- Fat Embolism Syndrome

Содержание
- 2. History In 1861, Zenker described fat droplets in the lung capillaries of a railroad worker who
- 3. What is it ?? complex with potentially catastrophic cardiopulmonary and cerebral dysfunction Three problems : dyspnoea,
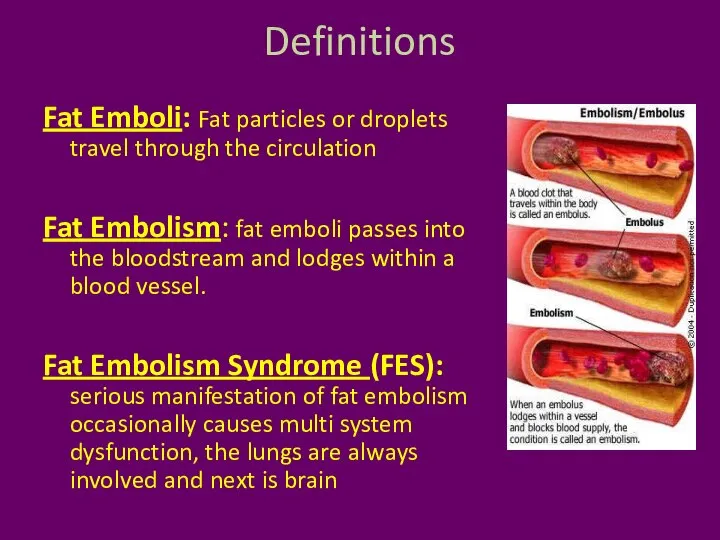
- 4. Definitions Fat Emboli: Fat particles or droplets travel through the circulation Fat Embolism: fat emboli passes
- 5. Fulminant fat embolism sudden intravascular liberation of a large amount of fat causing pulmonary vascular obstruction,
- 6. Etiology
- 7. Trauma related (95 %) Long bone fractures Pelvic fractures Fractures of other marrow-containing bones Orthopaedic procedures
- 8. Non-trauma related Pancreatitis Diabetes mellitus Osteomyelitis and panniculitis Bone tumour lysis Steroid therapy Sickle cell haemoglobinopathies
- 9. fat emboli also can arise from circulating lipoproteins
- 10. What is frequent ?? lower extremity and pelvic trauma, intramedullary nailing of long-bone fractures, hip arthroplasty,
- 11. Incidence ?? incidence of FES was 1 % But multiple fractures, adults, high velocity injuries, cementing,
- 12. Lethal dose The acute lethal dose of fat ranges from 20-50 ml. The volume of marrow
- 13. Pathophysiology ?? The Mechanical theory (Gauss) Biochemical theory (Lehmann and Moore) Coagulation theory
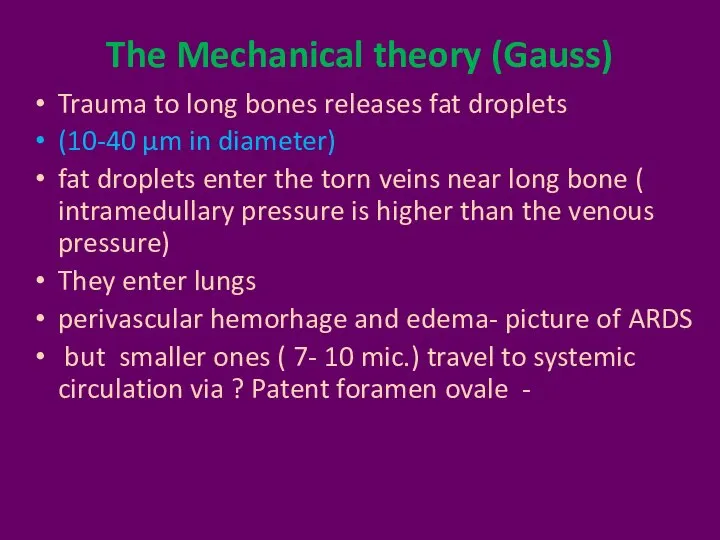
- 14. The Mechanical theory (Gauss) Trauma to long bones releases fat droplets (10-40 μm in diameter) fat
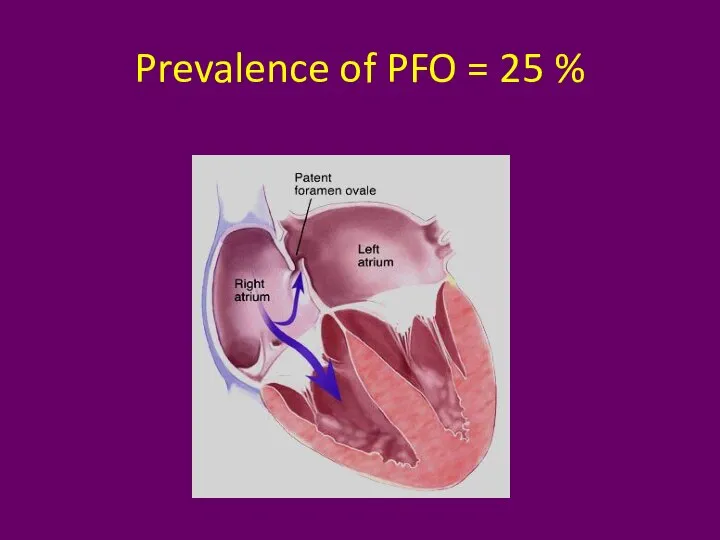
- 15. Prevalence of PFO = 25 %
- 16. Biochemical theory Embolized fat is degraded in plasma to free fatty acids. FFA can cause lung
- 17. Coagulation theory Tissue thromboplastin is released with marrow elements following long bone fractures. Activates intravascular coagulation
- 18. Can it happen in sickle cell disease ??
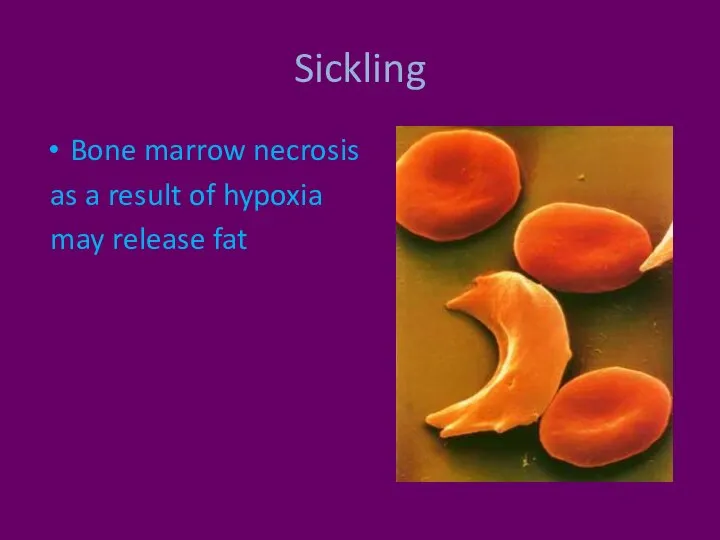
- 19. Sickling Bone marrow necrosis as a result of hypoxia may release fat
- 20. Number of theories means Poorly understood ??
- 21. Clinical Features 12-72 hrs after the initial injury Rarely two weeks
- 22. Features Respiratory changes – 95 % Cerebral changes – 60 % petechiae (33% - 60 %).
- 23. Respiratory changes Dyspnoea, tachypnoea and hypoxaemia are the most frequent early findings. Respiratory failure as ARDS
- 24. Cerebral The more common presentation is with an acute confusional state but focal neurological signs including
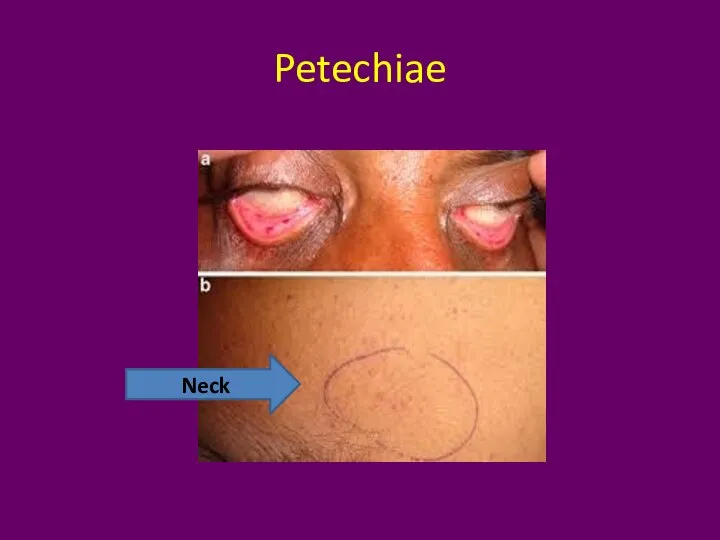
- 25. Petechiae Embolization of small dermal capillaries leading to extravasation of erythrocytes. This produces a petechial rash
- 26. Petechiae Neck
- 27. Petechiae Petechiae only rarely appear on the legs and they are never seen on the face
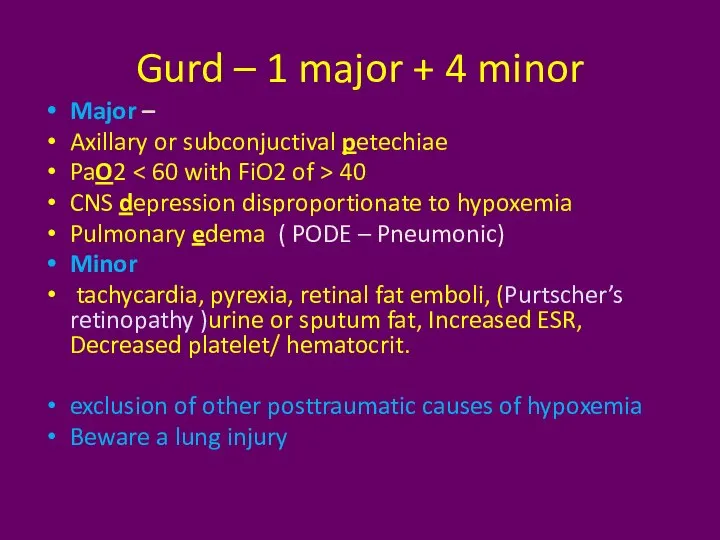
- 28. Gurd – 1 major + 4 minor Major – Axillary or subconjuctival petechiae PaO2 40 CNS
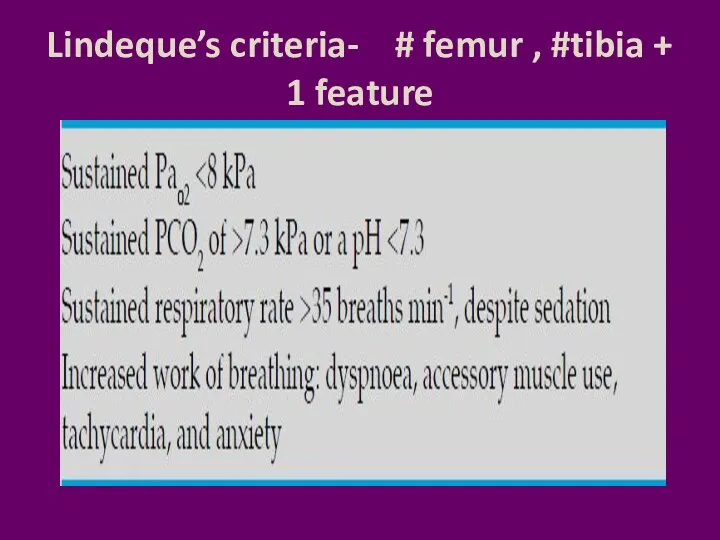
- 29. Lindeque’s criteria- # femur , #tibia + 1 feature
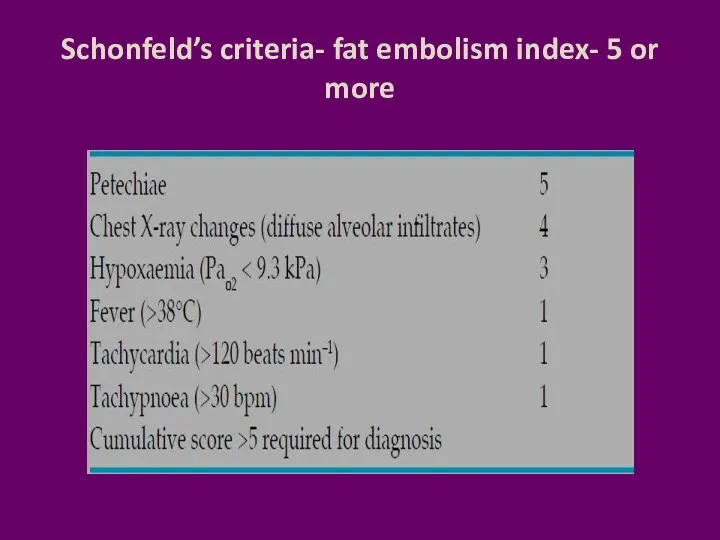
- 30. Schonfeld’s criteria- fat embolism index- 5 or more
- 31. The features are acute, but not abrupt
- 32. How to confirm ?? High index of suspicion and some investigations
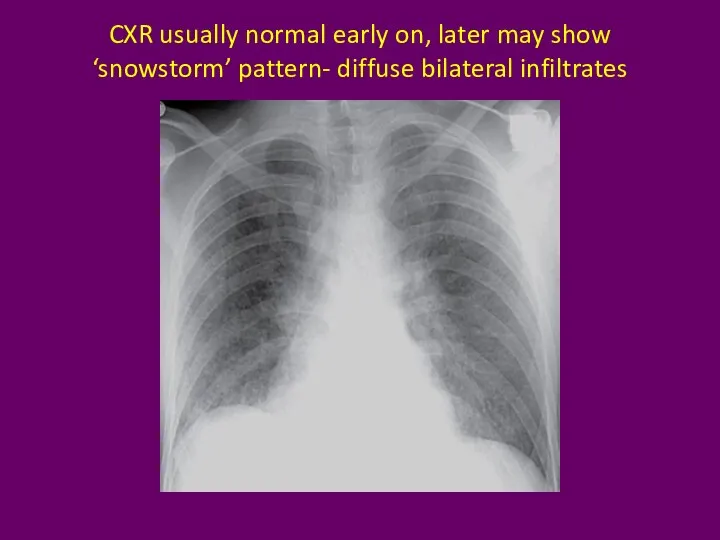
- 33. CXR usually normal early on, later may show ‘snowstorm’ pattern- diffuse bilateral infiltrates
- 34. Lab values Arterial blood gases : This reveals a low partial pressure of oxygen and a
- 35. CVS ECG : sinus tachycardia ; Non specific ST T changes, RBBB, Lung scan : ?
- 36. Broncho alveolar lavage BAL : fat droplets. The staining of cells with oil red O after
- 37. CT Brain White matter petechiae Cerebral edema Rarely cerebral atrophy due to full embolisation
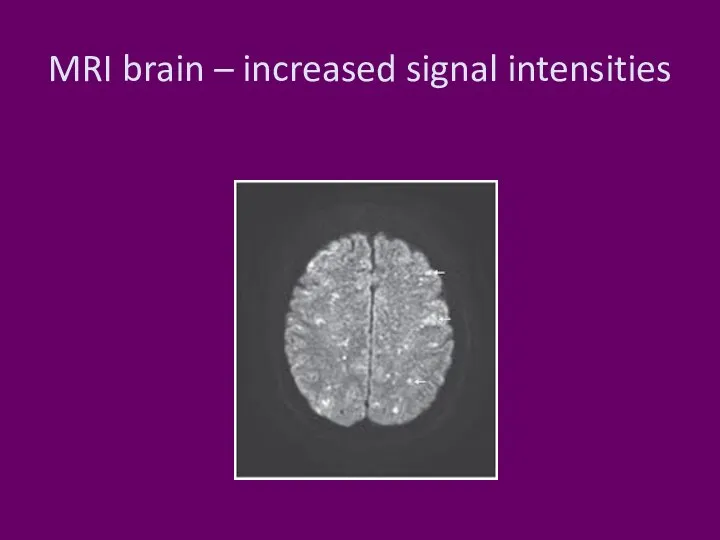
- 38. MRI brain – increased signal intensities
- 39. Treatment Prevention and supportive adequate oxygenation and ventilation, stable haemodynamics, blood products as clinically indicated, hydration,
- 40. Prevention Hole and drill the long bones Early immobilization of fractures Cementless prostheses or bone-vacuum cementing
- 41. Prevention during cementing Hydration Oxygenation No nitrous
- 42. Treatment Aspirin Heparin N acetyl cysteine Other speculated therapies such as glucose and insulin, alcohol infusion
- 43. Prognosis who survived The prognosis for patients who survive fat embolism is good, with recovery from
- 44. Summary Definitions Incidence Etiology lethal dose Theories Prevention Treatment
- 46. Скачать презентацию
Слайд 3What is it ??
complex with potentially catastrophic cardiopulmonary and cerebral dysfunction
Three
What is it ??
complex with potentially catastrophic cardiopulmonary and cerebral dysfunction
Three
Слайд 4Definitions
Fat Emboli: Fat particles or droplets travel through the circulation
Fat Embolism: fat
Definitions
Fat Emboli: Fat particles or droplets travel through the circulation
Fat Embolism: fat
Слайд 5Fulminant fat embolism
sudden intravascular liberation of a large amount of fat
Fulminant fat embolism
sudden intravascular liberation of a large amount of fat
Слайд 6Etiology
Etiology
Слайд 7Trauma related (95 %)
Long bone fractures
Pelvic fractures
Fractures of other marrow-containing bones
Orthopaedic
Trauma related (95 %)
Long bone fractures
Pelvic fractures
Fractures of other marrow-containing bones
Orthopaedic
Слайд 8
Non-trauma related
Pancreatitis
Diabetes mellitus
Osteomyelitis and panniculitis
Bone tumour lysis
Steroid therapy
Sickle cell haemoglobinopathies
Alcoholic (fatty) liver
Non-trauma related
Pancreatitis
Diabetes mellitus
Osteomyelitis and panniculitis
Bone tumour lysis
Steroid therapy
Sickle cell haemoglobinopathies
Alcoholic (fatty) liver
Слайд 9fat emboli also can arise from circulating lipoproteins
fat emboli also can arise from circulating lipoproteins
Слайд 10What is frequent ??
lower extremity and pelvic trauma,
intramedullary nailing of long-bone
What is frequent ??
lower extremity and pelvic trauma,
intramedullary nailing of long-bone
Слайд 11Incidence ??
incidence of FES was 1 %
But multiple fractures, adults, high
Incidence ??
incidence of FES was 1 %
But multiple fractures, adults, high
Слайд 12Lethal dose
The acute lethal dose of fat ranges from 20-50 ml.
Lethal dose
The acute lethal dose of fat ranges from 20-50 ml.
Слайд 13Pathophysiology ??
The Mechanical theory (Gauss)
Biochemical theory (Lehmann and Moore)
Coagulation theory
Pathophysiology ??
The Mechanical theory (Gauss)
Biochemical theory (Lehmann and Moore)
Coagulation theory
Слайд 14
The Mechanical theory (Gauss)
Trauma to long bones releases fat droplets
(10-40 μm in
The Mechanical theory (Gauss)
Trauma to long bones releases fat droplets
(10-40 μm in
Слайд 15Prevalence of PFO = 25 %
Prevalence of PFO = 25 %
Слайд 16Biochemical theory
Embolized fat is degraded in plasma to free fatty acids.
FFA
Biochemical theory
Embolized fat is degraded in plasma to free fatty acids.
FFA
Слайд 17Coagulation theory
Tissue thromboplastin is released with marrow elements following long bone
Coagulation theory
Tissue thromboplastin is released with marrow elements following long bone
Слайд 18Can it happen in sickle cell disease ??
Слайд 19Sickling
Bone marrow necrosis
as a result of hypoxia
may release fat
Sickling
Bone marrow necrosis
as a result of hypoxia
may release fat
Слайд 20Number of theories means
Poorly understood ??
Poorly understood ??
Слайд 21Clinical Features
12-72 hrs after the initial injury
Rarely two weeks
Clinical Features
12-72 hrs after the initial injury
Rarely two weeks
Слайд 22Features
Respiratory changes – 95 %
Cerebral changes – 60 %
petechiae
Features
Respiratory changes – 95 %
Cerebral changes – 60 %
petechiae
Слайд 23Respiratory changes
Dyspnoea, tachypnoea and hypoxaemia are the most frequent early findings.
Respiratory failure
Respiratory changes
Dyspnoea, tachypnoea and hypoxaemia are the most frequent early findings.
Respiratory failure
Слайд 24Cerebral
The more common presentation is with an acute confusional state
but
Cerebral
The more common presentation is with an acute confusional state
but
Слайд 25Petechiae
Embolization of small dermal capillaries leading to extravasation of erythrocytes. This
Petechiae
Embolization of small dermal capillaries leading to extravasation of erythrocytes. This
Слайд 26Petechiae
Neck
Petechiae
Neck
Слайд 27Petechiae
Petechiae only rarely appear on the legs and they are never seen
Petechiae
Petechiae only rarely appear on the legs and they are never seen
Слайд 28Gurd – 1 major + 4 minor
Major –
Axillary or subconjuctival petechiae
Gurd – 1 major + 4 minor
Major –
Axillary or subconjuctival petechiae
Слайд 29Lindeque’s criteria- # femur , #tibia + 1 feature
Lindeque’s criteria- # femur , #tibia + 1 feature
Слайд 30Schonfeld’s criteria- fat embolism index- 5 or more
Schonfeld’s criteria- fat embolism index- 5 or more
Слайд 31
The features are acute, but not abrupt
The features are acute, but not abrupt
Слайд 32How to confirm ??
High index of suspicion and some investigations
How to confirm ??
High index of suspicion and some investigations
Слайд 33CXR usually normal early on, later may show ‘snowstorm’ pattern- diffuse bilateral
CXR usually normal early on, later may show ‘snowstorm’ pattern- diffuse bilateral
Слайд 34Lab values
Arterial blood gases :
This reveals a low partial pressure
Lab values
Arterial blood gases :
This reveals a low partial pressure
Слайд 35CVS
ECG : sinus tachycardia ; Non specific ST T changes, RBBB,
CVS
ECG : sinus tachycardia ; Non specific ST T changes, RBBB,
Слайд 36Broncho alveolar lavage
BAL : fat droplets.
The staining of cells with
Broncho alveolar lavage
BAL : fat droplets.
The staining of cells with
Слайд 37CT Brain
White matter petechiae
Cerebral edema
Rarely cerebral atrophy due to
full embolisation
CT Brain
White matter petechiae
Cerebral edema
Rarely cerebral atrophy due to
full embolisation
Слайд 38MRI brain – increased signal intensities
MRI brain – increased signal intensities
Слайд 39Treatment
Prevention and supportive
adequate oxygenation and ventilation,
stable haemodynamics,
blood products as
Treatment
Prevention and supportive
adequate oxygenation and ventilation,
stable haemodynamics,
blood products as
Слайд 40Prevention
Hole and drill the long bones
Early immobilization of fractures
Cementless prostheses or
Prevention
Hole and drill the long bones
Early immobilization of fractures
Cementless prostheses or
Слайд 41Prevention
during cementing
Hydration
Oxygenation
No nitrous
Prevention
during cementing
Hydration
Oxygenation
No nitrous
Слайд 42Treatment
Aspirin
Heparin
N acetyl cysteine
Other speculated therapies such as glucose and insulin,
Treatment
Aspirin
Heparin
N acetyl cysteine
Other speculated therapies such as glucose and insulin,
Слайд 43Prognosis who survived
The prognosis for patients who survive fat embolism is
Prognosis who survived
The prognosis for patients who survive fat embolism is
Слайд 44Summary
Definitions
Incidence
Etiology
lethal dose
Theories
Prevention
Treatment
Summary
Definitions
Incidence
Etiology
lethal dose
Theories
Prevention
Treatment
 Вещества, действующие на мембрану клетки и клеточную стенку. Занятие 5
Вещества, действующие на мембрану клетки и клеточную стенку. Занятие 5 Главные заповеди здорового образа жизни
Главные заповеди здорового образа жизни Основы учения о лекарствах
Основы учения о лекарствах EMT-B / Combat Medic. Подготовка, специфика, протоколы
EMT-B / Combat Medic. Подготовка, специфика, протоколы ІХС: Інфаркт міокарда
ІХС: Інфаркт міокарда Презентация (2)
Презентация (2) Технологии развития артикуляционной моторики
Технологии развития артикуляционной моторики Терапиялық стоматология. Қайта минералдану терапияның әдістері және заттары
Терапиялық стоматология. Қайта минералдану терапияның әдістері және заттары UCSC Genome Browser
UCSC Genome Browser Седативные наркотические (успокаивающие) вещества
Седативные наркотические (успокаивающие) вещества Особенности анатомии и физиологии органов дыхания у детей
Особенности анатомии и физиологии органов дыхания у детей Вскармливание детей до 1 года. Грудное (естественное). Смешанное. Искусственное
Вскармливание детей до 1 года. Грудное (естественное). Смешанное. Искусственное Функциональная анатомия органа зрения
Функциональная анатомия органа зрения Панариций. Причины заболевания
Панариций. Причины заболевания Дети с РАС
Дети с РАС Показания к нанзначению корсета Шено
Показания к нанзначению корсета Шено Дермотологияда ГКС терапиясы
Дермотологияда ГКС терапиясы Анатомо-физиологические сведения о брюшине
Анатомо-физиологические сведения о брюшине Тактическая помощь пострадавшим в бою для медицинского персонала август 2018
Тактическая помощь пострадавшим в бою для медицинского персонала август 2018 Препарирование полостей II класса по Блеку
Препарирование полостей II класса по Блеку ЧМТ - черепно-мозговая травма
ЧМТ - черепно-мозговая травма Холодовая травма
Холодовая травма Влияние наркотиков на организм человека
Влияние наркотиков на организм человека Профилактика вторичного и рецидивного кариеса
Профилактика вторичного и рецидивного кариеса Заболевания органов выделительной системы
Заболевания органов выделительной системы Здоровье учителя. Школа выживания
Здоровье учителя. Школа выживания Ишемическая болезнь сердца
Ишемическая болезнь сердца Vegetarianism
Vegetarianism