- Covid–19 thrombosis prophylaxis with rivaroxaban therapy

Содержание
- 2. FOR EDUARDO RAMACCIOTTI DECLARATION OF INTEREST
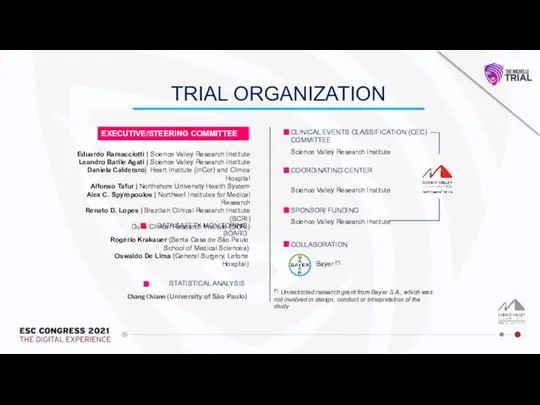
- 3. (*) Unrestricted research grant from Bayer S.A., which was not involved in design, conduct or interpretation
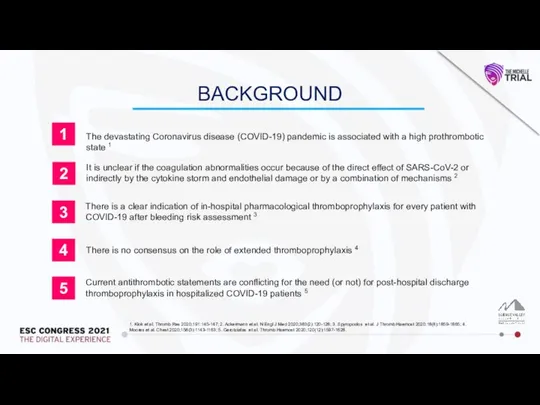
- 4. BACKGROUND The devastating Coronavirus disease (COVID-19) pandemic is associated with a high prothrombotic state 1 It
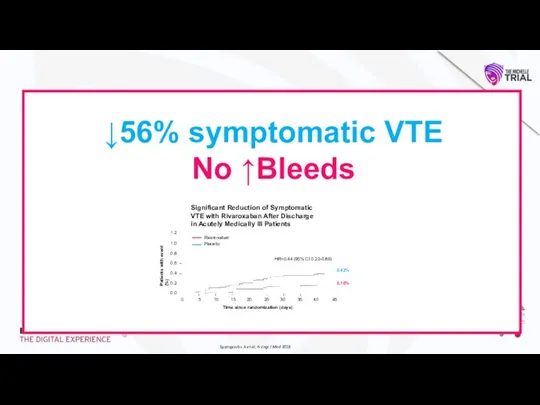
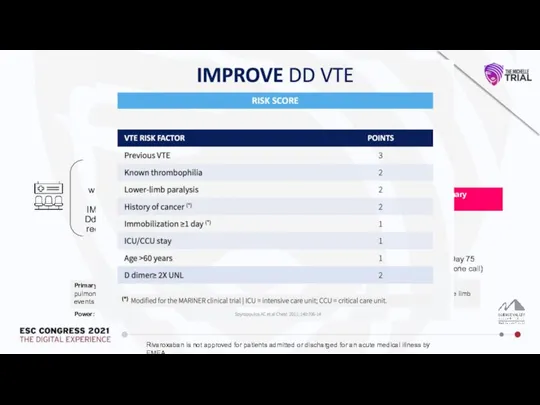
- 5. Spyropoulos A et al, N Engl J Med 2018 ↓56% symptomatic VTE No ↑Bleeds
- 6. Design: Prospective, randomized, open-label, controlled, multi-center trial No anticoagulation Rivaroxaban (10 mg/day) Day 35±4 R Day
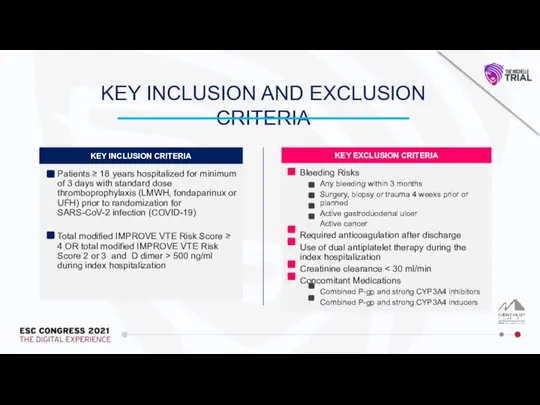
- 7. KEY INCLUSION AND EXCLUSION CRITERIA
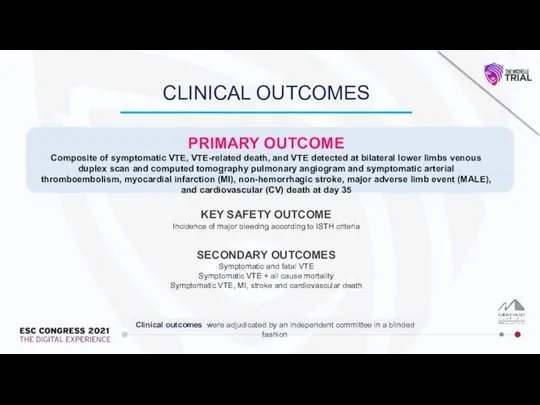
- 8. CLINICAL OUTCOMES PRIMARY OUTCOME Composite of symptomatic VTE, VTE-related death, and VTE detected at bilateral lower
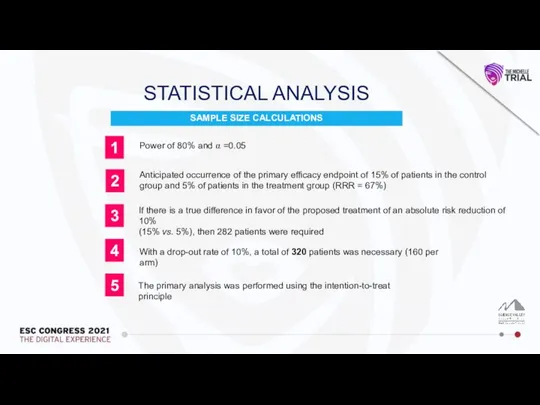
- 9. SAMPLE SIZE CALCULATIONS STATISTICAL ANALYSIS 2 1 3 5 4 Power of 80% and ⍺ =0.05
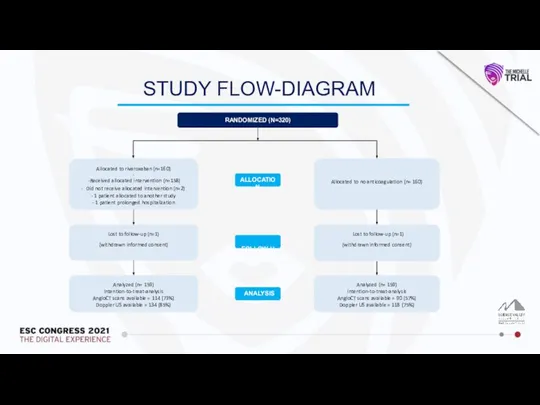
- 10. STUDY FLOW-DIAGRAM Analyzed (n= 159) Intention-to-treat-analysis AngioCT scans available = 114 (73%) Doppler US available =
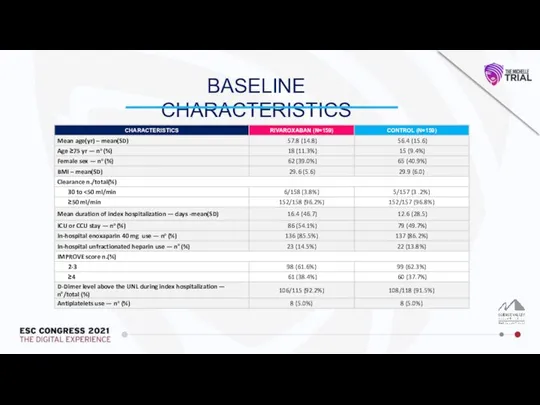
- 11. BASELINE CHARACTERISTICS
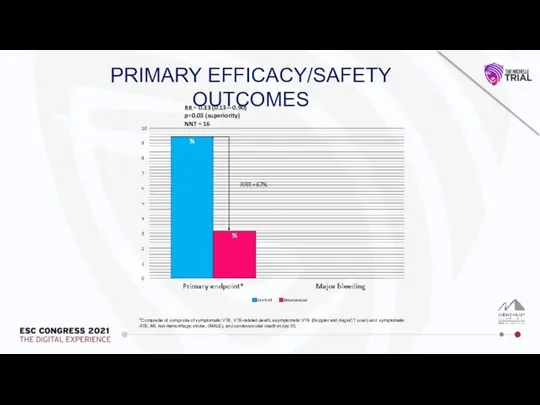
- 12. PRIMARY EFFICACY/SAFETY OUTCOMES *Composite of composite of symptomatic VTE, VTE-related death, asymptomatic VTE (Doppler and AngioCT
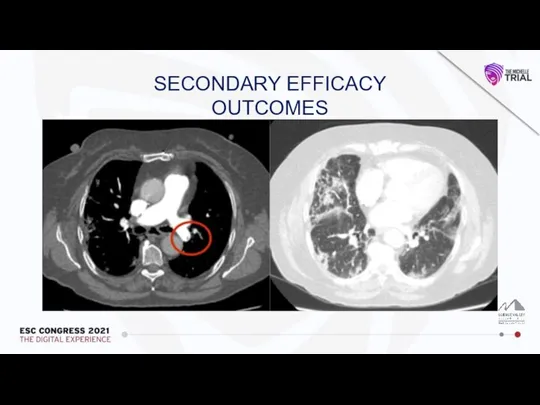
- 13. SECONDARY EFFICACY OUTCOMES
- 14. SECONDARY EFFICACY OUTCOMES
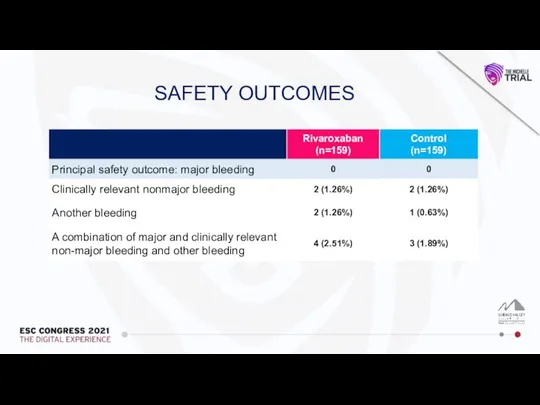
- 15. SAFETY OUTCOMES
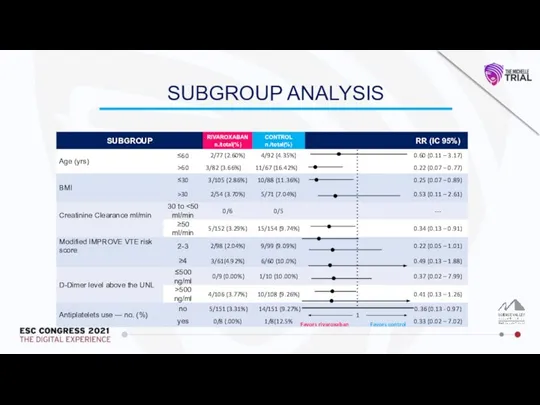
- 16. SUBGROUP ANALYSIS 1 Favors rivaroxaban Favors control
- 17. CONCLUSION In patients discharged after hospitalization due to COVID-19 with increased IMPROVE score, thromboprophylaxis with rivaroxaban
- 19. Скачать презентацию
Слайд 3(*) Unrestricted research grant from Bayer S.A., which was not involved in
(*) Unrestricted research grant from Bayer S.A., which was not involved in
Слайд 4BACKGROUND
The devastating Coronavirus disease (COVID-19) pandemic is associated with a high prothrombotic
BACKGROUND
The devastating Coronavirus disease (COVID-19) pandemic is associated with a high prothrombotic
Слайд 5Spyropoulos A et al, N Engl J Med 2018
↓56% symptomatic VTE
No
Spyropoulos A et al, N Engl J Med 2018
↓56% symptomatic VTE
No
Слайд 6Design: Prospective, randomized, open-label, controlled, multi-center trial
No anticoagulation
Rivaroxaban
(10 mg/day)
Day
Design: Prospective, randomized, open-label, controlled, multi-center trial
No anticoagulation
Rivaroxaban
(10 mg/day)
Day
Слайд 7KEY INCLUSION AND EXCLUSION CRITERIA
KEY INCLUSION AND EXCLUSION CRITERIA
Слайд 8CLINICAL OUTCOMES
PRIMARY OUTCOME
Composite of symptomatic VTE, VTE-related death, and VTE detected at
CLINICAL OUTCOMES
PRIMARY OUTCOME
Composite of symptomatic VTE, VTE-related death, and VTE detected at
Слайд 9SAMPLE SIZE CALCULATIONS
STATISTICAL ANALYSIS
2
1
3
5
4
Power of 80% and ⍺ =0.05
Anticipated occurrence of the
SAMPLE SIZE CALCULATIONS
STATISTICAL ANALYSIS
2
1
3
5
4
Power of 80% and ⍺ =0.05
Anticipated occurrence of the
Слайд 10STUDY FLOW-DIAGRAM
Analyzed (n= 159)
Intention-to-treat-analysis
AngioCT scans available = 114 (73%)
Doppler US available =
STUDY FLOW-DIAGRAM
Analyzed (n= 159)
Intention-to-treat-analysis
AngioCT scans available = 114 (73%)
Doppler US available =
Слайд 11BASELINE CHARACTERISTICS
BASELINE CHARACTERISTICS
Слайд 12PRIMARY EFFICACY/SAFETY OUTCOMES
*Composite of composite of symptomatic VTE, VTE-related death, asymptomatic VTE
PRIMARY EFFICACY/SAFETY OUTCOMES
*Composite of composite of symptomatic VTE, VTE-related death, asymptomatic VTE
Слайд 13SECONDARY EFFICACY OUTCOMES
SECONDARY EFFICACY OUTCOMES
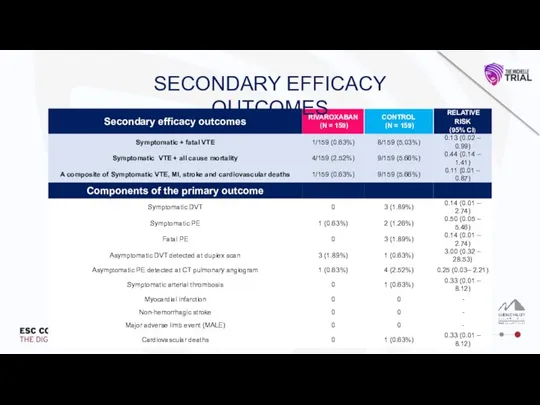
Слайд 14SECONDARY EFFICACY OUTCOMES
SECONDARY EFFICACY OUTCOMES
Слайд 15SAFETY OUTCOMES
SAFETY OUTCOMES
Слайд 16SUBGROUP ANALYSIS
1
Favors rivaroxaban
Favors control
SUBGROUP ANALYSIS
1
Favors rivaroxaban
Favors control
Слайд 17CONCLUSION
In patients discharged after hospitalization due to COVID-19 with increased IMPROVE score,
CONCLUSION
In patients discharged after hospitalization due to COVID-19 with increased IMPROVE score,
 Функциональная анатомия мышц и суставов туловища. Позвоночник
Функциональная анатомия мышц и суставов туловища. Позвоночник Строение синапса. Нейромедиаторы
Строение синапса. Нейромедиаторы Проблемы перегрузки железом
Проблемы перегрузки железом Кардиальные и внекардиальные эффекты СГ. Механизм систолического и диастолического действия
Кардиальные и внекардиальные эффекты СГ. Механизм систолического и диастолического действия Введение в иммунологию
Введение в иммунологию Основы реанимации новородженных
Основы реанимации новородженных Сестринский процесс при туберкулёзе лёгких
Сестринский процесс при туберкулёзе лёгких The Digestive system
The Digestive system Гипоксия. Занятие 10
Гипоксия. Занятие 10 ИММУНОПРОФИЛАКТИКА_Инфекционных заболеваний
ИММУНОПРОФИЛАКТИКА_Инфекционных заболеваний Опухоли головного мозга. Часть 1
Опухоли головного мозга. Часть 1 Синдром артериальной гипертензии в практике участкового терапевта. Современные принципы лечебно- диагностической тактики
Синдром артериальной гипертензии в практике участкового терапевта. Современные принципы лечебно- диагностической тактики Роль трансэзофагеальной эхокардиографии (ТЭЭ) в диагностике инфекционного эндокардита (ИЭ) и его осложнений
Роль трансэзофагеальной эхокардиографии (ТЭЭ) в диагностике инфекционного эндокардита (ИЭ) и его осложнений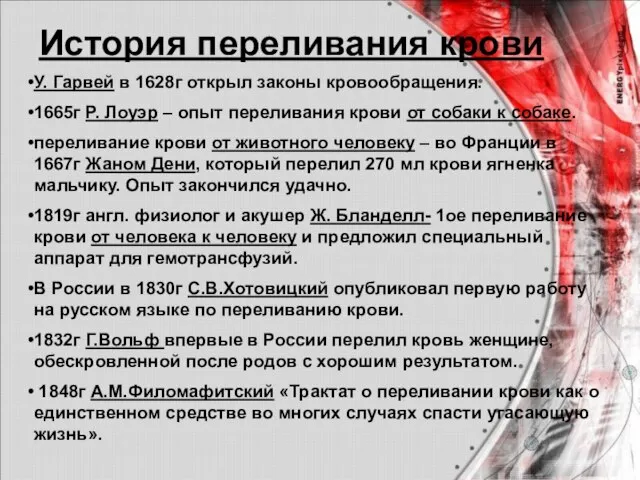 История переливания крови
История переливания крови Врачевание в первобытном обществе. Народное врачевание
Врачевание в первобытном обществе. Народное врачевание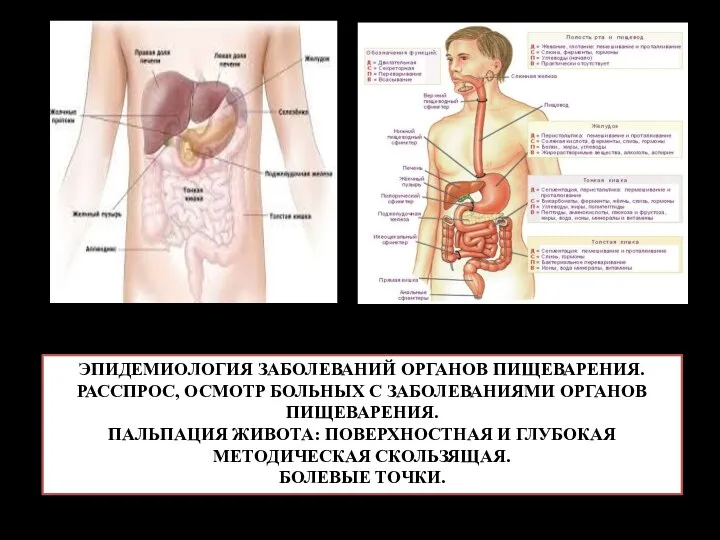 Эпидемиология заболеваний органов пищеварения. Расспрос, осмотр больных с заболеваниями органов пищеварения
Эпидемиология заболеваний органов пищеварения. Расспрос, осмотр больных с заболеваниями органов пищеварения Определение факторов риска, способствующих развитию гастрита среди подростков
Определение факторов риска, способствующих развитию гастрита среди подростков Измерение движений в суставах
Измерение движений в суставах Ожирение как образ жизни: путь к патологии
Ожирение как образ жизни: путь к патологии Імунна відповідь у нормі та при її порушення при найбільш поширених патологічних станах
Імунна відповідь у нормі та при її порушення при найбільш поширених патологічних станах Карієс у школярів різних вікових груп
Карієс у школярів різних вікових груп Жиры как питательные вещества
Жиры как питательные вещества ANCA-ассоциированные васкулиты
ANCA-ассоциированные васкулиты Лечебная физическая культура в комплексной реабилитации больных хроническими бронхитами
Лечебная физическая культура в комплексной реабилитации больных хроническими бронхитами Острый гломерулонефрит у детей
Острый гломерулонефрит у детей Этапы лечения хирургического больного. Предоперационный период. Хирургическая операция и её влияние на организм больного
Этапы лечения хирургического больного. Предоперационный период. Хирургическая операция и её влияние на организм больного Использование ксеноновых ингаляций для коррекции функционального состояния спортсменов
Использование ксеноновых ингаляций для коррекции функционального состояния спортсменов Туберкулез. Причины туберкулеза. Характеристика возбудителя. Профилактика и лечение
Туберкулез. Причины туберкулеза. Характеристика возбудителя. Профилактика и лечение