORY ACIDOSIS: Increase the PCO2---> the pH goes down. Hypoventilation. Compensation: Metabolic
Слайд 6METABOLIC ALKALOSIS
CAUSES:
• Vomiting: Lose enough stomach acid to produce alkalosis.
• Diuretics: Loop diuretics and
METABOLIC ALKALOSIS
CAUSES:
• Vomiting: Lose enough stomach acid to produce alkalosis.
• Diuretics: Loop diuretics and
Слайд 7RESPIRATORY ACIDOSIS:
causes:
CNS DEPRESSION
DRUGS:Opiates,sedatives,anaesthetics
OBESITY HYPOVENTILATION SYNDROME
STROKE
NEUROMUSCULAR DISORDERS:
NEUROLOGIC: POLIO,GBS,TETANUS,BOTULISM
MUSCULAR DYSTROPHY
AIRWAY OBSTRUCTION
ACUTE
RESPIRATORY ACIDOSIS:
causes:
CNS DEPRESSION
DRUGS:Opiates,sedatives,anaesthetics
OBESITY HYPOVENTILATION SYNDROME
STROKE
NEUROMUSCULAR DISORDERS:
NEUROLOGIC: POLIO,GBS,TETANUS,BOTULISM
MUSCULAR DYSTROPHY
AIRWAY OBSTRUCTION
ACUTE
Слайд 8RESPIRATORY ALKALOSIS
Causes:
High altitude.
Neuromuscular disease
Respiratory center depression
Inadequate mechanical ventilation
Sepsis
Burns
RESPIRATORY ALKALOSIS
Causes:
High altitude.
Neuromuscular disease
Respiratory center depression
Inadequate mechanical ventilation
Sepsis
Burns
Слайд 9Metabolic acidosis
Metabolic acidosis: Is caused by a decrease in HCO3- concentration in blood.
Causes:
Increased production
Metabolic acidosis
Metabolic acidosis: Is caused by a decrease in HCO3- concentration in blood.
Causes:
Increased production
Слайд 10Compensation of Metabolic acidosis:
Respiratory compensation: decrease in pH stimulates respiratory center causing hyperventilation which
Compensation of Metabolic acidosis:
Respiratory compensation: decrease in pH stimulates respiratory center causing hyperventilation which


Слайд 13Metabolic alkalosis
Metabolic alkalosis
Слайд 14Metabolic acidosis
Metabolic acidosis
Слайд 15Respiratory acidosis
Respiratory acidosis
Слайд 16Respiratory Alkalosis
Respiratory Alkalosis

Слайд 17Metabolic Acidosis
pH 7.30
PaCO2 40
HCO3 15
Metabolic Acidosis
pH 7.30
PaCO2 40
HCO3 15
Слайд 18Metabolic Alkalosis
pH 7.50
PCO2 40
HCO3 30
Metabolic Alkalosis
pH 7.50
PCO2 40
HCO3 30
Слайд 19Respiratory Acidosis
pH 7.30
PaCO2 60
HCO3 26
Respiratory Acidosis
pH 7.30
PaCO2 60
HCO3 26
Слайд 20Respiratory Alkalosis
pH 7.50
PaCO2 25
HCO3 23
Respiratory Alkalosis
pH 7.50
PaCO2 25
HCO3 23
Слайд 21What are the compensations?
• Respiratory acidosis --metabolic alkalosis
• Respiratory alkalosis --metabolic acidosis
• In respiratory conditions,
What are the compensations?
• Respiratory acidosis --metabolic alkalosis
• Respiratory alkalosis --metabolic acidosis
• In respiratory conditions,
Слайд 22Buffers kick in within minutes.
Respiratory compensation is rapid and starts within minutes
Buffers kick in within minutes.
Respiratory compensation is rapid and starts within minutes
Слайд 23Acid base disorder-worksheet
Acid base disorder-worksheet
Слайд 24Acid base disorder-worksheet
Practice ABG’s
Acid base disorder-worksheet
Practice ABG’s
Слайд 25Answers:
1. Respiratory alkalosis
2. Respiratory acidosis
3. Metabolic acidosis 4.Compensated
Respiratory
acidosis
5. Metabolic alkalosis
6. Compensated Respiratory
Answers:
1. Respiratory alkalosis
2. Respiratory acidosis
3. Metabolic acidosis 4.Compensated
Respiratory
acidosis
5. Metabolic alkalosis
6. Compensated Respiratory
Слайд 26STEPS OF ASSESSING ABG
STEP 1: Diagnose whether it is acidosis or alkalosis-
STEPS OF ASSESSING ABG
STEP 1: Diagnose whether it is acidosis or alkalosis-
Слайд 27Work sheet
Diarrhea may lead to----------?
Acid loss due to vomiting and gastric
suction may
Work sheet
Diarrhea may lead to----------?
Acid loss due to vomiting and gastric
suction may

Слайд 28Problem#1
67 year female known diabetic for past 20years presented with sudden onset
Problem#1
67 year female known diabetic for past 20years presented with sudden onset
Слайд 29Problem #2
A 30-year old man with DM presents with polyuria, polydipsia, fever, cough,
Problem #2
A 30-year old man with DM presents with polyuria, polydipsia, fever, cough,
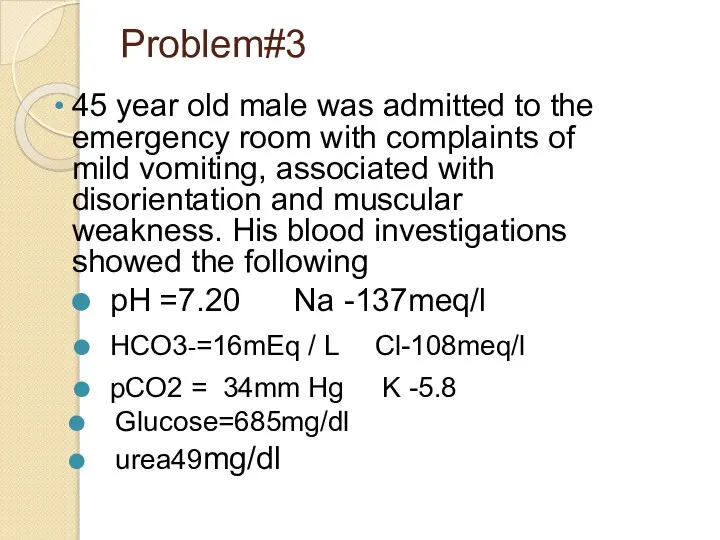
Слайд 30Problem#3
45 year old male was admitted to the emergency room with complaints
Problem#3
45 year old male was admitted to the emergency room with complaints
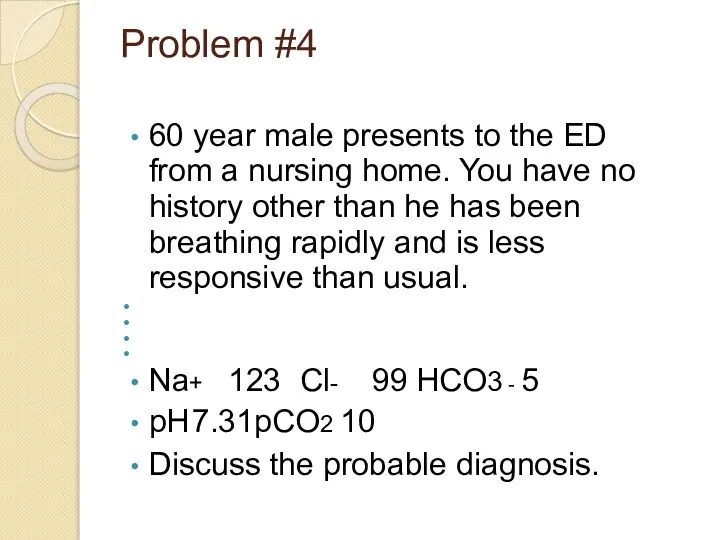
Слайд 31Problem #4
60 year male presents to the ED from a nursing home.
Problem #4
60 year male presents to the ED from a nursing home.
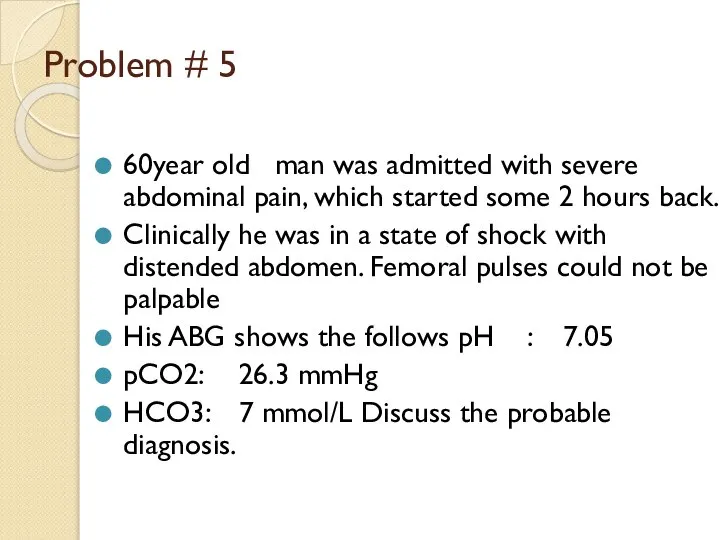
Слайд 32Problem # 5
60year old man was admitted with severe abdominal pain, which started
Problem # 5
60year old man was admitted with severe abdominal pain, which started
 Қабылдаудағы иллюзия және галлюцинациялар және олардың тұлға аралық коммуникацияға әсері
Қабылдаудағы иллюзия және галлюцинациялар және олардың тұлға аралық коммуникацияға әсері Легенькая
Легенькая Тромбоцитопения и тромбоцитопатия
Тромбоцитопения и тромбоцитопатия ВИЧ-инфекция у детей. I часть
ВИЧ-инфекция у детей. I часть Тактика ведения беременных с фетоплацентарной плацентарной недостаточностью: возможности и перспективы
Тактика ведения беременных с фетоплацентарной плацентарной недостаточностью: возможности и перспективы Как медицина относится к диетам
Как медицина относится к диетам Опухоли кроветворной и лимфоидной тканей
Опухоли кроветворной и лимфоидной тканей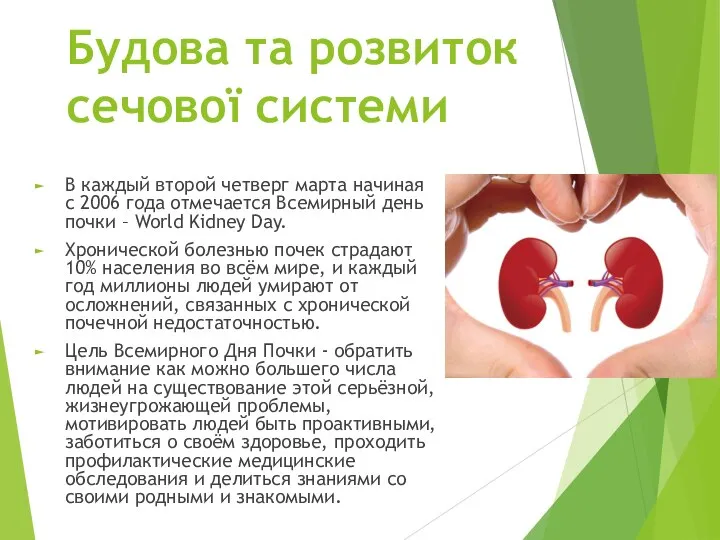 № 1-2-4 леч Будова та розвиток сечової системи
№ 1-2-4 леч Будова та розвиток сечової системи Мышцы, фасции, топография плеча, предплечья. Кафедра анатомии человека
Мышцы, фасции, топография плеча, предплечья. Кафедра анатомии человека Біздің елдегі дәлелді медицина орталыктары
Біздің елдегі дәлелді медицина орталыктары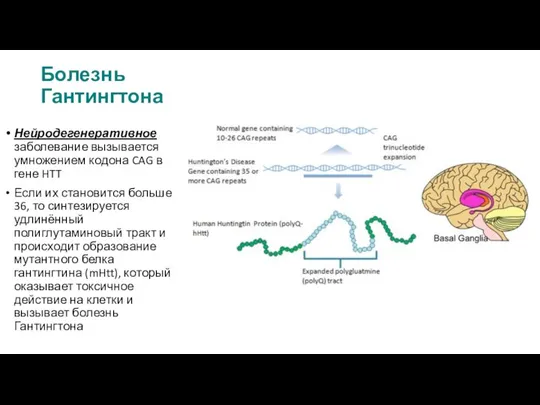 Болезнь Гантингтона
Болезнь Гантингтона Ведение пациента в интраоперационном и после-операционном периодах
Ведение пациента в интраоперационном и после-операционном периодах Нормативное и правовое регулирование обеспечения санитарно-эпидемиологического благополучия населения
Нормативное и правовое регулирование обеспечения санитарно-эпидемиологического благополучия населения Основные закономерности фармакодинамики
Основные закономерности фармакодинамики Место войта-терапии в ранней реабилитации недоношенных новорожденных
Место войта-терапии в ранней реабилитации недоношенных новорожденных Захворювання гіпофізу
Захворювання гіпофізу Патологияда тұқым қуалаушылықтың ролі
Патологияда тұқым қуалаушылықтың ролі Эфферентные нервные волокна. Средства, влияющие на холинэргические синапсы Средства, стимулирующие холинэргические синапсы
Эфферентные нервные волокна. Средства, влияющие на холинэргические синапсы Средства, стимулирующие холинэргические синапсы Упражнения для формирования правильного носового дыхания при аденоидах
Упражнения для формирования правильного носового дыхания при аденоидах The treatment of disorders of calcium metabolism in children on the data of osteodensitometry
The treatment of disorders of calcium metabolism in children on the data of osteodensitometry Тромболитическая терапия в практике врача Скорой помощи
Тромболитическая терапия в практике врача Скорой помощи Беременная с желудочковой аритмией - еще одна проблема кардиолога
Беременная с желудочковой аритмией - еще одна проблема кардиолога Гастродуоденит. Классификация, диагностика, лечение
Гастродуоденит. Классификация, диагностика, лечение Генетика и онкология
Генетика и онкология Минимально инвазивная эзофагэктомия: беспристрастный разговор
Минимально инвазивная эзофагэктомия: беспристрастный разговор Клинический проект. Тромбоэмболия легочной артерии
Клинический проект. Тромбоэмболия легочной артерии Проблемы перегрузки железом
Проблемы перегрузки железом Дәріс неврологияға кіріспе. Пән және клиникалық неврология тарихы. Неврологиядағы дәлелдену медицинасы
Дәріс неврологияға кіріспе. Пән және клиникалық неврология тарихы. Неврологиядағы дәлелдену медицинасы