Serum rantes, transforming growth factor-β1 and interleukin-6 fibrosis in patients with aortic valve stenosis
- Serum rantes, transforming growth factor-β1 and interleukin-6 fibrosis in patients with aortic valve stenosis

Содержание
- 2. INTRODUCTION Progressive aortic valve degeneration leads to severe aortic valve stenosis (AS) in approximately 2 –
- 3. Some postulated factors driving AS progession include influence of classic atherosclerotic risk factors. In AS, not
- 4. Myocardial fibrosis results from increased myofibroblast activity and excessive extracellular matrix deposition. Various cells and molecules
- 5. METHODS Study population Magnetic resonance imaging Inflammatory biomarkers Echocardiography Statistical analysis
- 6. Study population Forty consecutive patients with moderate (defined as an aortic valve area between 1.0 –
- 7. Magnetic resonance imaging LV end-diastolic volume and diameters, LV end-systolic volume and diameters, LV ejection fraction
- 8. Inflammatory biomarkers Fasting blood was drawn from an antecubital vein without tourniquet and placed in a
- 9. Echocardiography Comprehensive transthoracic echocardiography was performed in all patients after ≥30 minutes of rest by 2
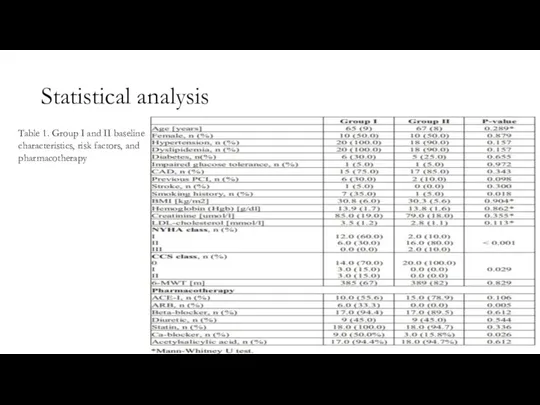
- 10. Statistical analysis Table 1. Group I and II baseline characteristics, risk factors, and pharmacotherapy
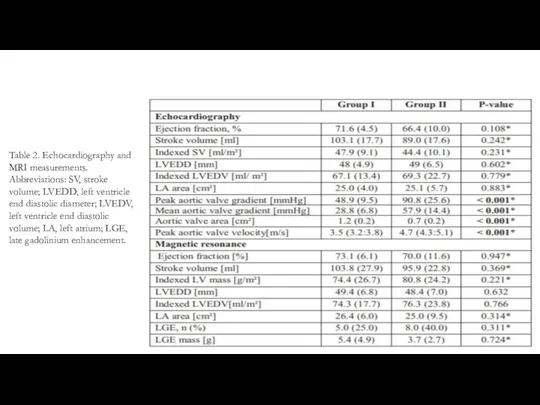
- 11. Table 2. Echocardiography and MRI measurements. Abbreviations: SV, stroke volume; LVEDD, left ventricle end diastolic diameter;
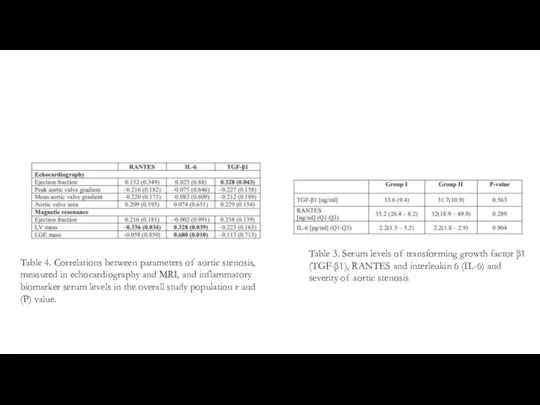
- 12. Table 3. Serum levels of transforming growth factor β1 (TGF-β1), RANTES and interleukin 6 (IL-6) and
- 13. RESULTS Group I included twenty patients with moderate AS while group II included twenty patients with
- 14. In previous studies, significant differences in serum levels of TGF-β1 were found in severe AS patients
- 15. Conclusions Although there is an increasing interest in the immunopathogenesis of AS, relatively little is known
- 17. Скачать презентацию
Слайд 2INTRODUCTION
Progressive aortic valve degeneration leads to severe aortic valve stenosis (AS) in
INTRODUCTION
Progressive aortic valve degeneration leads to severe aortic valve stenosis (AS) in
Слайд 3Some postulated factors driving AS progession include influence of classic atherosclerotic risk
Some postulated factors driving AS progession include influence of classic atherosclerotic risk
Слайд 4Myocardial fibrosis results from increased myofibroblast activity and excessive extracellular matrix deposition.
Myocardial fibrosis results from increased myofibroblast activity and excessive extracellular matrix deposition.
Слайд 5METHODS
Study population
Magnetic resonance imaging
Inflammatory biomarkers
Echocardiography
Statistical analysis
METHODS
Study population
Magnetic resonance imaging
Inflammatory biomarkers
Echocardiography
Statistical analysis

Слайд 6Study population
Forty consecutive patients with moderate (defined as an aortic valve area
Study population
Forty consecutive patients with moderate (defined as an aortic valve area
Слайд 7Magnetic resonance imaging
LV end-diastolic volume and diameters, LV end-systolic volume and diameters,
Magnetic resonance imaging
LV end-diastolic volume and diameters, LV end-systolic volume and diameters,
Слайд 8Inflammatory biomarkers
Fasting blood was drawn from an antecubital vein without tourniquet and
Inflammatory biomarkers
Fasting blood was drawn from an antecubital vein without tourniquet and
Слайд 9Echocardiography
Comprehensive transthoracic echocardiography was performed in all patients after ≥30 minutes of
Echocardiography
Comprehensive transthoracic echocardiography was performed in all patients after ≥30 minutes of
Слайд 10Statistical analysis
Table 1. Group I and II baseline characteristics, risk factors, and
Statistical analysis
Table 1. Group I and II baseline characteristics, risk factors, and
Слайд 11Table 2. Echocardiography and MRI measurements. Abbreviations: SV, stroke volume; LVEDD, left
Table 2. Echocardiography and MRI measurements. Abbreviations: SV, stroke volume; LVEDD, left
Слайд 12Table 3. Serum levels of transforming growth factor β1 (TGF-β1), RANTES and
Table 3. Serum levels of transforming growth factor β1 (TGF-β1), RANTES and
Слайд 13RESULTS
Group I included twenty patients with moderate AS while group II included
RESULTS
Group I included twenty patients with moderate AS while group II included
Слайд 14In previous studies, significant differences in serum levels of TGF-β1 were found
In previous studies, significant differences in serum levels of TGF-β1 were found
Слайд 15Conclusions
Although there is an increasing interest in the immunopathogenesis of AS, relatively
Conclusions
Although there is an increasing interest in the immunopathogenesis of AS, relatively
 Behandling av eksudativ AMD
Behandling av eksudativ AMD Боррелиозы. Диагностика
Боррелиозы. Диагностика Сестринская деятельность при циррозе печени в стационарных условиях
Сестринская деятельность при циррозе печени в стационарных условиях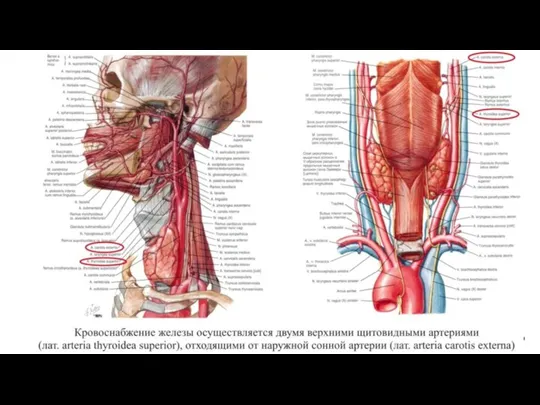 Кровоснабжение щитовидной железы
Кровоснабжение щитовидной железы Глинолечение
Глинолечение Инфекционные заболевания 21 века
Инфекционные заболевания 21 века Medical Biology
Medical Biology Оказание неотложной медицинской помощи пациентам с ОКС без подъема сегмента ST на догоспитальном этапе
Оказание неотложной медицинской помощи пациентам с ОКС без подъема сегмента ST на догоспитальном этапе Қатерлі лимфомалар. Ходжкиндік және Ходжкиндік емес лимфомалар
Қатерлі лимфомалар. Ходжкиндік және Ходжкиндік емес лимфомалар Хромосомные болезни
Хромосомные болезни Сыпи у детей (1)
Сыпи у детей (1) Манчестерская операция /Операция Дональда, усовершенствованная Фозергиллом
Манчестерская операция /Операция Дональда, усовершенствованная Фозергиллом Гликогенфосфорилазы
Гликогенфосфорилазы Центр по лечению ХСН, маршрутизация пациентов с ХСН
Центр по лечению ХСН, маршрутизация пациентов с ХСН Определение Гиперлипопротеинемий по Фридрексену
Определение Гиперлипопротеинемий по Фридрексену Предмет и задачи физиотерапии электролечение
Предмет и задачи физиотерапии электролечение Систолическое нарушение ритма
Систолическое нарушение ритма Депрескрайбинг. Практика снижения дозы и отмены лекарственных средств
Депрескрайбинг. Практика снижения дозы и отмены лекарственных средств Газоотведение. Введение свечей в прямую кишку
Газоотведение. Введение свечей в прямую кишку Клиническая гипнотерапия. Классический и эриксоновский гипноз. Гипноз и гипнотерапия в психотерапевтической работе
Клиническая гипнотерапия. Классический и эриксоновский гипноз. Гипноз и гипнотерапия в психотерапевтической работе Хронические гнойные заболевания уха отогенные внутричерепные осложнения. Лекция 2
Хронические гнойные заболевания уха отогенные внутричерепные осложнения. Лекция 2 Клинические случаи в детской стоматологии
Клинические случаи в детской стоматологии дисбиоз
дисбиоз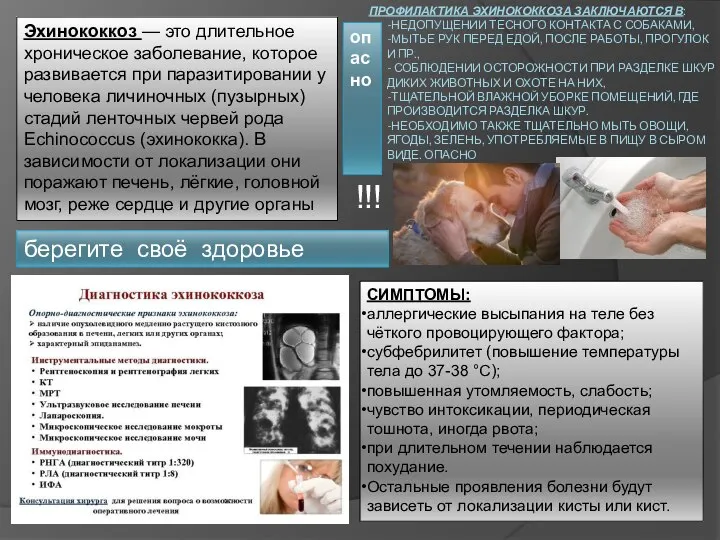 Эхинококкоз
Эхинококкоз Гематологические аспекты в морфологии
Гематологические аспекты в морфологии Рыночные механизмы в здравоохранении
Рыночные механизмы в здравоохранении Балаларда әртүрлі гингивит түрлерін емдеу әдістері
Балаларда әртүрлі гингивит түрлерін емдеу әдістері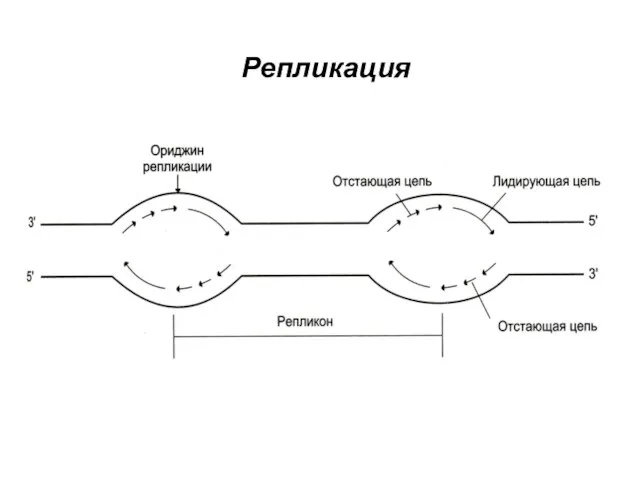 Репликация. Транскрипция
Репликация. Транскрипция