- DATA Program Diabetes Awareness, Training, and Action

Содержание
- 2. Supported by: Blue Cross and Blue Shield of North Carolina Foundation Collaborating Organizations: NC Department of
- 3. Introduction Thank you for being a participant in the DATA Program!! Your participation demonstrates your interest
- 4. Introduction continued… When a student with diabetes is part of the school system, the school staff
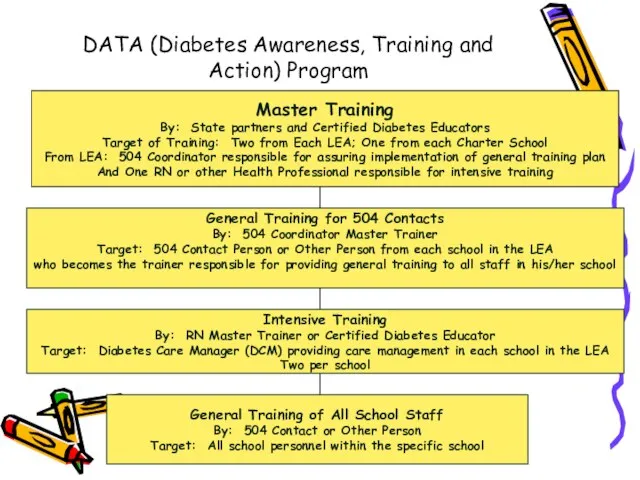
- 5. DATA (Diabetes Awareness, Training and Action) Program Master Training By: State partners and Certified Diabetes Educators
- 6. Part 1 Overview of SB 911 Care of School Children With Diabetes
- 7. Part 1: Overview of SB 911: Care of School Children with Diabetes Federal & State Support
- 8. Overview of SB 911 continued… State Board of Education Policy # 04A107 Special Health Care Services
- 9. Overview of SB 911 continued… The bill passed unanimously in the House and Senate in August,
- 10. Overview of SB 911 continued… Implications for NC Schools Guidelines adopted in every school in the
- 11. Overview of SB 911 continued… Section 1 of SB 911 Procedures for the development of a
- 12. Overview of SB 911 continued… Section 2 of SB 911 Local Boards of Education must ensure
- 13. Section 3 of SB 911 The NC State Board of Education delivered a progress report in
- 14. Overview of SB 911 continued… Please refer to your copy of the ADA Standards. An Individual
- 15. Overview of SB 911 continued… Children should have immediate access to diabetes supplies and diabetes treatments
- 16. G.S. 115C-375.3 April 28, 2005 House Bill 496 states that local boards of education shall ensure
- 17. Forms to Facilitate Implementation of the Law Diabetes Care Plan Request Diabetes Care Plan Responsibilities of
- 18. Role of the Master Trainer (One RN and One 504 Coordinator from each LEA) Participate in
- 19. Communication- Role of Nurse With student, parent & school staff SB-911 Diabetes School Act Provide forms
- 20. Communication With student and parent before school year begins By phone, meeting at the library, by
- 21. Communicate: Self Care Procedures done at school Equipment kept at school Diabetes care recommendations may change
- 22. Communicate: Parent Responsibilities Phone numbers Home, work, cell, pager Supplies Snacks School absences Care Plan request
- 23. Customize: Parent Request Form No MD signature required Request for Care Plan to be implemented Consent
- 24. Communicate: Parent Responsibilities Student, parent or 9-1-1 may have to assume responsibility for diabetes care until
- 25. Role of the DCM Diabetes Care Managers in Each School Participate in the Intensive training session.
- 26. DCM Roles continued… Communicate with teachers/substitute teachers/student/parents/health care team as indicated or as necessary. Assist the
- 27. Role of the 504 Contact in Each School Attend general information session instructed by the 504
- 28. Guidelines for PE Teacher and Coach Encourage exercise and participation in sports and physical activities for
- 29. Guidelines for Bus Drivers At the beginning of the school year, identify any students on the
- 30. Actions for Food Service Staff or Lunchroom Monitor Provide a lunch menu and lunch schedule in
- 31. Role of School Administration Work with the LEA Master Trainers to identify at least 2 school
- 32. Role of School Administration continued… Notify the Master Trainers for the school when such turnovers occur
- 33. Liability Concerns and Issues for DCMs How do I prevent liability situations from occurring? Be very
- 34. Liability Concerns and Issues Remember, a vial of insulin kept at room temperature is discarded 30
- 35. Liability Concerns and Issues continued… What happens if there is an occurrence? Most incidents occur when
- 36. Liability Concerns and Issues continued… If you give too much insulin Notify the student’s health care
- 37. Liability Concerns and Issues continued… If you give too little insulin, an additional shot can be
- 38. Liability Concerns and Issues continued… But how am I protected from litigation? The State of NC
- 39. Liability Concerns and Issues continued… Do I have any other protections? NC General Statute 90-21.14 adopted
- 40. Liability Concerns and Issues continued… So what needs to happen in my school? You as DCM,
- 41. Liability Concerns and Issues continued… So what about sharps, blood, carrying medication around the school? Self-monitoring
- 42. Continued Glucose Tabs are not medication. Some students with diabetes should be monitored at all times
- 43. Questions ??
- 44. Part 2: Diabetes Overview Diabetes Defined: “Diabetes Mellitus is a group of metabolic diseases characterized by
- 45. Diabetes Overview continued… Insulin is a hormone produced in the beta or islet cells of the
- 46. Diabetes Overview continued… Type 1: *Has been called Juvenile-Onset or Insulin Dependent Diabetes in the past.
- 47. Diabetes Overview continued… Type 2: * Has been called Adult-Onset or Non-Insulin-Dependent Diabetes. * Characterized by
- 48. Diabetes Overview continued… Insulin resistance means that insulin is produced, but the body is not using
- 49. Diabetes Overview continued… Reasons for Control: Diabetes is the 7th leading cause of death in the
- 50. Diabetes Overview continued… The goal of effective diabetes management is to control blood glucose levels by
- 51. Diabetes Overview continued… Diabetes management means monitoring or checking blood glucose levels throughout the day. Planning
- 52. Diabetes Overview continued… The Good News: The “Diabetes Control And Complications Trial” (DCCT) of 1993, clearly
- 53. Treatment Foundations: Type 1 diabetes: Occurs in approximately 1:400 children (10% of the diabetes population.) Often
- 54. Treatment Foundations: Currently, most students are taking insulin by syringe, pen device, or insulin pump. The
- 55. Treatment Foundations: The amount of insulin taken has to be balanced with food intake (specifically carbohydrates)
- 56. Treatment Foundations: Type 2 diabetes: Most often occurs in the adult population. Accounts for 90% of
- 57. Necessary Tools for Diabetes Management Self-Monitoring of Blood Sugar: Is important for anyone with diabetes. Currently
- 58. Necessary Tools continued… Blood Sugar Monitoring If you need to assist a child with blood sugar
- 59. Blood Sugar Monitoring continued… Prick the fleshy part on the side of the fingertip (may use
- 60. Blood Sugar Monitoring continued… If the school has a meter that is kept in the office
- 61. Necessary Tools continued… Carbohydrate Counting and the Meal Plan Students with Type 1 diabetes may practice
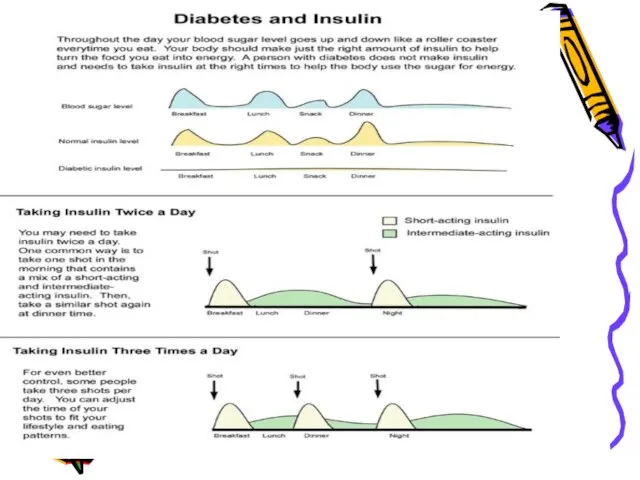
- 63. Insulin Action and Administration Most students take at least two injections of insulin a day. Some
- 64. What is an insulin pump? A battery operated device about the size of a pager
- 65. Insulin Action Insulin types are categorized as rapid-acting, fast-acting, intermediate-acting, long-acting or basal. Each type has
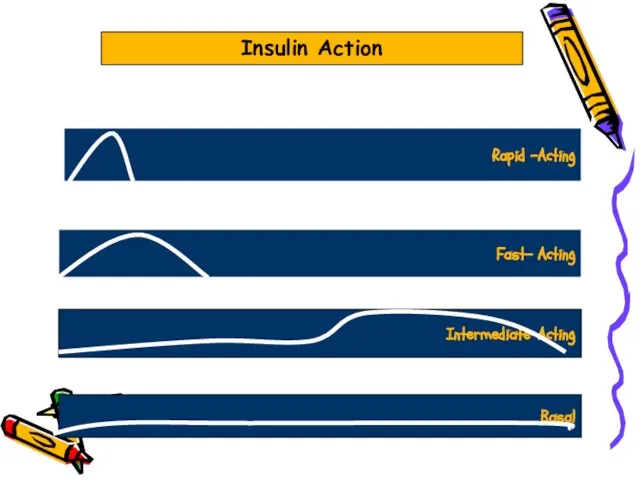
- 66. Rapid -Acting Fast- Acting Intermediate-Acting Basal Insulin Action
- 67. Insulin Administration After carefully drawing up the correct amount of insulin, cleanse the injection site with
- 68. Insulin Administration-Continued After pushing the plunger on the syringe, count slowly to five and remove the
- 69. Carb Counting, Insulin to Carb Ratios Many students are now using an algorithm instead of a
- 70. Insulin to Carb Ratio In an effort to match insulin to carbohydrate eaten, an insulin to
- 71. Combining the Two In order to correctly determine the amount of insulin needed before a meal,
- 72. Insulin to Carb Ratios and the Insulin Pump Most insulin pumps today are far more sophisticated
- 73. Oral Meds for Kids With Type 2 Diabetes The preferred method of treating Type 2 diabetes
- 74. Oral Meds The most frequently used medication for increasing insulin sensitivity in Type 2 diabetes in
- 75. Oral Meds It is important to note that some kids with Type 2 diabetes may at
- 76. Part 3 Acute Complications of Diabetes Hyperglycemia (High Blood Sugar) Hypoglycemia (Low Blood Sugar)
- 77. High Blood Sugar “Hyperglycemia”
- 78. Hyperglycemia High blood glucose (hyperglycemia) occurs when the body gets too little insulin, too much food,
- 79. Definition: High Blood Sugar Target Blood Sugar 6-12 years: 80-160 mg/dL pre-meal and bedtime >12 years:
- 80. Definition: High Blood Sugar Most health professionals view a blood sugar greater than 240 as “hyperglycemia.”
- 81. Signs & Symptoms of Hyperglycemia Frequent Urination Extreme Hunger Extreme Fatigue Unusual Thirst Irritability Blurred Vision
- 82. High Blood Sugar “Hyperglycemia” For the school age child, a blood sugar greater than 240 mg/dL
- 83. Ketostix® Directions must be followed exactly. Dip reagent end of strip in FRESH urine and remove
- 84. If a student’s ketone level is greater than “trace” but less than “large”, refer to that
- 85. In the event of moderate to large ketones, treat as an emergency situation according to the
- 86. In all cases of high blood sugar, if the student is able, he should drink calorie-free,
- 87. Diabetic Ketoacidosis-DKA If untreated over a period of time, high blood sugar can cause a serious
- 88. Diabetic Ketoacidosis For students using insulin infusion pumps, lack of insulin supply may lead to DKA
- 89. Diabetic Ketoacidosis Ketones in the bloodstream cause the pH of the blood and body fluids to
- 90. Any Questions???
- 91. Low Blood Sugar “Hypoglycemia”
- 92. What Is Hypoglycemia or Low Blood Sugar? Sometimes called an insulin reaction Occurs when blood sugar
- 93. Lows happen when insulin and blood sugar are out of balance. People without diabetes do not
- 94. Low blood glucose levels, which can be life-threatening, present the greatest immediate danger to people with
- 95. Signs and Symptoms of Low Blood Sugar Hunger Shakiness Dizziness Sweatiness Fast heartbeat Drowsiness Feeling irritable,
- 96. More Signs and Symptoms of Low Blood Sugars Feeling sleepy Being stubborn Lack of coordination Tingling
- 97. Recognizing Low Blood Sugar It is important to recognize a low blood sugar as soon as
- 98. Frequent Causes of Low Blood Sugar Meals that are late or missed Extra exercise or activity
- 99. What To Do When Hypoglycemia Occurs If possible always do a blood sugar check first. If
- 100. Hypoglycemia Busters 2-4 glucose tablets 4 ounces of apple or orange juice 4-6 ounces of regular
- 101. Catch Low Blood Sugar Early Be alert for any symptoms and times when a low blood
- 102. Treating Severe Hypoglycemia When severe hypoglycemia occurs, not enough sugar is in the brain. The student
- 103. What Happens when the Child is Unconscious? Drinking soda or eating glucose tablets is not possible
- 104. Using Glucagon Glucagon should be administered promptly if the person is unable to swallow, loses consciousness
- 105. In order for school staff to use Glucagon, orders for its use must be included on
- 107. Скачать презентацию
Слайд 2Supported by:
Blue Cross and Blue Shield of North Carolina Foundation
Collaborating Organizations:
NC Department
Supported by:
Blue Cross and Blue Shield of North Carolina Foundation
Collaborating Organizations:
NC Department

Слайд 3Introduction
Thank you for being a participant in the DATA Program!! Your participation
Introduction
Thank you for being a participant in the DATA Program!! Your participation
Слайд 4Introduction continued…
When a student with diabetes is part of the school system,
Introduction continued…
When a student with diabetes is part of the school system,
Слайд 5DATA (Diabetes Awareness, Training and Action) Program
Master Training
By: State partners and Certified
DATA (Diabetes Awareness, Training and Action) Program
Master Training
By: State partners and Certified
Слайд 6Part 1
Overview of SB 911
Care of School Children With Diabetes
Part 1
Overview of SB 911
Care of School Children With Diabetes
Слайд 7Part 1: Overview of SB 911: Care of School Children with Diabetes
Federal
Part 1: Overview of SB 911: Care of School Children with Diabetes
Federal
Слайд 8Overview of SB 911 continued…
State Board of Education Policy # 04A107 Special
Overview of SB 911 continued…
State Board of Education Policy # 04A107 Special
Слайд 9Overview of SB 911 continued…
The bill passed unanimously in the House and
Overview of SB 911 continued…
The bill passed unanimously in the House and
Слайд 10Overview of SB 911 continued…
Implications for NC Schools
Guidelines adopted in every school
Overview of SB 911 continued…
Implications for NC Schools
Guidelines adopted in every school
Слайд 11Overview of SB 911 continued…
Section 1 of SB 911
Procedures for the development
Overview of SB 911 continued…
Section 1 of SB 911
Procedures for the development
Слайд 12Overview of SB 911 continued…
Section 2 of SB 911
Local Boards of Education
Overview of SB 911 continued…
Section 2 of SB 911
Local Boards of Education
Слайд 13Section 3 of SB 911
The NC State Board of Education delivered a
The NC State Board of Education delivered a
Слайд 14Overview of SB 911 continued…
Please refer to your copy of the ADA
Overview of SB 911 continued…
Please refer to your copy of the ADA
Слайд 15Overview of SB 911 continued…
Children should have immediate access to diabetes supplies
Overview of SB 911 continued…
Children should have immediate access to diabetes supplies
Слайд 16G.S. 115C-375.3
April 28, 2005
House Bill 496 states that local boards of education
G.S. 115C-375.3
April 28, 2005
House Bill 496 states that local boards of education
Слайд 17Forms to Facilitate Implementation of the Law
Diabetes Care Plan Request
Diabetes Care Plan
Forms to Facilitate Implementation of the Law
Diabetes Care Plan Request
Diabetes Care Plan
Слайд 18Role of the Master Trainer
(One RN and One 504 Coordinator from each
Role of the Master Trainer (One RN and One 504 Coordinator from each
Слайд 19Communication- Role of Nurse
With student, parent & school staff
SB-911 Diabetes School Act
Provide
Communication- Role of Nurse
With student, parent & school staff
SB-911 Diabetes School Act
Provide
Слайд 20Communication
With student and parent before school year begins
By phone, meeting at the
Communication
With student and parent before school year begins
By phone, meeting at the
Слайд 21Communicate: Self Care
Procedures done at school
Equipment kept at school
Diabetes care recommendations may
Communicate: Self Care
Procedures done at school
Equipment kept at school
Diabetes care recommendations may
Слайд 22Communicate: Parent Responsibilities
Phone numbers
Home, work, cell, pager
Supplies
Snacks
School absences
Care Plan request
Care Plan
Student’s self-care
Communicate: Parent Responsibilities
Phone numbers
Home, work, cell, pager
Supplies
Snacks
School absences
Care Plan request
Care Plan
Student’s self-care
Слайд 23Customize: Parent Request Form
No MD signature required
Request for Care Plan to
Customize: Parent Request Form
No MD signature required
Request for Care Plan to
Слайд 24 Communicate: Parent Responsibilities
Student, parent or 9-1-1 may have to assume responsibility
Communicate: Parent Responsibilities
Student, parent or 9-1-1 may have to assume responsibility
Слайд 25Role of the DCM
Diabetes Care Managers in Each School
Participate in the Intensive
Role of the DCM
Diabetes Care Managers in Each School
Participate in the Intensive
Слайд 26DCM Roles continued…
Communicate with teachers/substitute teachers/student/parents/health care team as indicated or as
DCM Roles continued…
Communicate with teachers/substitute teachers/student/parents/health care team as indicated or as
Слайд 27Role of the 504 Contact in Each School
Attend general information session instructed
Role of the 504 Contact in Each School
Attend general information session instructed
Слайд 28Guidelines for PE Teacher and Coach
Encourage exercise and participation in sports and
Guidelines for PE Teacher and Coach
Encourage exercise and participation in sports and
Слайд 29Guidelines for Bus Drivers
At the beginning of the school year, identify any
Guidelines for Bus Drivers
At the beginning of the school year, identify any
Слайд 30Actions for Food Service Staff or Lunchroom Monitor
Provide a lunch menu and
Actions for Food Service Staff or Lunchroom Monitor
Provide a lunch menu and
Слайд 31Role of School Administration
Work with the LEA Master Trainers to identify at
Role of School Administration
Work with the LEA Master Trainers to identify at
Слайд 32Role of School Administration continued…
Notify the Master Trainers for the school when
Role of School Administration continued…
Notify the Master Trainers for the school when
Слайд 33Liability Concerns and Issues
for DCMs
How do I prevent liability situations from occurring?
Be
Liability Concerns and Issues
for DCMs
How do I prevent liability situations from occurring?
Be
Слайд 34Liability Concerns and Issues
Remember, a vial of insulin kept at room temperature
Liability Concerns and Issues
Remember, a vial of insulin kept at room temperature
Слайд 35Liability Concerns and Issues continued…
What happens if there is an occurrence?
Most incidents
Liability Concerns and Issues continued…
What happens if there is an occurrence?
Most incidents
Слайд 36Liability Concerns and Issues continued…
If you give too much insulin
Notify the student’s
Liability Concerns and Issues continued…
If you give too much insulin
Notify the student’s
Слайд 37Liability Concerns and Issues continued…
If you give too little insulin, an additional
Liability Concerns and Issues continued…
If you give too little insulin, an additional
Слайд 38Liability Concerns and Issues continued…
But how am I protected from litigation?
The State
Liability Concerns and Issues continued…
But how am I protected from litigation?
The State
Слайд 39Liability Concerns and Issues continued…
Do I have any other protections?
NC General Statute
Liability Concerns and Issues continued…
Do I have any other protections?
NC General Statute
Слайд 40Liability Concerns and Issues continued…
So what needs to happen in my school?
You
Liability Concerns and Issues continued…
So what needs to happen in my school?
You
Слайд 41Liability Concerns and Issues continued…
So what about sharps, blood, carrying medication around
Liability Concerns and Issues continued…
So what about sharps, blood, carrying medication around
Слайд 42Continued
Glucose Tabs are not medication.
Some students with diabetes should be monitored at
Continued
Glucose Tabs are not medication.
Some students with diabetes should be monitored at
Слайд 43Questions ??
Questions ??

Слайд 44Part 2: Diabetes Overview
Diabetes Defined:
“Diabetes Mellitus is a group of
Part 2: Diabetes Overview
Diabetes Defined:
“Diabetes Mellitus is a group of
Слайд 45Diabetes Overview continued…
Insulin is a hormone produced in the beta or islet
Diabetes Overview continued…
Insulin is a hormone produced in the beta or islet
Слайд 46Diabetes Overview continued…
Type 1:
*Has been called Juvenile-Onset or Insulin Dependent Diabetes
Diabetes Overview continued…
Type 1:
*Has been called Juvenile-Onset or Insulin Dependent Diabetes
Слайд 47Diabetes Overview continued…
Type 2:
* Has been called Adult-Onset or Non-Insulin-Dependent Diabetes.
*
Diabetes Overview continued…
Type 2:
* Has been called Adult-Onset or Non-Insulin-Dependent Diabetes.
*
Слайд 48Diabetes Overview continued…
Insulin resistance means that insulin is produced, but the body
Diabetes Overview continued…
Insulin resistance means that insulin is produced, but the body
Слайд 49Diabetes Overview continued…
Reasons for Control:
Diabetes is
the 7th leading cause of death
Diabetes Overview continued…
Reasons for Control:
Diabetes is
the 7th leading cause of death
Слайд 50Diabetes Overview continued…
The goal of effective diabetes management is to control blood
Diabetes Overview continued…
The goal of effective diabetes management is to control blood
Слайд 51Diabetes Overview continued…
Diabetes management means monitoring or checking blood glucose levels throughout
Diabetes Overview continued…
Diabetes management means monitoring or checking blood glucose levels throughout
Слайд 52Diabetes Overview continued…
The Good News:
The “Diabetes Control
And Complications Trial”
(DCCT) of 1993, clearly
demonstrated
Diabetes Overview continued…
The Good News:
The “Diabetes Control
And Complications Trial”
(DCCT) of 1993, clearly
demonstrated
Слайд 53Treatment Foundations:
Type 1 diabetes:
Occurs in approximately 1:400 children (10% of the
Treatment Foundations:
Type 1 diabetes:
Occurs in approximately 1:400 children (10% of the
Слайд 54Treatment Foundations:
Currently, most students are taking insulin by syringe, pen device, or
Treatment Foundations:
Currently, most students are taking insulin by syringe, pen device, or
Слайд 55
Treatment Foundations:
The amount of insulin taken has to be balanced with food
Treatment Foundations:
The amount of insulin taken has to be balanced with food
Слайд 56Treatment Foundations:
Type 2 diabetes:
Most often occurs in the adult population.
Accounts for
Treatment Foundations:
Type 2 diabetes:
Most often occurs in the adult population.
Accounts for
Слайд 57Necessary Tools for Diabetes Management
Self-Monitoring of Blood Sugar:
Is important for anyone with
Necessary Tools for Diabetes Management
Self-Monitoring of Blood Sugar:
Is important for anyone with
Слайд 58Necessary Tools continued…
Blood Sugar Monitoring
If you need to assist a child with
Necessary Tools continued…
Blood Sugar Monitoring
If you need to assist a child with
Слайд 59Blood Sugar Monitoring continued…
Prick the fleshy part on the side of the
Blood Sugar Monitoring continued…
Prick the fleshy part on the side of the
Слайд 60Blood Sugar Monitoring continued…
If the school has a meter that is kept
Blood Sugar Monitoring continued…
If the school has a meter that is kept
Слайд 61Necessary Tools continued…
Carbohydrate Counting and the Meal Plan
Students with Type 1 diabetes
Necessary Tools continued…
Carbohydrate Counting and the Meal Plan
Students with Type 1 diabetes
Слайд 63Insulin Action and Administration
Most students take at least two injections of insulin
Insulin Action and Administration
Most students take at least two injections of insulin
Слайд 64What is an insulin pump?
A battery operated device about the size of
What is an insulin pump?
A battery operated device about the size of
Слайд 65Insulin Action
Insulin types are categorized as rapid-acting, fast-acting, intermediate-acting, long-acting or basal.
Each
Insulin Action
Insulin types are categorized as rapid-acting, fast-acting, intermediate-acting, long-acting or basal.
Each
Слайд 66Rapid -Acting
Fast- Acting
Intermediate-Acting
Basal
Insulin Action
Rapid -Acting
Fast- Acting
Intermediate-Acting
Basal
Insulin Action
Слайд 67Insulin Administration
After carefully drawing up the correct amount of insulin, cleanse the
Insulin Administration
After carefully drawing up the correct amount of insulin, cleanse the
Слайд 68Insulin Administration-Continued
After pushing the plunger on the syringe, count slowly to five
Insulin Administration-Continued
After pushing the plunger on the syringe, count slowly to five
Слайд 69Carb Counting, Insulin to Carb Ratios
Many students are now using an algorithm
Carb Counting, Insulin to Carb Ratios
Many students are now using an algorithm
Слайд 70Insulin to Carb Ratio
In an effort to match insulin to carbohydrate eaten,
Insulin to Carb Ratio
In an effort to match insulin to carbohydrate eaten,
Слайд 71Combining the Two
In order to correctly determine the amount of insulin needed
Combining the Two
In order to correctly determine the amount of insulin needed
Слайд 72Insulin to Carb Ratios and the Insulin Pump
Most insulin pumps today are
Insulin to Carb Ratios and the Insulin Pump
Most insulin pumps today are
Слайд 73Oral Meds for Kids With Type 2 Diabetes
The preferred method of treating
Oral Meds for Kids With Type 2 Diabetes
The preferred method of treating
Слайд 74Oral Meds
The most frequently used medication for increasing insulin sensitivity in Type
Oral Meds
The most frequently used medication for increasing insulin sensitivity in Type
Слайд 75Oral Meds
It is important to note that some kids with Type 2
Oral Meds
It is important to note that some kids with Type 2
Слайд 76Part 3
Acute Complications of Diabetes
Hyperglycemia (High Blood
Sugar)
Hypoglycemia (Low Blood Sugar)
Part 3
Acute Complications of Diabetes
Hyperglycemia (High Blood
Sugar)
Hypoglycemia (Low Blood Sugar)
Слайд 77High Blood Sugar
“Hyperglycemia”
High Blood Sugar
“Hyperglycemia”
Слайд 78Hyperglycemia
High blood glucose (hyperglycemia) occurs when the body gets too little insulin,
Hyperglycemia
High blood glucose (hyperglycemia) occurs when the body gets too little insulin,
Слайд 79Definition: High Blood Sugar
Target Blood Sugar
<6 years: 100-160 mg/dL pre-meal and bedtime
6-12
Definition: High Blood Sugar
Target Blood Sugar
<6 years: 100-160 mg/dL pre-meal and bedtime
6-12
Слайд 80Definition: High Blood Sugar
Most health professionals view a blood sugar greater than
Definition: High Blood Sugar
Most health professionals view a blood sugar greater than
Слайд 81Signs & Symptoms of Hyperglycemia
Frequent Urination
Extreme Hunger
Extreme Fatigue
Unusual Thirst
Irritability
Blurred Vision
Signs & Symptoms of Hyperglycemia
Frequent Urination
Extreme Hunger
Extreme Fatigue
Unusual Thirst
Irritability
Blurred Vision
Слайд 82
High Blood Sugar
“Hyperglycemia”
For the school age child, a blood sugar
High Blood Sugar
“Hyperglycemia”
For the school age child, a blood sugar
Слайд 83Ketostix®
Directions must be followed exactly.
Dip reagent end of strip in FRESH urine
Ketostix®
Directions must be followed exactly.
Dip reagent end of strip in FRESH urine
Слайд 84If a student’s ketone level is greater than “trace” but less than
Слайд 85In the event of moderate to large ketones, treat as an emergency
In the event of moderate to large ketones, treat as an emergency
Слайд 86In all cases of high blood sugar, if the student is able,
In all cases of high blood sugar, if the student is able,
Слайд 87Diabetic Ketoacidosis-DKA
If untreated over a period of time, high blood sugar can
Diabetic Ketoacidosis-DKA
If untreated over a period of time, high blood sugar can
Слайд 88Diabetic Ketoacidosis
For students using insulin infusion pumps, lack of insulin supply may
Diabetic Ketoacidosis
For students using insulin infusion pumps, lack of insulin supply may
Слайд 89Diabetic Ketoacidosis
Ketones in the bloodstream cause the pH of the blood and
Diabetic Ketoacidosis
Ketones in the bloodstream cause the pH of the blood and
Слайд 90Any Questions???
Any Questions???
Слайд 91Low Blood Sugar
“Hypoglycemia”
Low Blood Sugar
“Hypoglycemia”
Слайд 92What Is Hypoglycemia or Low Blood Sugar?
Sometimes called an insulin reaction
Occurs when
What Is Hypoglycemia or Low Blood Sugar?
Sometimes called an insulin reaction
Occurs when
Слайд 93Lows happen when insulin and blood sugar are out of balance.
People without
Lows happen when insulin and blood sugar are out of balance.
People without
Слайд 94Low blood glucose levels, which can be life-threatening, present the greatest immediate
Low blood glucose levels, which can be life-threatening, present the greatest immediate
Слайд 95Signs and Symptoms of Low Blood Sugar
Hunger
Shakiness
Dizziness
Sweatiness
Fast heartbeat
Signs and Symptoms of Low Blood Sugar
Hunger
Shakiness
Dizziness
Sweatiness
Fast heartbeat
Слайд 96More Signs and Symptoms of Low Blood Sugars
Feeling sleepy
Being stubborn
Lack of coordination
Tingling
More Signs and Symptoms of Low Blood Sugars
Feeling sleepy
Being stubborn
Lack of coordination
Tingling
Слайд 97Recognizing Low Blood Sugar
It is important to recognize a low blood sugar
Recognizing Low Blood Sugar
It is important to recognize a low blood sugar
Слайд 98Frequent Causes of Low Blood Sugar
Meals that are late or missed
Extra exercise
Frequent Causes of Low Blood Sugar
Meals that are late or missed
Extra exercise
Слайд 99What To Do When Hypoglycemia Occurs
If possible always do a blood sugar
What To Do When Hypoglycemia Occurs
If possible always do a blood sugar
Слайд 100Hypoglycemia Busters
2-4 glucose tablets
4 ounces of apple or orange juice
4-6 ounces of
Hypoglycemia Busters
2-4 glucose tablets
4 ounces of apple or orange juice
4-6 ounces of
Слайд 101Catch Low Blood Sugar Early
Be alert for any symptoms and times when
Catch Low Blood Sugar Early
Be alert for any symptoms and times when
Слайд 102Treating Severe Hypoglycemia
When severe hypoglycemia occurs, not enough sugar is in the
Treating Severe Hypoglycemia
When severe hypoglycemia occurs, not enough sugar is in the
Слайд 103What Happens when the Child is Unconscious?
Drinking soda or eating glucose tablets
What Happens when the Child is Unconscious?
Drinking soda or eating glucose tablets
Слайд 104Using Glucagon
Glucagon should be administered promptly if the person is unable to
Using Glucagon
Glucagon should be administered promptly if the person is unable to
Слайд 105In order for school staff to use Glucagon, orders for its use
In order for school staff to use Glucagon, orders for its use
 Прямые антикоагулянты. Гепарин. Фармакокинетика. Механизм противосвертывающего действия. Особенности низкомолекулярных гепаринов
Прямые антикоагулянты. Гепарин. Фармакокинетика. Механизм противосвертывающего действия. Особенности низкомолекулярных гепаринов Тікелей емес немесе айнамен ларингоскопия
Тікелей емес немесе айнамен ларингоскопия Передняя ишемическая нейрооптикопатия
Передняя ишемическая нейрооптикопатия Что такое Большая перемена. Будь здоров!
Что такое Большая перемена. Будь здоров! Физиология крови
Физиология крови Кишечный шов. Виды, техника. Операция ушивания колотой и резанной раны кишки
Кишечный шов. Виды, техника. Операция ушивания колотой и резанной раны кишки Болезни системы крови
Болезни системы крови ВИЧ-инфицированные и заболевание СПИДом
ВИЧ-инфицированные и заболевание СПИДом Атомдық жарылыстың зардаптары
Атомдық жарылыстың зардаптары Особенности стоматологического статуса населения пожилого возраста
Особенности стоматологического статуса населения пожилого возраста Общие сведения о питании. Витамины
Общие сведения о питании. Витамины Методическая разработка раздела Соотношения между сторонами и углами треугольника
Методическая разработка раздела Соотношения между сторонами и углами треугольника Инвалидность в Норвегии
Инвалидность в Норвегии Ребенок с проблемами интеллектуального развития в семье
Ребенок с проблемами интеллектуального развития в семье Стенокардия. Первая помощь при приступе стенокардии
Стенокардия. Первая помощь при приступе стенокардии Do we need a vaccination against coronavirus
Do we need a vaccination against coronavirus Периоды новорожденности
Периоды новорожденности Обморочные и судорожные состояния
Обморочные и судорожные состояния Вступление к TCCC. Тактическая помощь пострадавшим в бою для медицинского персонала
Вступление к TCCC. Тактическая помощь пострадавшим в бою для медицинского персонала Оригинальные техники массажа с применением натуральных косметических средств в сфере салонного бизнеса
Оригинальные техники массажа с применением натуральных косметических средств в сфере салонного бизнеса К2Д3-Boost. Метаболизм кальция в организме
К2Д3-Boost. Метаболизм кальция в организме Омикрон – штамм короновируса: что надо знать
Омикрон – штамм короновируса: что надо знать Введение. История фармакологии. Общая фармакология
Введение. История фармакологии. Общая фармакология Клиническая ситуация
Клиническая ситуация Crimea state medical university
Crimea state medical university Профессия – «Врач»
Профессия – «Врач» Medical acadmy named after s.i.georgievsky of vernadsky cfu
Medical acadmy named after s.i.georgievsky of vernadsky cfu Результаты применения компьютерной и видео-цветоволновой ауторелаксации
Результаты применения компьютерной и видео-цветоволновой ауторелаксации