- Ventricular tachycardias in the absence of structural heart disease

Содержание
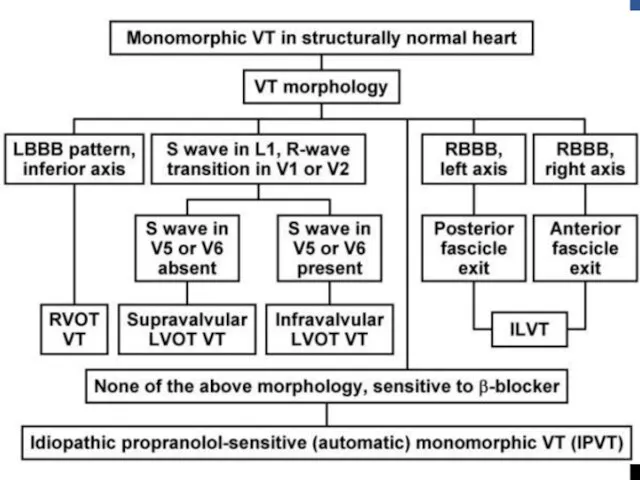
- 2. 10% of patients presenting with VT have no apparent structural heart disease VT in structurally normal
- 3. NON–LIFE-THREATENING (TYPICALLY MONOMORPHIC) Classified on basis of site of origin Most common sites are ventricular outflow
- 4. Idiopathic left VT Left posterior fascicle Left anterior fascicle High septal fascicle Others Mitral annulus Tricuspid
- 5. OUTFLOW TRACT VT Idiopathic VT originate most commonly in outflow tract area Nearly 80% of which
- 6. Phenotypes are a continuum of the same focal cellular process Premature ventricular complexes (PVCs) Nonsustained,repetitive monomorphic
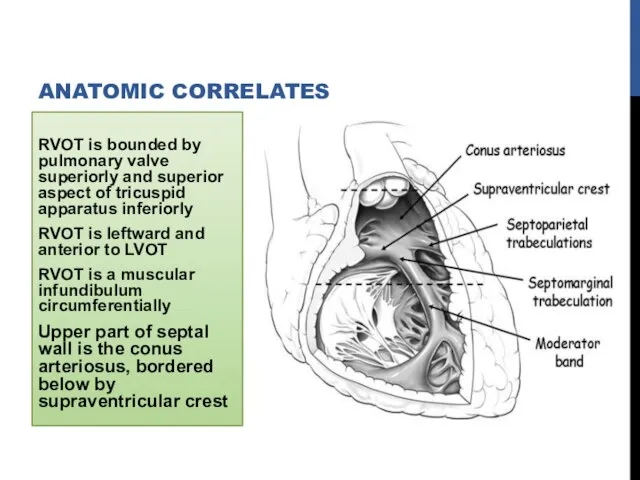
- 7. RVOT is bounded by pulmonary valve superiorly and superior aspect of tricuspid apparatus inferiorly RVOT is
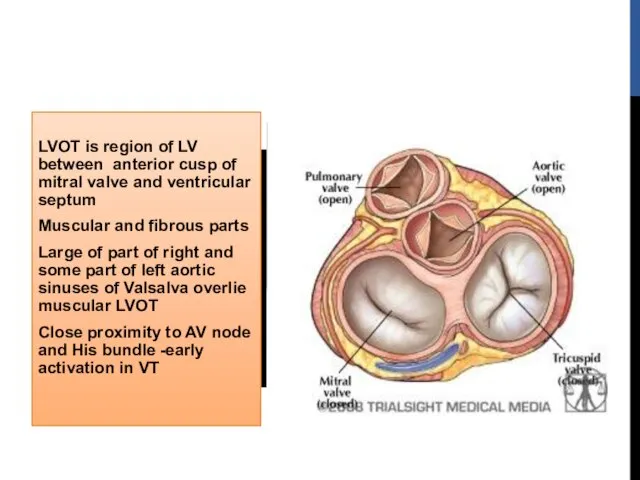
- 8. LVOT is region of LV between anterior cusp of mitral valve and ventricular septum Muscular and
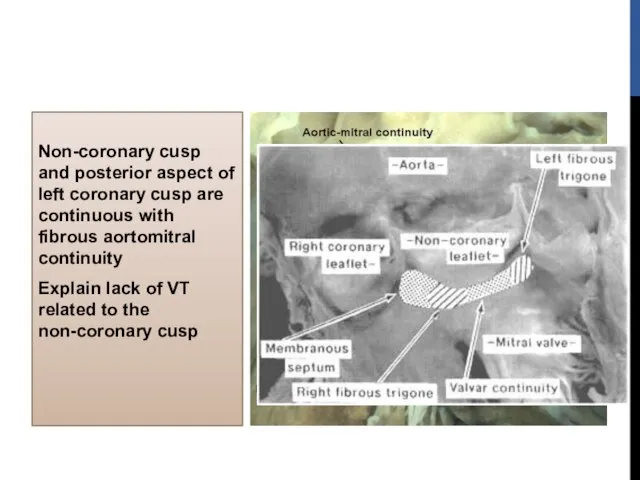
- 9. Non-coronary cusp and posterior aspect of left coronary cusp are continuous with fibrous aortomitral continuity Explain
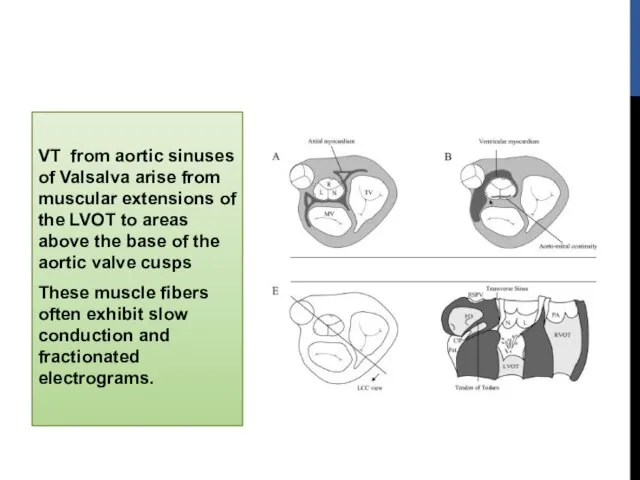
- 10. VT from aortic sinuses of Valsalva arise from muscular extensions of the LVOT to areas above
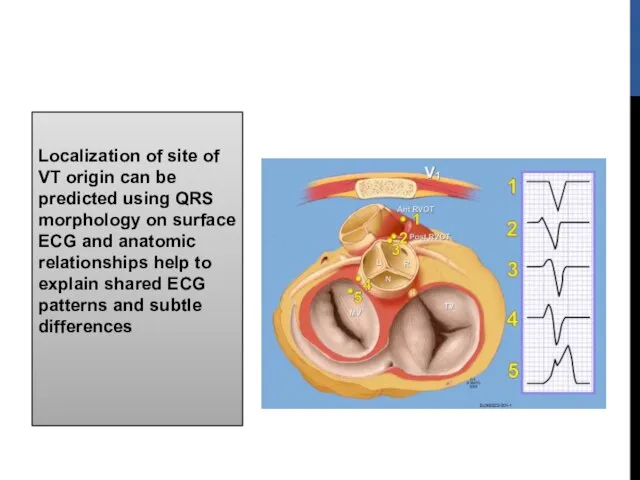
- 11. Localization of site of VT origin can be predicted using QRS morphology on surface ECG and
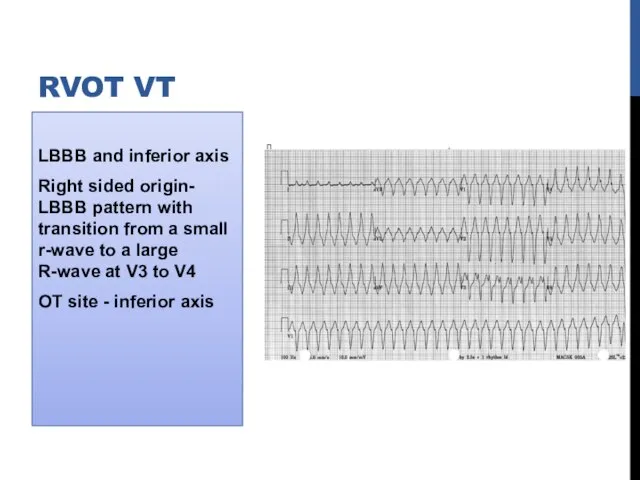
- 12. LBBB and inferior axis Right sided origin- LBBB pattern with transition from a small r-wave to
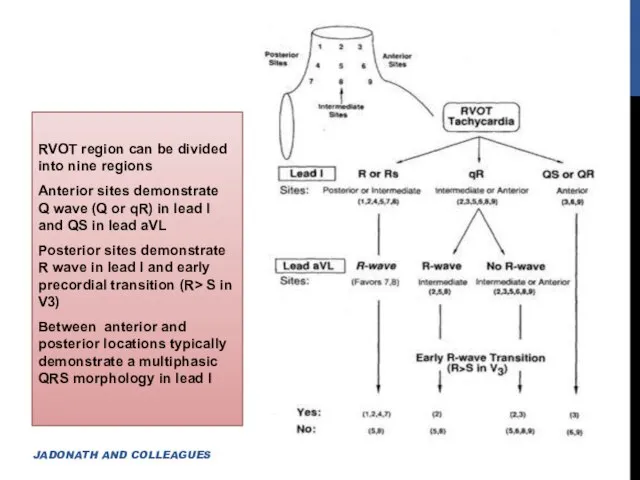
- 13. RVOT region can be divided into nine regions Anterior sites demonstrate Q wave (Q or qR)
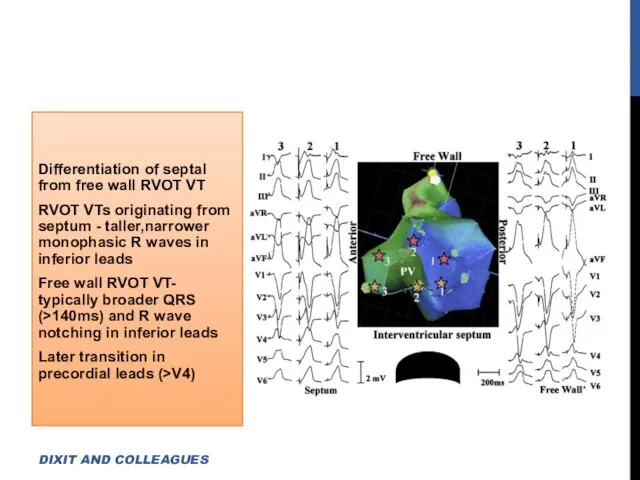
- 14. Differentiation of septal from free wall RVOT VT RVOT VTs originating from septum - taller,narrower monophasic
- 15. Anterior position of free wall relative to septum -Accounts for deeper S wave in lead V2
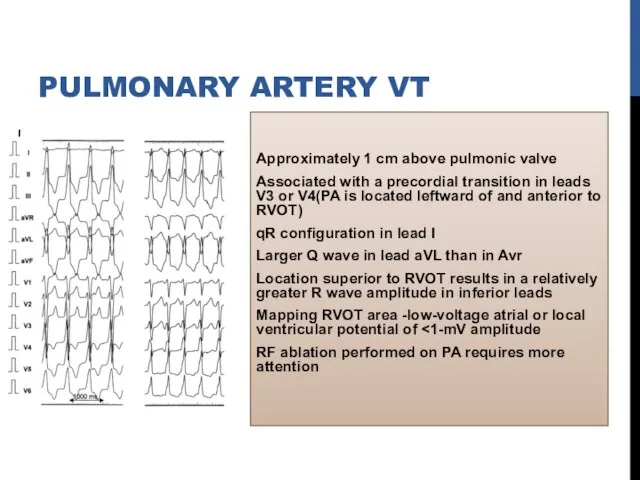
- 16. Approximately 1 cm above pulmonic valve Associated with a precordial transition in leads V3 or V4(PA
- 17. Atriofascicular fibers (Mahaim fibers) AVRT using Rt-sided accessory pathway VT after repair of TOF ARVD DIFFERENTIAL
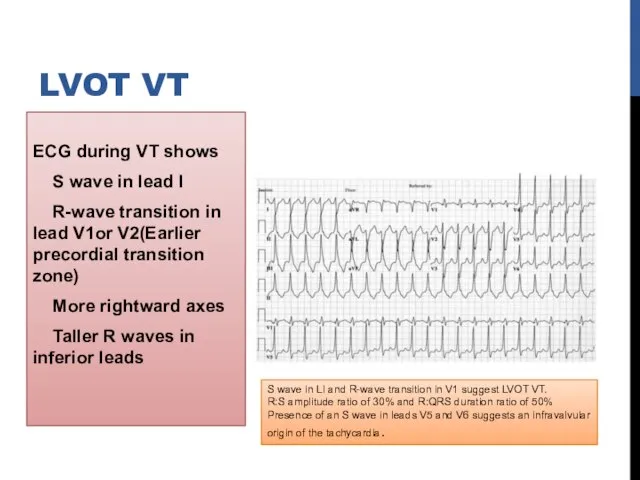
- 18. ECG during VT shows S wave in lead I R-wave transition in lead V1or V2(Earlier precordial
- 19. Shows one of the following depending on site of origin a)Basal left interventricular or septal origin
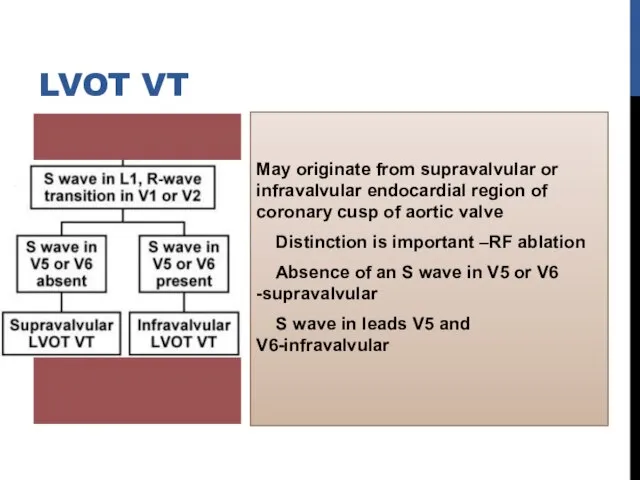
- 20. May originate from supravalvular or infravalvular endocardial region of coronary cusp of aortic valve Distinction is
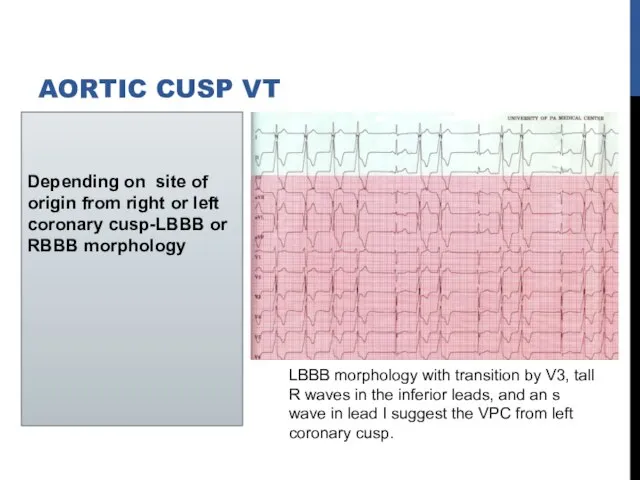
- 21. Depending on site of origin from right or left coronary cusp-LBBB or RBBB morphology AORTIC CUSP
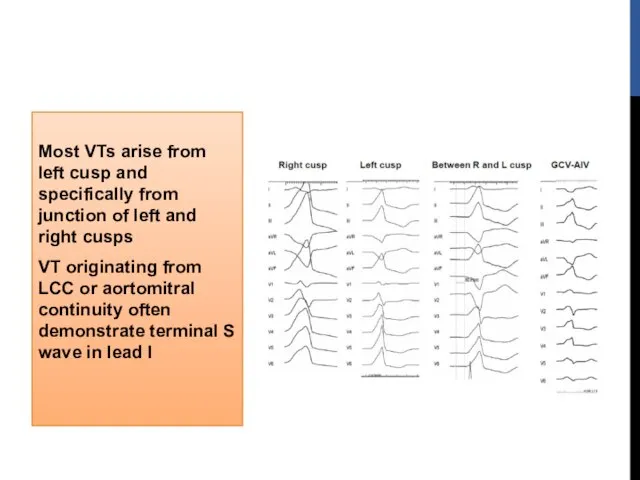
- 22. Most VTs arise from left cusp and specifically from junction of left and right cusps VT
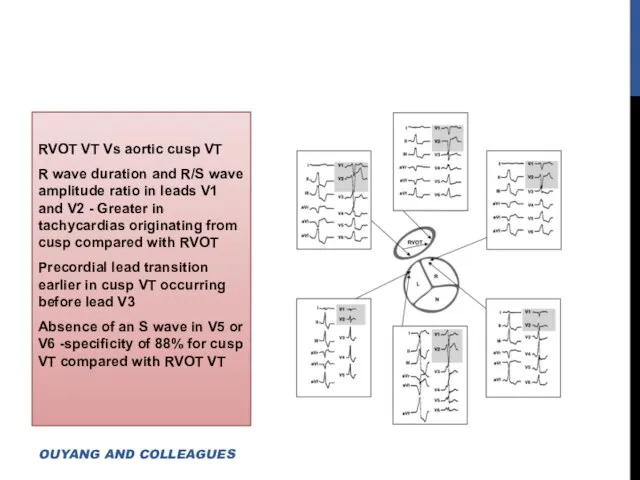
- 23. RVOT VT Vs aortic cusp VT R wave duration and R/S wave amplitude ratio in leads
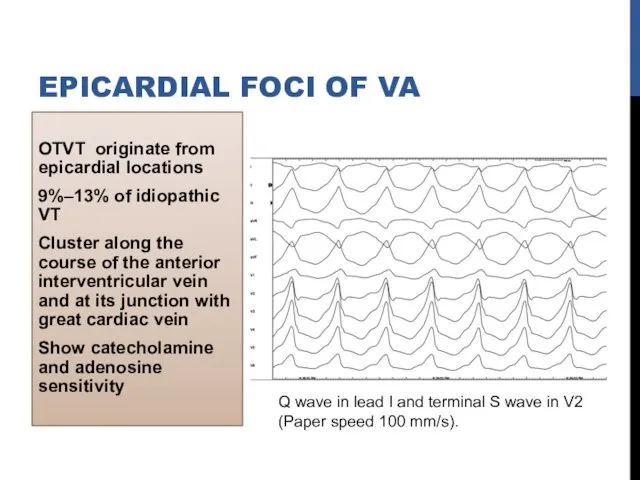
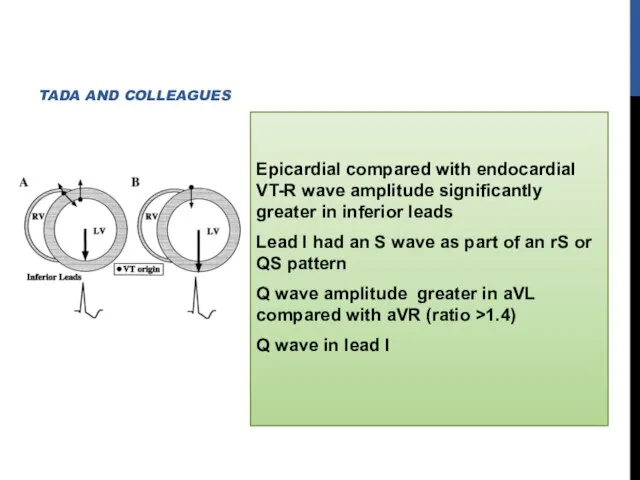
- 24. OTVT originate from epicardial locations 9%–13% of idiopathic VT Cluster along the course of the anterior
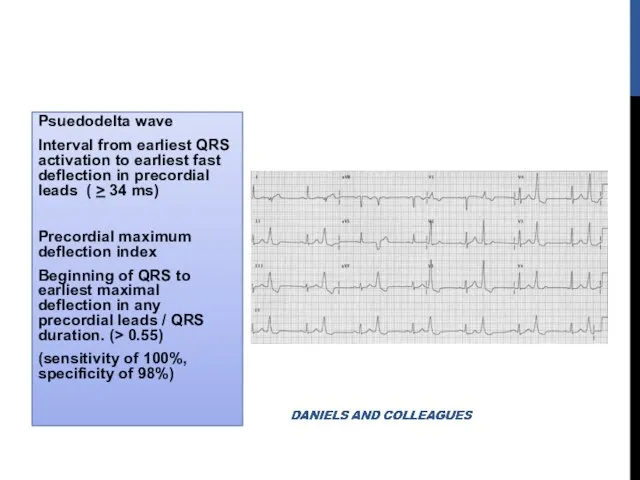
- 25. Psuedodelta wave Interval from earliest QRS activation to earliest fast deflection in precordial leads ( >
- 26. Epicardial compared with endocardial VT-R wave amplitude significantly greater in inferior leads Lead I had an
- 27. MITRAL ANNULUS, TRICUSPID ANNULUS PAPILLARY MUSCLE PERIVASCULAR EPICARDIAL ECTOPY
- 28. MITRAL ANNULAR VT Significant slurring of QRS complex onset resembling delta-wave Regardless of where along circumference
- 29. PVCs or VT also originate from RVOT along region of tricuspid annulus Most common site is
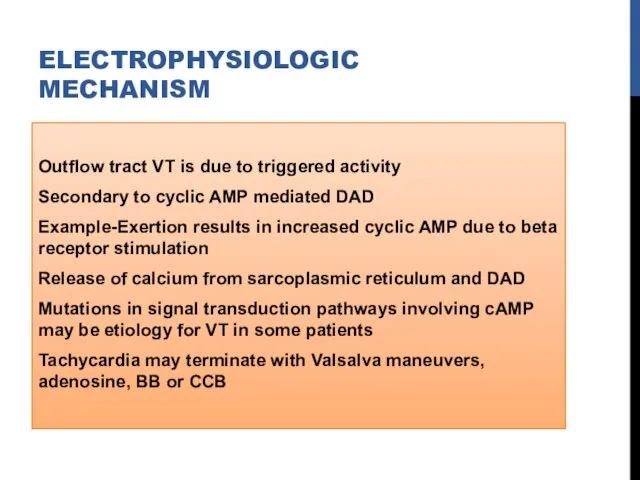
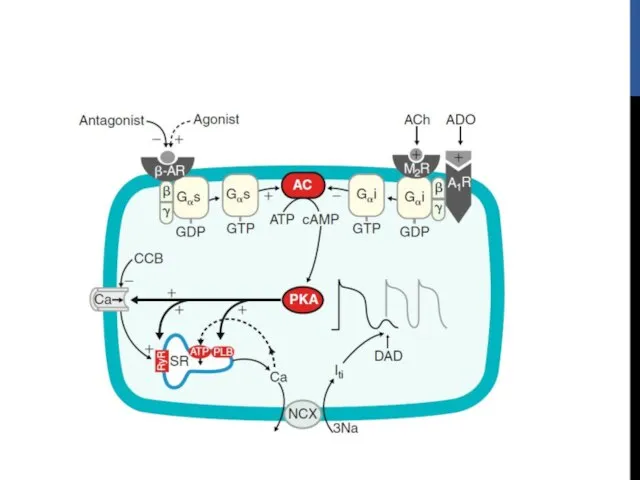
- 30. ELECTROPHYSIOLOGIC MECHANISM Outflow tract VT is due to triggered activity Secondary to cyclic AMP mediated DAD
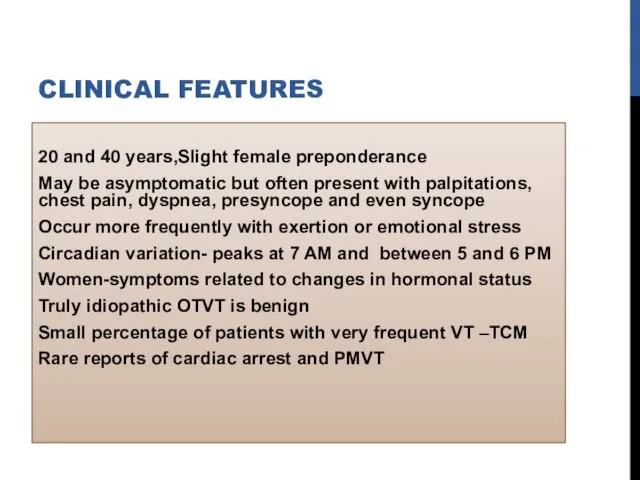
- 32. CLINICAL FEATURES 20 and 40 years,Slight female preponderance May be asymptomatic but often present with palpitations,
- 33. TREATMENT May respond acutely to carotid sinus massage, Valsalva maneuvers or intravenous adenosine or verapamil Long-term
- 34. RFA When medical therapy is ineffective or not tolerated High success rate (>80%) Ablation of epicardial
- 35. Tachycardia localization 12-lead ECG Intracardiac activation Pace mapping
- 36. BIPOLAR ACTIVATION MAPPING
- 37. PACE MAPPING Useful because typically site of origin is focal and because underlying tissue is normal
- 38. ELECTROANATOMIC RE-CREATION OF 3D ANATOMY Helpful for catheter mapping and localization of site of origin Incessant
- 39. Predictors for successful ablation Single VT morphology Accurate pace maps Absence of a deltalike wave at
- 40. Some tachycardias arise from epicardium, necessitate ablation from great cardiac vein or epicardium itself using pericardial
- 41. Complications during outflow tract VT ablation are rare RBBB (1%) Cardiac perforation Damage to the coronary
- 42. IDIOPATHIC LEFT VT Three varieties left posterior fascicular VT -RBBB and LAD (90%) left anterior fascicular
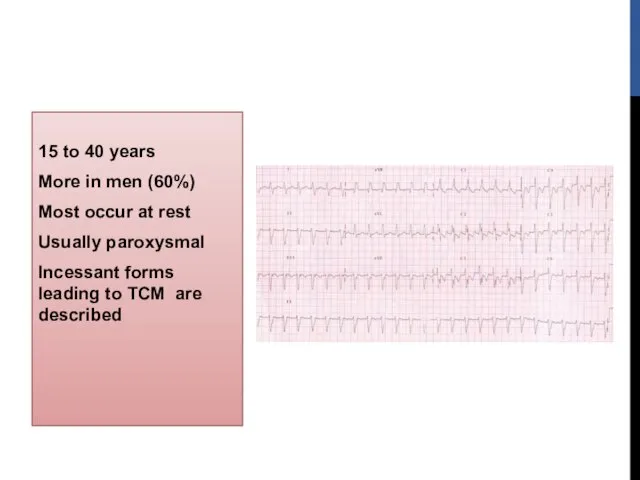
- 43. 15 to 40 years More in men (60%) Most occur at rest Usually paroxysmal Incessant forms
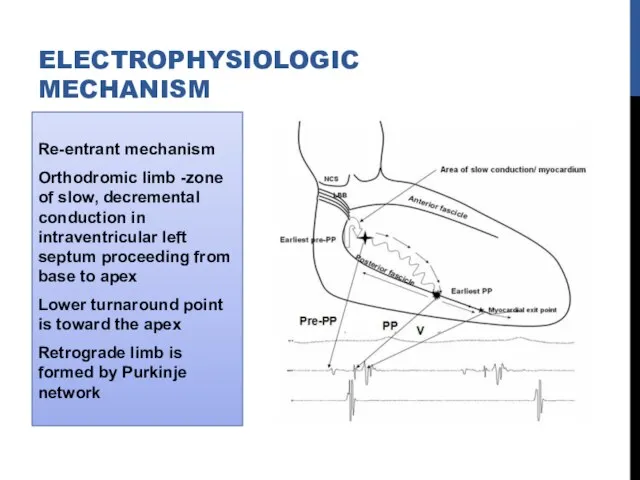
- 44. Re-entrant mechanism Orthodromic limb -zone of slow, decremental conduction in intraventricular left septum proceeding from base
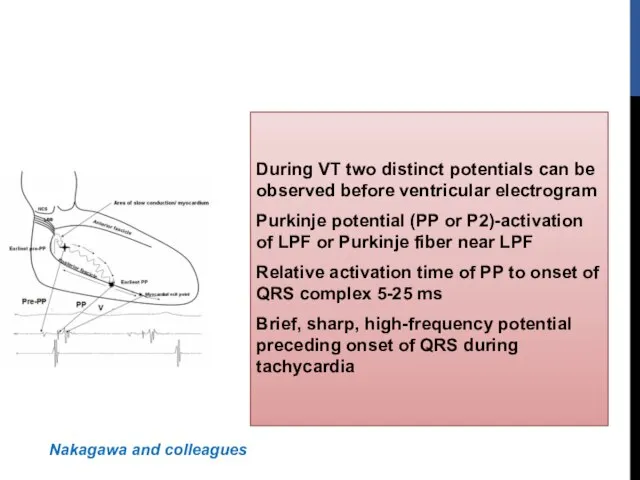
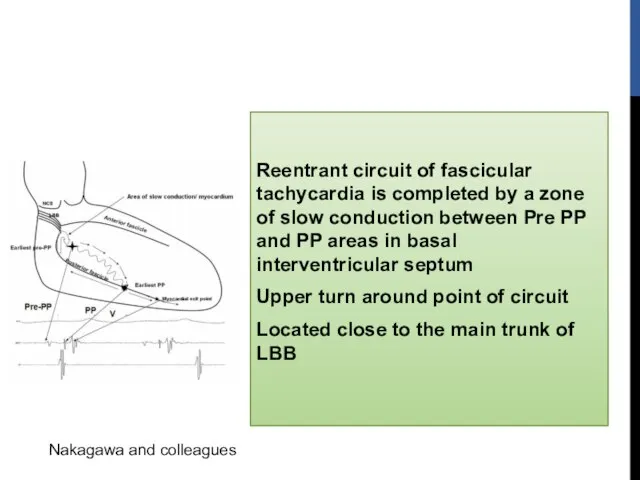
- 45. During VT two distinct potentials can be observed before ventricular electrogram Purkinje potential (PP or P2)-activation
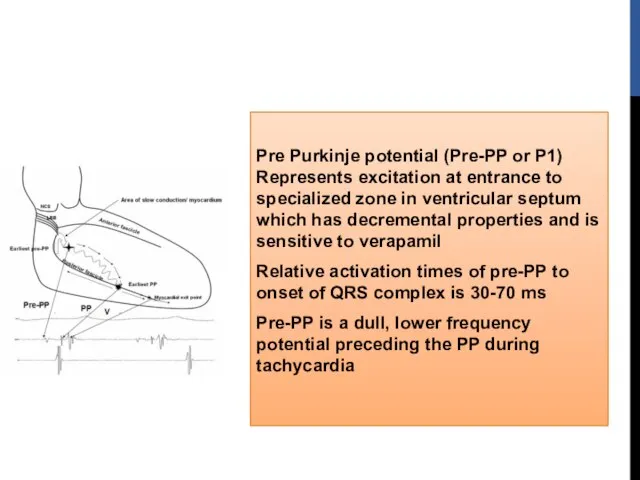
- 46. Pre Purkinje potential (Pre-PP or P1) Represents excitation at entrance to specialized zone in ventricular septum
- 47. Reentrant circuit of fascicular tachycardia is completed by a zone of slow conduction between Pre PP
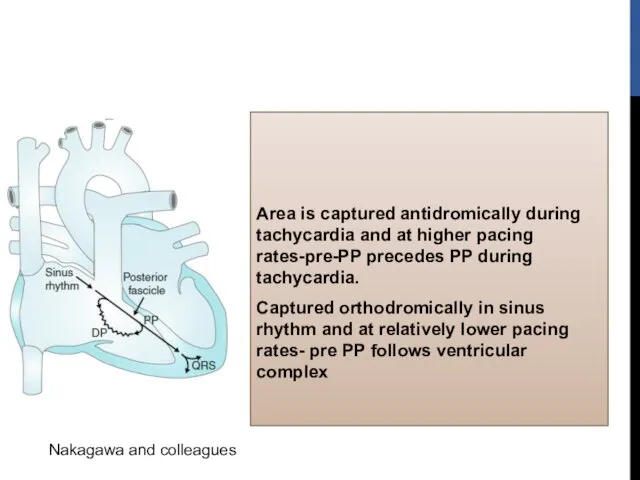
- 48. Area is captured antidromically during tachycardia and at higher pacing rates-pre-PP precedes PP during tachycardia. Captured
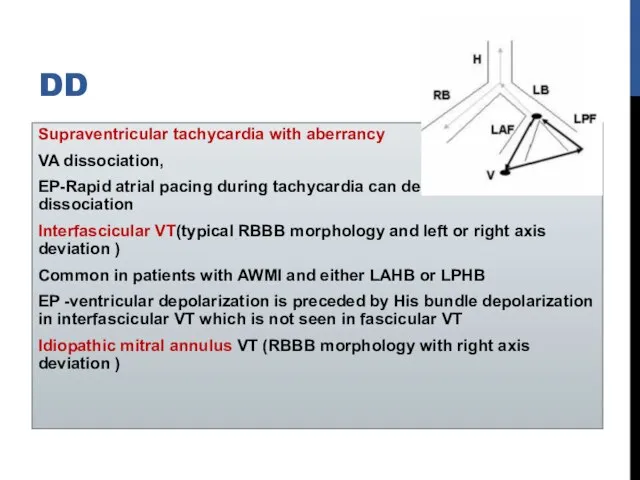
- 49. DD Supraventricular tachycardia with aberrancy VA dissociation, EP-Rapid atrial pacing during tachycardia can demonstrate AV dissociation
- 50. VT originates from a false tendon extends from posteroinferior left ventricle to basal septum Resection of
- 51. ECG Baseline 12-lead ECG is normal in most patients Exit near the area of the left
- 52. Long-term prognosis is very good Patients who have incessant tachycardia may develop tachycardia related cardiomyopathy Intravenous
- 53. RADIOFREQUENCY ABLATION Associated with significant symptoms or who are intolerant or resistant to medical therapy Strategies
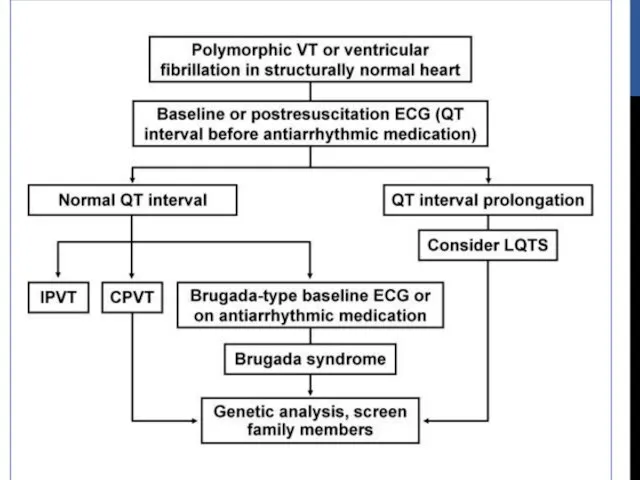
- 54. LIFE-THREATENING (TYPICALLY POLYMORPHIC VT) Rare Generally occurs with genetic ion channel disorders Associated with SCD Abnormalities
- 55. Long QT Syndrome Brugada Syndrome CPVT Short QT Syndrome LIFE-THREATENING (TYPICALLY POLYMORPHIC VT)
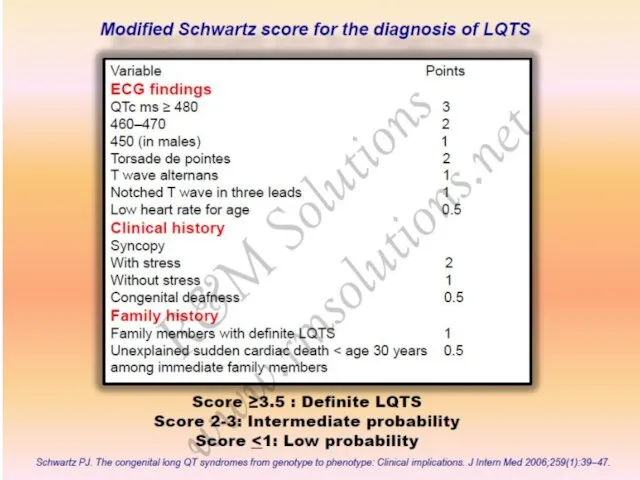
- 56. LONG QT SYNDROME Corrected QT interval 440 ms in men and 460 ms in women with
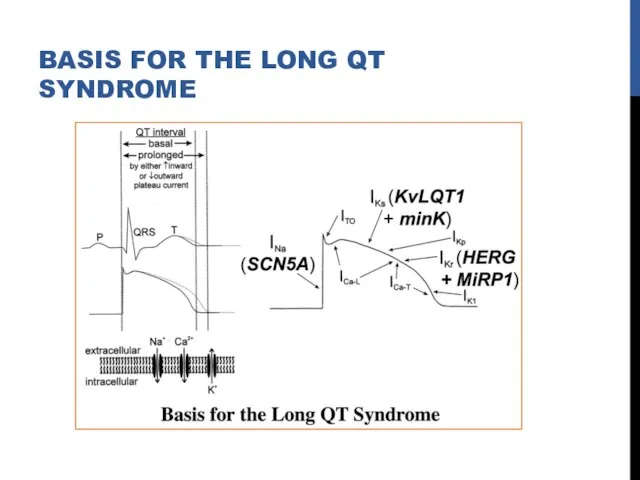
- 57. BASIS FOR THE LONG QT SYNDROME
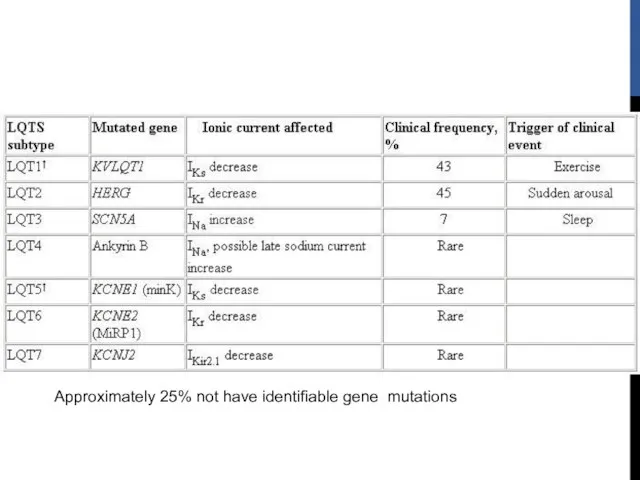
- 58. Approximately 25% not have identifiable gene mutations
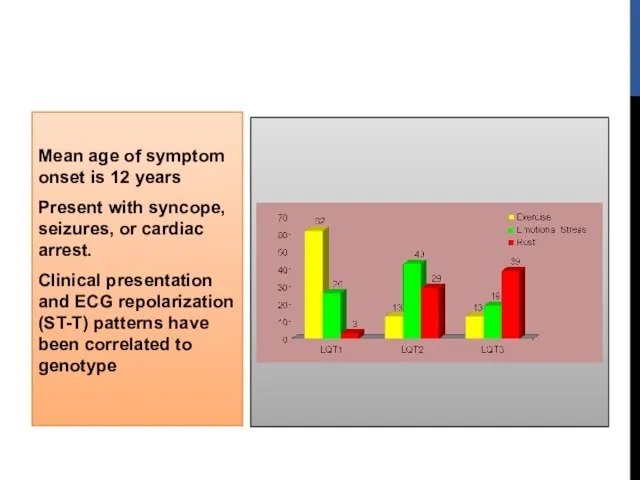
- 59. Mean age of symptom onset is 12 years Present with syncope, seizures, or cardiac arrest. Clinical
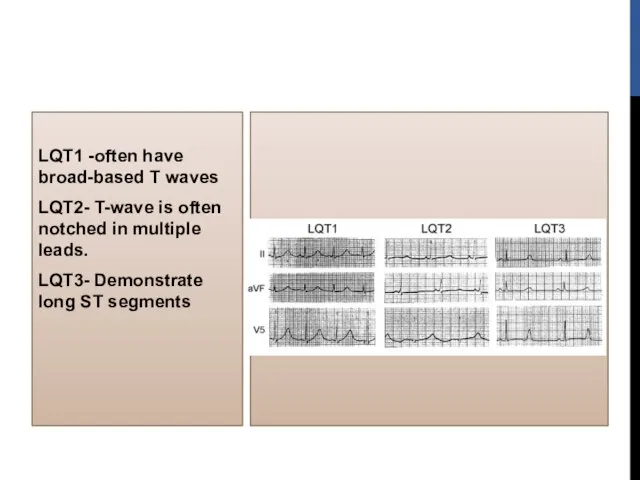
- 60. LQT1 -often have broad-based T waves LQT2- T-wave is often notched in multiple leads. LQT3- Demonstrate
- 62. MANAGEMENT Avoid trigger events and medications prolong QT interval Risk stratification -degree of QT prolongation, genotype
- 63. MEDICATIONS PROLONG QT INTERVAL Antiarrhythmic: procainamide, quinidine, amiodarone, sotalol Antihistamine: astemizole, terfenadine Antimicrobial/antifungal: trimethoprim sulfa, erythromycin,
- 64. MANAGEMENT BB -patients with syncope and asymptomatic patients with significant QT prolongation Role of BB in
- 65. MANAGEMENT ICD are indicated for secondary prevention of cardiac arrest and for patients with recurrent syncope
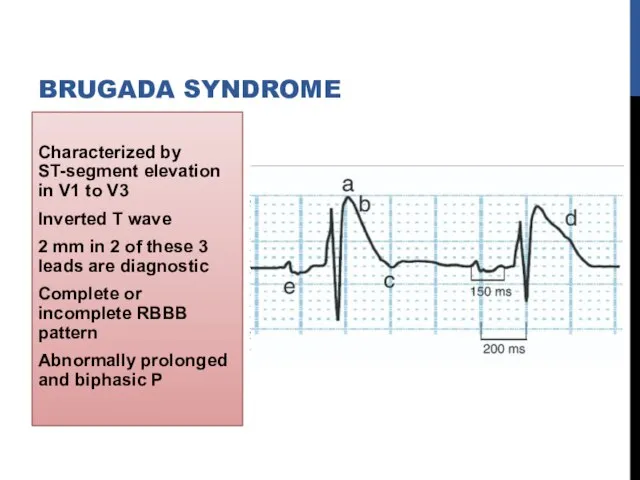
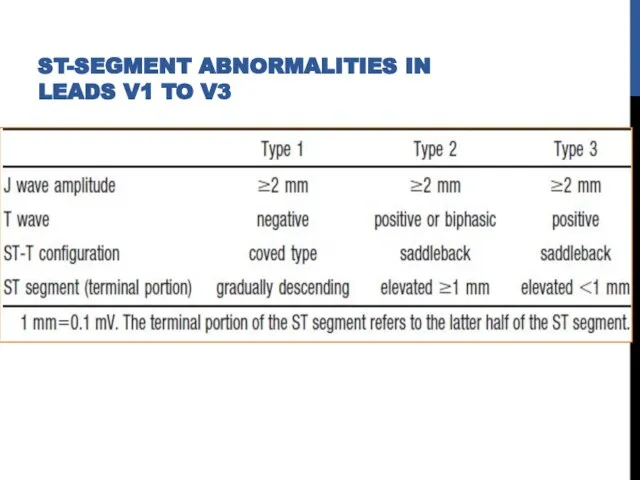
- 66. Characterized by ST-segment elevation in V1 to V3 Inverted T wave 2 mm in 2 of
- 67. ST-SEGMENT ABNORMALITIES IN LEADS V1 TO V3
- 68. Typical ECG pattern can be transient and may only be detected during long-term ECG monitoring Methods
- 69. CLINICAL PRESENTATION 0.12% to 0.14% in general population Syncope or cardiac arrest Predominantly in men in
- 70. Risk of SCD with Brugada syndrome is substantial Risk of recurrent events during 4 years of
- 71. TREATMENT Drugs inhibit Ito (such as quinidine) and increase calcium current (such as isoproterenol) are effective
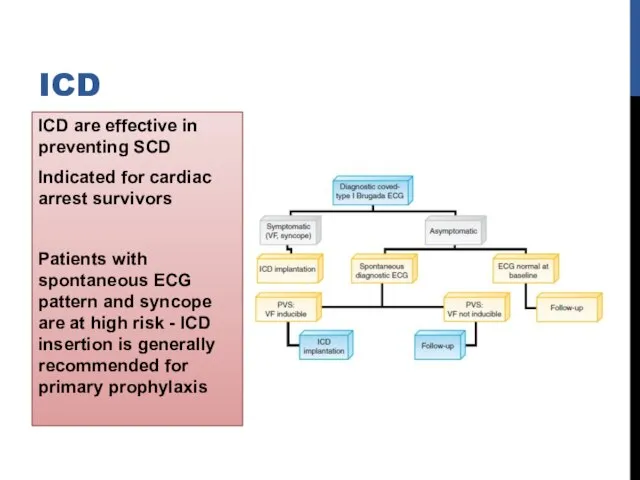
- 72. ICD are effective in preventing SCD Indicated for cardiac arrest survivors Patients with spontaneous ECG pattern
- 73. Different genes involved SCN5A gene mutations (BrS1) - loss of function of cardiac sodium channel (NaV
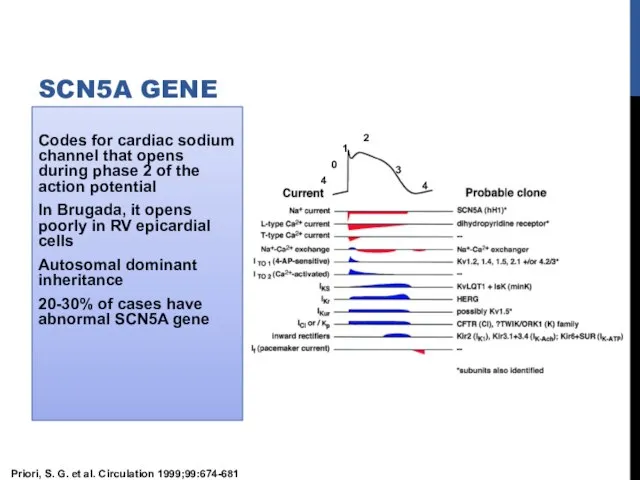
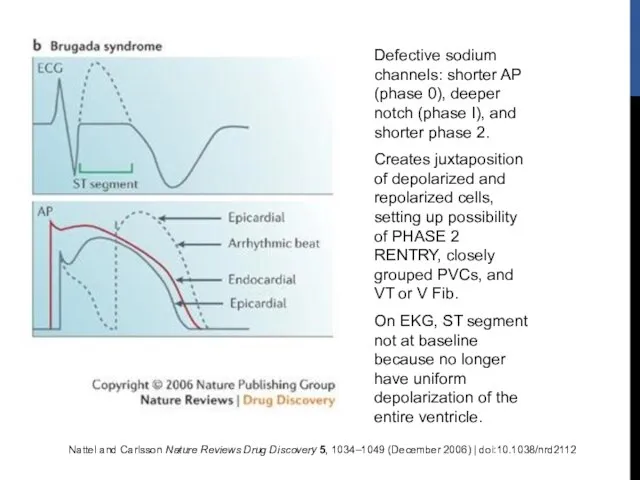
- 74. Codes for cardiac sodium channel that opens during phase 2 of the action potential In Brugada,
- 75. Nattel and Carlsson Nature Reviews Drug Discovery 5, 1034–1049 (December 2006) | doi:10.1038/nrd2112 Defective sodium channels:
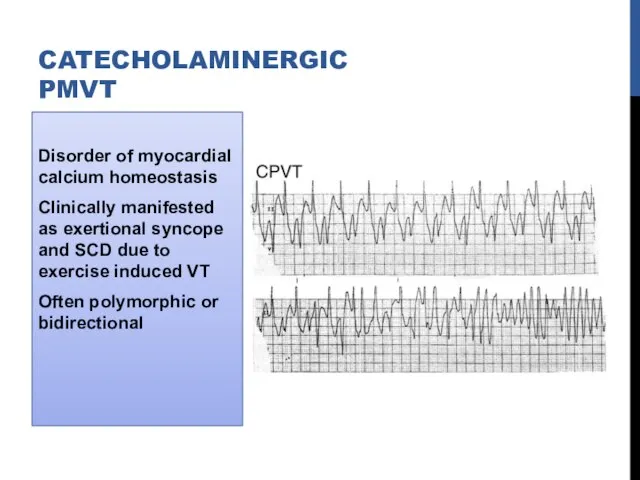
- 76. Disorder of myocardial calcium homeostasis Clinically manifested as exertional syncope and SCD due to exercise induced
- 77. Autosomal dominant (50% )-mutation of cardiac ryanodine receptor (RyR2 gene) Autosomal recessive (3% to 5% )-mutations
- 78. Ryanodine receptor spans membrane of sarcoplasmic reticulum Releases calcium triggered by calcium entry into cell through
- 79. Resting ECG is unremarkable, prominent U waves may be seen Typical VT patterns are reproducible with
- 80. Medical management-BB 46% may have recurrent events while receiving therapy CCB -limited effectiveness Flecainide (blocks RyR2
- 81. ICD Cardiac arrest Life-threatening VA despite maximal medical therapy Initial ICD shock with its accompanying pain
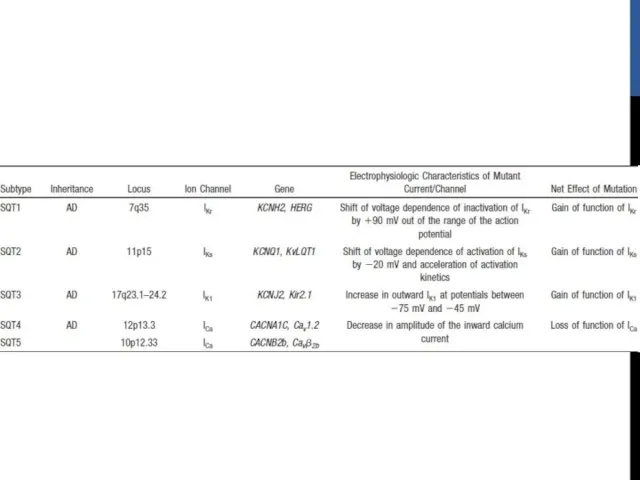
- 82. SHORT QT SYNDROME Rare disorder Characterized by short QT intervals of 300 to 320 ms Shortening
- 84. ICD implantation for secondary and primary prevention Preliminary observations suggest quinidine might be useful
- 85. IDIOPATHIC PROPRANOLOL-SENSITIVE VT (IPVT) Usually occurs by fifth decade of life Can arise from LV or
- 86. TREATMENT OF IPVT BBs effective in acute situations Insufficient information available regarding long-term management Survivors of
- 89. REFERENCES ZIPES 5th EDITION BRAUNWALD 9TH EDITION HURST 13TH EDITION VENTRICULAR ARRHYTHMIAS IN NORMAL HEARTS,SHUAIB LATIF,
- 91. Скачать презентацию
Слайд 3NON–LIFE-THREATENING
(TYPICALLY MONOMORPHIC)
Classified on basis of site of origin
Most common sites
NON–LIFE-THREATENING
(TYPICALLY MONOMORPHIC)
Classified on basis of site of origin
Most common sites
Слайд 4Idiopathic left VT
Left posterior fascicle
Left anterior fascicle
High septal fascicle
Others
Mitral annulus
Tricuspid annulus
Papillary muscle
Perivascular
Left posterior fascicle
Left anterior fascicle
High septal fascicle
Others
Mitral annulus
Tricuspid annulus
Papillary muscle
Perivascular
Слайд 5OUTFLOW TRACT VT
Idiopathic VT originate most commonly in outflow tract area
Nearly
OUTFLOW TRACT VT
Idiopathic VT originate most commonly in outflow tract area
Nearly
Слайд 6Phenotypes are a continuum of the same focal cellular process
Premature ventricular
Premature ventricular
Слайд 7RVOT is bounded by pulmonary valve superiorly and superior aspect of tricuspid
Слайд 8LVOT is region of LV between anterior cusp of mitral valve and
Слайд 9Non-coronary cusp and posterior aspect of left coronary cusp are continuous with
Слайд 10VT from aortic sinuses of Valsalva arise from muscular extensions of the
Слайд 11Localization of site of VT origin can be predicted using QRS morphology
Слайд 12LBBB and inferior axis
Right sided origin- LBBB pattern with transition from
Right sided origin- LBBB pattern with transition from
Слайд 13RVOT region can be divided into nine regions
Anterior sites demonstrate Q
Anterior sites demonstrate Q
Слайд 14Differentiation of septal from free wall RVOT VT
RVOT VTs originating from
RVOT VTs originating from
Слайд 15Anterior position of free wall relative to septum -Accounts for deeper S
Слайд 16Approximately 1 cm above pulmonic valve
Associated with a precordial transition in leads
Associated with a precordial transition in leads
Слайд 17Atriofascicular fibers (Mahaim fibers)
AVRT using Rt-sided accessory pathway
VT after repair of TOF
ARVD
DIFFERENTIAL
AVRT using Rt-sided accessory pathway
VT after repair of TOF
ARVD
DIFFERENTIAL
Слайд 18ECG during VT shows
S wave in lead I
R-wave transition
S wave in lead I
R-wave transition
Слайд 19Shows one of the following depending on site of origin
a)Basal left interventricular
a)Basal left interventricular
Слайд 20May originate from supravalvular or infravalvular endocardial region of coronary cusp of
Слайд 21Depending on site of origin from right or left coronary cusp-LBBB or
Слайд 22Most VTs arise from left cusp and specifically from junction of left
Слайд 23RVOT VT Vs aortic cusp VT
R wave duration and R/S wave amplitude
R wave duration and R/S wave amplitude
Слайд 24OTVT originate from epicardial locations
9%–13% of idiopathic VT
Cluster along the course
9%–13% of idiopathic VT
Cluster along the course
Слайд 25Psuedodelta wave
Interval from earliest QRS activation to earliest fast deflection in precordial
Psuedodelta wave
Interval from earliest QRS activation to earliest fast deflection in precordial
Слайд 26Epicardial compared with endocardial VT-R wave amplitude significantly greater in inferior leads
Слайд 27MITRAL ANNULUS,
TRICUSPID ANNULUS
PAPILLARY MUSCLE
PERIVASCULAR EPICARDIAL ECTOPY
MITRAL ANNULUS,
TRICUSPID ANNULUS
PAPILLARY MUSCLE
PERIVASCULAR EPICARDIAL ECTOPY
Слайд 28MITRAL ANNULAR VT
Significant slurring of QRS complex onset resembling delta-wave
Regardless of where
MITRAL ANNULAR VT
Significant slurring of QRS complex onset resembling delta-wave
Regardless of where
Слайд 29PVCs or VT also originate from RVOT along region of tricuspid annulus
Слайд 30ELECTROPHYSIOLOGIC MECHANISM
Outflow tract VT is due to triggered activity
Secondary to cyclic
ELECTROPHYSIOLOGIC MECHANISM
Outflow tract VT is due to triggered activity
Secondary to cyclic
Слайд 32CLINICAL FEATURES
20 and 40 years,Slight female preponderance
May be asymptomatic but often
CLINICAL FEATURES
20 and 40 years,Slight female preponderance
May be asymptomatic but often
Слайд 33TREATMENT
May respond acutely to carotid sinus massage, Valsalva maneuvers or intravenous adenosine
TREATMENT
May respond acutely to carotid sinus massage, Valsalva maneuvers or intravenous adenosine
Слайд 34RFA
When medical therapy is ineffective or not tolerated
High success rate (>80%)
RFA
When medical therapy is ineffective or not tolerated
High success rate (>80%)
Слайд 35Tachycardia localization
12-lead ECG
Intracardiac activation
Pace mapping
12-lead ECG
Intracardiac activation
Pace mapping

Слайд 36BIPOLAR ACTIVATION MAPPING
BIPOLAR ACTIVATION MAPPING
Слайд 37PACE MAPPING
Useful because typically site of origin is focal and because
PACE MAPPING
Useful because typically site of origin is focal and because
Слайд 38
ELECTROANATOMIC RE-CREATION OF 3D ANATOMY
Helpful for catheter mapping and localization of
ELECTROANATOMIC RE-CREATION OF 3D ANATOMY
Helpful for catheter mapping and localization of
Слайд 39Predictors for successful ablation
Single VT morphology
Accurate pace maps
Absence of a deltalike
Single VT morphology
Accurate pace maps
Absence of a deltalike
Слайд 40Some tachycardias arise from epicardium, necessitate ablation from great cardiac vein or
Слайд 41Complications during outflow tract VT ablation are rare
RBBB (1%)
Cardiac perforation
Damage to the
RBBB (1%)
Cardiac perforation
Damage to the
Слайд 42IDIOPATHIC LEFT VT
Three varieties
left posterior fascicular VT -RBBB and LAD (90%)
left anterior
IDIOPATHIC LEFT VT
Three varieties
left posterior fascicular VT -RBBB and LAD (90%)
left anterior
Слайд 4315 to 40 years
More in men (60%)
Most occur at rest
Usually
More in men (60%)
Most occur at rest
Usually
Слайд 44Re-entrant mechanism
Orthodromic limb -zone of slow, decremental conduction in intraventricular left
Orthodromic limb -zone of slow, decremental conduction in intraventricular left
Слайд 45During VT two distinct potentials can be observed before ventricular electrogram
Purkinje potential
Purkinje potential
Слайд 46Pre Purkinje potential (Pre-PP or P1) Represents excitation at entrance to specialized
Слайд 47Reentrant circuit of fascicular tachycardia is completed by a zone of slow
Слайд 48Area is captured antidromically during tachycardia and at higher pacing rates-pre-PP precedes
Слайд 49DD
Supraventricular tachycardia with aberrancy
VA dissociation,
EP-Rapid atrial pacing during tachycardia can
DD
Supraventricular tachycardia with aberrancy
VA dissociation,
EP-Rapid atrial pacing during tachycardia can
Слайд 50VT originates from a false tendon extends from posteroinferior left ventricle to
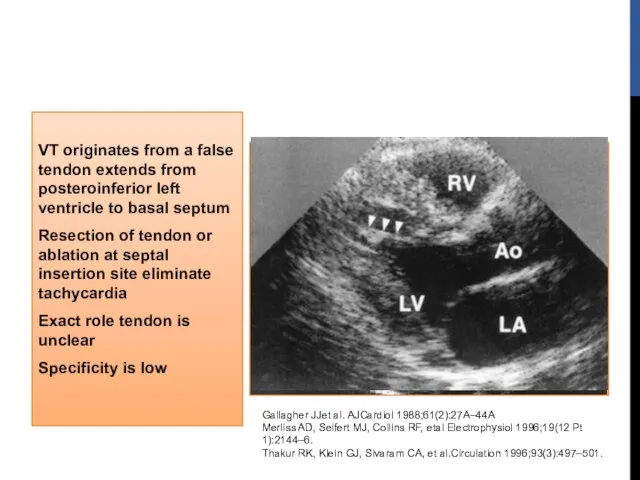
Слайд 51ECG
Baseline 12-lead ECG is normal in most patients
Exit near the area of
ECG
Baseline 12-lead ECG is normal in most patients
Exit near the area of
Слайд 52Long-term prognosis is very good
Patients who have incessant tachycardia may develop tachycardia
Patients who have incessant tachycardia may develop tachycardia
Слайд 53RADIOFREQUENCY ABLATION
Associated with significant symptoms or who are intolerant or resistant to
RADIOFREQUENCY ABLATION
Associated with significant symptoms or who are intolerant or resistant to
Слайд 54LIFE-THREATENING
(TYPICALLY POLYMORPHIC VT)
Rare
Generally occurs with genetic ion channel disorders
Associated with
LIFE-THREATENING
(TYPICALLY POLYMORPHIC VT)
Rare
Generally occurs with genetic ion channel disorders
Associated with
Слайд 55Long QT Syndrome
Brugada Syndrome
CPVT
Short QT Syndrome
LIFE-THREATENING
(TYPICALLY POLYMORPHIC VT)
Brugada Syndrome
CPVT
Short QT Syndrome
LIFE-THREATENING
(TYPICALLY POLYMORPHIC VT)
Слайд 56LONG QT SYNDROME
Corrected QT interval 440 ms in men and 460 ms
LONG QT SYNDROME
Corrected QT interval 440 ms in men and 460 ms
Слайд 57BASIS FOR THE LONG QT SYNDROME
BASIS FOR THE LONG QT SYNDROME
Слайд 58Approximately 25% not have identifiable gene mutations
Approximately 25% not have identifiable gene mutations
Слайд 59
Mean age of symptom onset is 12 years
Present with syncope, seizures, or
Mean age of symptom onset is 12 years
Present with syncope, seizures, or
Слайд 60
LQT1 -often have broad-based T waves
LQT2- T-wave is often notched in
LQT1 -often have broad-based T waves
LQT2- T-wave is often notched in
Слайд 62MANAGEMENT
Avoid trigger events and medications prolong QT interval
Risk stratification -degree
MANAGEMENT
Avoid trigger events and medications prolong QT interval
Risk stratification -degree
Слайд 63MEDICATIONS PROLONG QT INTERVAL
Antiarrhythmic: procainamide, quinidine, amiodarone, sotalol
Antihistamine: astemizole, terfenadine
Antimicrobial/antifungal: trimethoprim
MEDICATIONS PROLONG QT INTERVAL
Antiarrhythmic: procainamide, quinidine, amiodarone, sotalol
Antihistamine: astemizole, terfenadine
Antimicrobial/antifungal: trimethoprim
Слайд 64MANAGEMENT
BB -patients with syncope and asymptomatic patients with significant QT prolongation
Role
MANAGEMENT
BB -patients with syncope and asymptomatic patients with significant QT prolongation
Role
Слайд 65MANAGEMENT
ICD are indicated for secondary prevention of cardiac arrest and for patients
MANAGEMENT
ICD are indicated for secondary prevention of cardiac arrest and for patients
Слайд 66Characterized by ST-segment elevation in V1 to V3
Inverted T wave
2 mm
Inverted T wave
2 mm
Слайд 67ST-SEGMENT ABNORMALITIES IN LEADS V1 TO V3
ST-SEGMENT ABNORMALITIES IN LEADS V1 TO V3
Слайд 68Typical ECG pattern can be transient and may only be detected during
Слайд 69CLINICAL PRESENTATION
0.12% to 0.14% in general population
Syncope or cardiac arrest
Predominantly in
CLINICAL PRESENTATION
0.12% to 0.14% in general population
Syncope or cardiac arrest
Predominantly in
Слайд 70Risk of SCD with Brugada syndrome is substantial
Risk of recurrent events
Risk of recurrent events
Слайд 71TREATMENT
Drugs inhibit Ito (such as quinidine) and increase calcium current (such as
TREATMENT
Drugs inhibit Ito (such as quinidine) and increase calcium current (such as
Слайд 72ICD are effective in preventing SCD
Indicated for cardiac arrest survivors
Patients
ICD are effective in preventing SCD
Indicated for cardiac arrest survivors
Patients
Слайд 73Different genes involved
SCN5A gene mutations (BrS1) - loss of function of
SCN5A gene mutations (BrS1) - loss of function of
Слайд 74Codes for cardiac sodium channel that opens during phase 2 of the
Слайд 75Nattel and Carlsson Nature Reviews Drug Discovery 5, 1034–1049 (December 2006) |
Nattel and Carlsson Nature Reviews Drug Discovery 5, 1034–1049 (December 2006) |
Слайд 76Disorder of myocardial calcium homeostasis
Clinically manifested as exertional syncope and SCD due
Clinically manifested as exertional syncope and SCD due
Слайд 77Autosomal dominant (50% )-mutation of cardiac ryanodine receptor (RyR2 gene)
Autosomal recessive
Autosomal recessive
Слайд 78Ryanodine receptor spans membrane of sarcoplasmic reticulum
Releases calcium triggered by calcium
Releases calcium triggered by calcium
Слайд 79Resting ECG is unremarkable, prominent U waves may be seen
Typical VT patterns
Typical VT patterns
Слайд 80Medical management-BB
46% may have recurrent events while receiving therapy
CCB -limited effectiveness
Flecainide
46% may have recurrent events while receiving therapy
CCB -limited effectiveness
Flecainide
Слайд 81ICD
Cardiac arrest
Life-threatening VA despite maximal medical therapy
Initial ICD shock with
ICD
Cardiac arrest
Life-threatening VA despite maximal medical therapy
Initial ICD shock with
Слайд 82SHORT QT SYNDROME
Rare disorder
Characterized by short QT intervals of 300 to
SHORT QT SYNDROME
Rare disorder
Characterized by short QT intervals of 300 to
Слайд 84ICD implantation for secondary and primary prevention
Preliminary observations suggest quinidine might
Preliminary observations suggest quinidine might
Слайд 85IDIOPATHIC PROPRANOLOL-SENSITIVE VT (IPVT)
Usually occurs by fifth decade of life
Can arise
IDIOPATHIC PROPRANOLOL-SENSITIVE VT (IPVT)
Usually occurs by fifth decade of life
Can arise
Слайд 86
TREATMENT OF IPVT
BBs effective in acute situations
Insufficient information available regarding long-term
TREATMENT OF IPVT
BBs effective in acute situations
Insufficient information available regarding long-term
Слайд 89REFERENCES
ZIPES 5th EDITION
BRAUNWALD 9TH EDITION
HURST 13TH EDITION
VENTRICULAR ARRHYTHMIAS IN NORMAL HEARTS,SHUAIB
REFERENCES
ZIPES 5th EDITION
BRAUNWALD 9TH EDITION
HURST 13TH EDITION
VENTRICULAR ARRHYTHMIAS IN NORMAL HEARTS,SHUAIB
 Детский фонд ООН (ЮНИСЕФ)
Детский фонд ООН (ЮНИСЕФ) Гломерулонефриты
Гломерулонефриты Воля
Воля Брюшной тиф. Шигеллёз. Сестринское дело
Брюшной тиф. Шигеллёз. Сестринское дело 3 декабря - Международный день инвалидов
3 декабря - Международный день инвалидов ЖИВАЯ МАТЕРИЯ ПРИ НИЗКИХ И СВЕРХНИЗКИХ ТЕМПЕРАТУРАХ И. В. Артюхов
ЖИВАЯ МАТЕРИЯ ПРИ НИЗКИХ И СВЕРХНИЗКИХ ТЕМПЕРАТУРАХ И. В. Артюхов 02 Изготовление индивидуальных ложек и окклюзионных валиков
02 Изготовление индивидуальных ложек и окклюзионных валиков Острый панкреатит: этиология и патогенез
Острый панкреатит: этиология и патогенез Жүректің иннервациясы
Жүректің иннервациясы Опасности и осложнения при лечении грыж
Опасности и осложнения при лечении грыж Шөптердің дәрілік қасиеттері
Шөптердің дәрілік қасиеттері Иммунитет. Виды иммунитета
Иммунитет. Виды иммунитета Ранняя диагностика сахарного диабета
Ранняя диагностика сахарного диабета Проекционные зоны коры головного мозга
Проекционные зоны коры головного мозга Суставной синдром при подагре
Суставной синдром при подагре Хирургическое лечение глаукомы
Хирургическое лечение глаукомы Роль ранней диагностики заболеваний в современной жизни людей
Роль ранней диагностики заболеваний в современной жизни людей HELLP-синдром. Диагностика и принципы интенсивной терапии
HELLP-синдром. Диагностика и принципы интенсивной терапии Портальная гипертензия
Портальная гипертензия Разработка технологии получения экстрактов, обогащенных фитоэстрогенами
Разработка технологии получения экстрактов, обогащенных фитоэстрогенами Медико-биологические основы физической культуры. Психофизиологические аспекты адаптации человека. (Лекция 3)
Медико-биологические основы физической культуры. Психофизиологические аспекты адаптации человека. (Лекция 3) Менструальный цикл
Менструальный цикл Особенности нервной системы и ее методика исследования у детей
Особенности нервной системы и ее методика исследования у детей Access бағдарламасы көмегімен Медециналык деректер базасын жоспарлау және құру
Access бағдарламасы көмегімен Медециналык деректер базасын жоспарлау және құру Десмургия
Десмургия Анализ клинического случая и обсуждение плана лечения
Анализ клинического случая и обсуждение плана лечения Мама и малыш после родов
Мама и малыш после родов Annual scientific report of pharmacognosy department. Pharmacognostic analysis of the raw materials
Annual scientific report of pharmacognosy department. Pharmacognostic analysis of the raw materials