- Yellow fever vaccine – past, present & future

Содержание
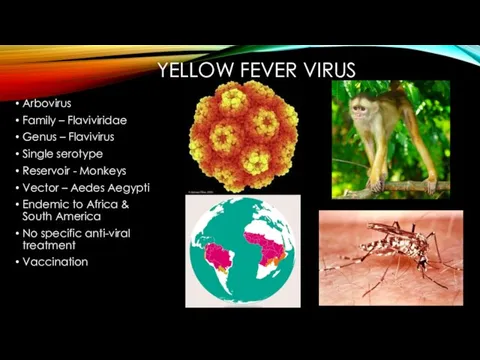
- 2. YELLOW FEVER VIRUS Arbovirus Family – Flaviviridae Genus – Flavivirus Single serotype Reservoir - Monkeys Vector
- 3. PAST 1912 – opening of Panama canal – increased global exposure – first modern attempt for
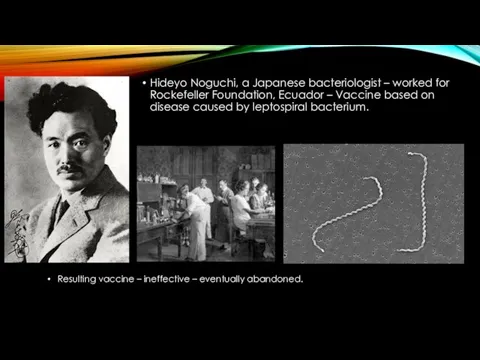
- 4. Hideyo Noguchi, a Japanese bacteriologist – worked for Rockefeller Foundation, Ecuador – Vaccine based on disease
- 5. “French strain” – obtained from a survivor – another vaccine by Pasteur Institute scientists. Administered by
- 6. Attempts to attenuate – failed. Another vaccine developed – derived from Asibi in 1927. First isolation
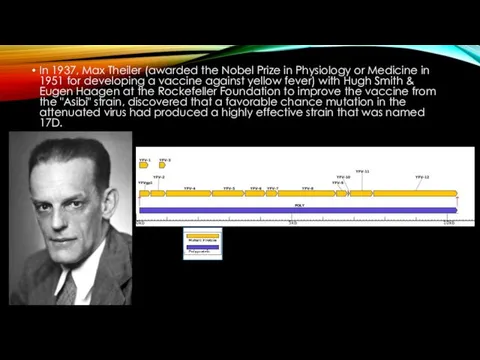
- 7. In 1937, Max Theiler (awarded the Nobel Prize in Physiology or Medicine in 1951 for developing
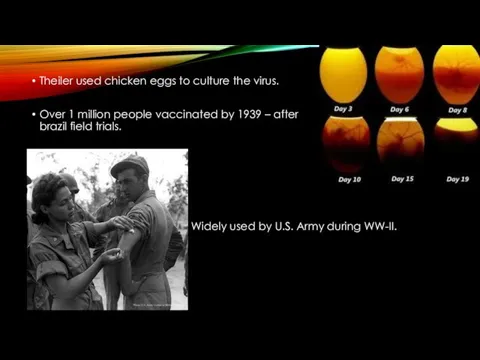
- 8. Theiler used chicken eggs to culture the virus. Over 1 million people vaccinated by 1939 –
- 9. Theiler’s vaccine – largest outbreak of Hepatits B – 330,000
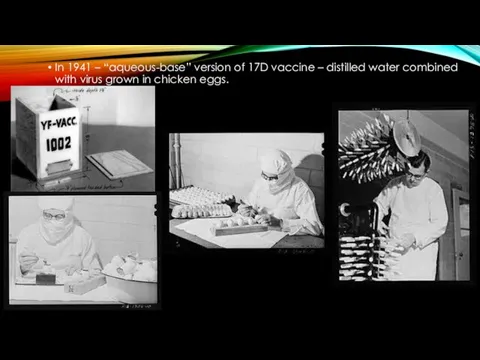
- 10. In 1941 – “aqueous-base” version of 17D vaccine – distilled water combined with virus grown in
- 12. PRESENT Currently available YF-vaccines (WHO prequalified) Bio-manguinhos, 17-DD, Brazil Sanofi Pasteur, Stamaril, 17D-204, France Pasteur Institute
- 13. Contraindiction Allergy to vaccine component (Egg protein) Age Symptomatic HIV infection/CD4+ counts Thymus disorder Primary immunodeficiencies
- 14. Common adverse events of YF Vaccines Fever, headache, backache 3-7 days after vaccination: 5-15% Injection site
- 15. WHO YF vaccines recommendations: SAGE formed YF Vaccine workgroup in 2011: Need for booster dose every
- 16. YF VACCINE ASSOCIATED DISEASE Neurogenic- due to direct viral invasion of CNS or auto-immune mediated, can
- 17. WHO EYE INITIATIVE “Eliminate Yellow Fever Epidemics” Aims to increase 17D vaccine manufacturing to distribute 1.3
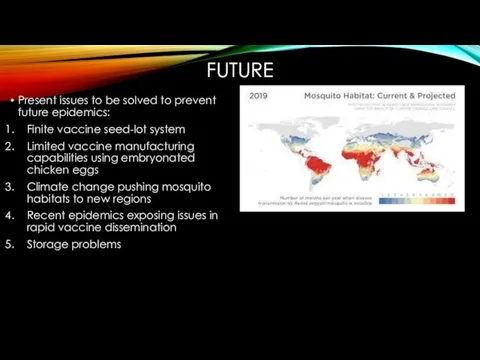
- 18. FUTURE Present issues to be solved to prevent future epidemics: Finite vaccine seed-lot system Limited vaccine
- 19. Solutions A more shelf-stable vaccine - more doses generated with fewer IU per dose YF-Vaccines in
- 21. Скачать презентацию
Слайд 2YELLOW FEVER VIRUS
Arbovirus
Family – Flaviviridae
Genus – Flavivirus
Single serotype
Reservoir - Monkeys
Vector – Aedes
YELLOW FEVER VIRUS
Arbovirus
Family – Flaviviridae
Genus – Flavivirus
Single serotype
Reservoir - Monkeys
Vector – Aedes
Слайд 3PAST
1912 – opening of Panama canal – increased global exposure – first
PAST
1912 – opening of Panama canal – increased global exposure – first

Слайд 4Hideyo Noguchi, a Japanese bacteriologist – worked for Rockefeller Foundation, Ecuador –
Hideyo Noguchi, a Japanese bacteriologist – worked for Rockefeller Foundation, Ecuador –
Слайд 5“French strain” – obtained from a survivor – another vaccine by Pasteur
“French strain” – obtained from a survivor – another vaccine by Pasteur
Слайд 6Attempts to attenuate – failed.
Another vaccine developed – derived from Asibi
Attempts to attenuate – failed.
Another vaccine developed – derived from Asibi
Слайд 7In 1937, Max Theiler (awarded the Nobel Prize in Physiology or Medicine
In 1937, Max Theiler (awarded the Nobel Prize in Physiology or Medicine
Слайд 8Theiler used chicken eggs to culture the virus.
Over 1 million people vaccinated
Theiler used chicken eggs to culture the virus.
Over 1 million people vaccinated
Слайд 9Theiler’s vaccine – largest outbreak of Hepatits B – 330,000
Theiler’s vaccine – largest outbreak of Hepatits B – 330,000

Слайд 10In 1941 – “aqueous-base” version of 17D vaccine – distilled water combined
In 1941 – “aqueous-base” version of 17D vaccine – distilled water combined

Слайд 12PRESENT
Currently available YF-vaccines (WHO prequalified)
Bio-manguinhos, 17-DD, Brazil
Sanofi Pasteur, Stamaril, 17D-204, France
Pasteur Institute
PRESENT
Currently available YF-vaccines (WHO prequalified)
Bio-manguinhos, 17-DD, Brazil
Sanofi Pasteur, Stamaril, 17D-204, France
Pasteur Institute
Слайд 13Contraindiction
Allergy to vaccine component (Egg protein)
Age < 6 months
Symptomatic HIV infection/CD4+ counts
Contraindiction
Allergy to vaccine component (Egg protein)
Age < 6 months
Symptomatic HIV infection/CD4+ counts
Слайд 14Common adverse events of YF Vaccines
Fever, headache, backache 3-7 days after vaccination:
Common adverse events of YF Vaccines
Fever, headache, backache 3-7 days after vaccination:

Слайд 15WHO YF vaccines recommendations:
SAGE formed YF Vaccine workgroup in 2011: Need for
WHO YF vaccines recommendations:
SAGE formed YF Vaccine workgroup in 2011: Need for
Слайд 16YF VACCINE ASSOCIATED DISEASE
Neurogenic- due to direct viral invasion of CNS or
YF VACCINE ASSOCIATED DISEASE
Neurogenic- due to direct viral invasion of CNS or
Слайд 17WHO EYE INITIATIVE
“Eliminate Yellow Fever Epidemics”
Aims to increase 17D vaccine manufacturing to
WHO EYE INITIATIVE
“Eliminate Yellow Fever Epidemics”
Aims to increase 17D vaccine manufacturing to
Слайд 18FUTURE
Present issues to be solved to prevent future epidemics:
Finite vaccine seed-lot system
Limited
FUTURE
Present issues to be solved to prevent future epidemics:
Finite vaccine seed-lot system
Limited
Слайд 19Solutions
A more shelf-stable vaccine - more doses generated with fewer IU
Solutions
A more shelf-stable vaccine - more doses generated with fewer IU
 Кровяные инфекции. Чума
Кровяные инфекции. Чума Пролапс митрального клапана и дизъюнкция. Оценка рисков ВСС
Пролапс митрального клапана и дизъюнкция. Оценка рисков ВСС Основы трансфузиологии
Основы трансфузиологии Биогенные амины. Ингибиторы МАО. Антигистаминные препараты
Биогенные амины. Ингибиторы МАО. Антигистаминные препараты МРТ диагностика компрессионной миелопатии, изменений интра - и эпидуральных пространств
МРТ диагностика компрессионной миелопатии, изменений интра - и эпидуральных пространств Токсикоз с эксикозом при кишечных инфекциях у детей
Токсикоз с эксикозом при кишечных инфекциях у детей Уреаплазмоз. Микоплазмоз
Уреаплазмоз. Микоплазмоз Врожденный сифилис. Лекция 7
Врожденный сифилис. Лекция 7 Дневник развития ребенка
Дневник развития ребенка ОВИН – диагноз исключения. Клинические примеры
ОВИН – диагноз исключения. Клинические примеры Сыроедение
Сыроедение Розвиток професійних хвороб зумовлений впливом на організм працівників шкідливих виробничих чинників
Розвиток професійних хвороб зумовлений впливом на організм працівників шкідливих виробничих чинників Глаукомы. Лекция 10
Глаукомы. Лекция 10 Периферический увеит
Периферический увеит Жеке даму биологиясы әдістері
Жеке даму биологиясы әдістері Избыточная масса тела. Ожирение
Избыточная масса тела. Ожирение Опухоли головного мозга
Опухоли головного мозга Паховая грыжа
Паховая грыжа Алкогольная полиневропатия
Алкогольная полиневропатия Простагландины. Функции, используемые для терапии
Простагландины. Функции, используемые для терапии Психофармакотерапия. Анксиолитики. Гипнотики
Психофармакотерапия. Анксиолитики. Гипнотики Роль гиперчувствительности замедленного типа в инфекционном процессе и нестерильном иммунитете
Роль гиперчувствительности замедленного типа в инфекционном процессе и нестерильном иммунитете О речевом развитии детей. Что должны знать родители
О речевом развитии детей. Что должны знать родители Эндокринология. Феохромоцитома
Эндокринология. Феохромоцитома Острая почечная недостаточность
Острая почечная недостаточность Поняття про артеріальний тиск
Поняття про артеріальний тиск Миеломенингоцеле. Знак лимона
Миеломенингоцеле. Знак лимона Үймереттердің ішкі суағары
Үймереттердің ішкі суағары