- Liver cirrhosis

Содержание
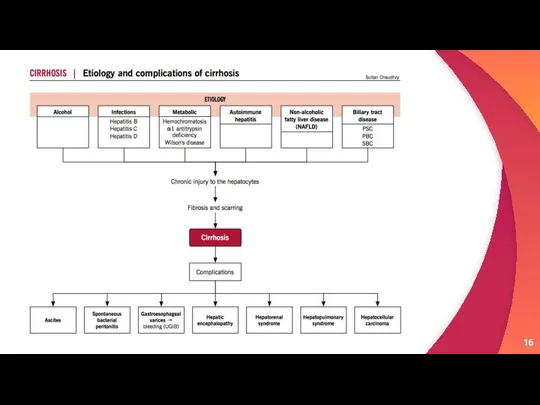
- 3. Liver cirrhosis is a chronic liver disease accompanied by irreversible replacement of parenchymal liver tissue by
- 4. Etiology Alcohol Hepatitis B can cause liver inflammation and damage that can lead to cirrhosis. Hepatitis
- 5. Damage to the bile ducts, which function to drain bile: One example of such a condition
- 6. Classification 1
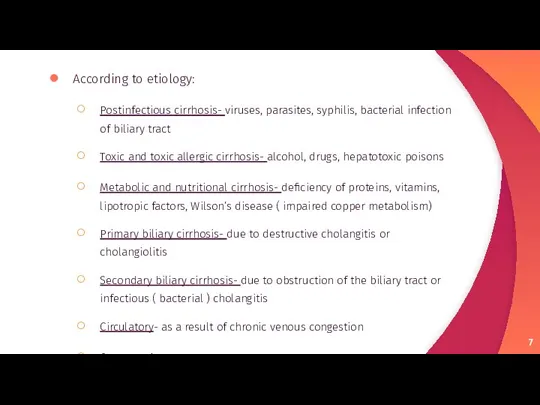
- 7. According to etiology: Postinfectious cirrhosis- viruses, parasites, syphilis, bacterial infection of biliary tract Toxic and toxic
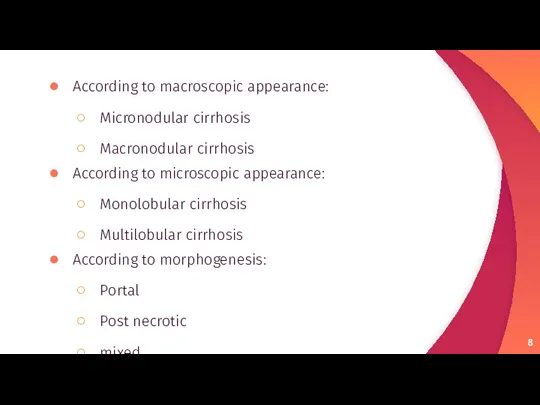
- 8. According to macroscopic appearance: Micronodular cirrhosis Macronodular cirrhosis According to microscopic appearance: Monolobular cirrhosis Multilobular cirrhosis
- 9. According to course: Active Inactive
- 10. Pathogenesis 2
- 12. Irrespective of the aetiology, cirrhosis in general is initiated by hepatocellular necrosis Replacement of BM collagen
- 13. ECM regulates cellular activity and availability of growth factors Decorin and biglycan binds TGF-B Fibronectin and
- 14. HSC activation represents a critical event in the fibrosis This cell become the primary source of
- 15. Sources of ECM HSC Bone marrow derive cells Epithelial mesenchymal transition Portal fibroblast
- 17. CYTOKINES AND SIGNALING PATHWAYS Inflammatory cytokines play a key role in fibrosis, given that persistent inflammation
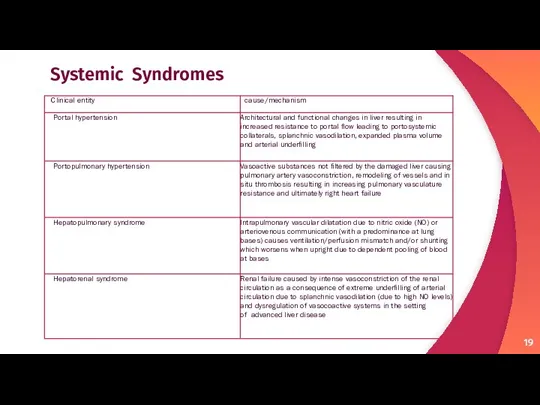
- 19. Systemic Syndromes
- 20. Clinical Features 3
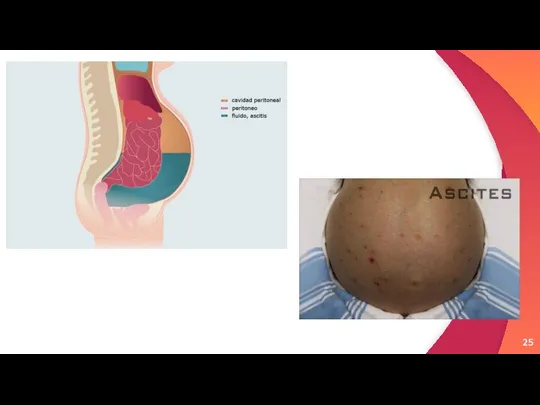
- 21. More serious symptoms include: confusion and difficulty thinking clearly abdominal swelling (ascites) swelling of the legs
- 22. Liver dysfunction The following features are a direct consequence of liver cells not functioning. Spider angiomata
- 23. Spider angiomata Palmnar Erythema
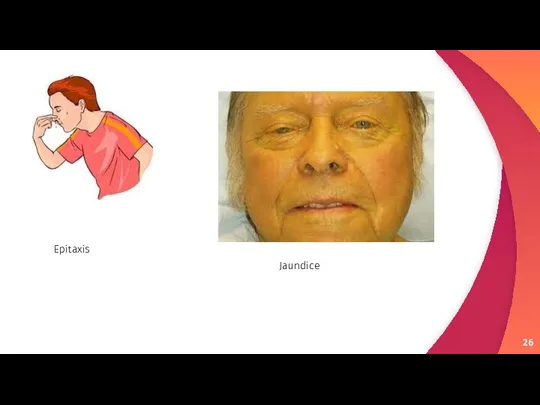
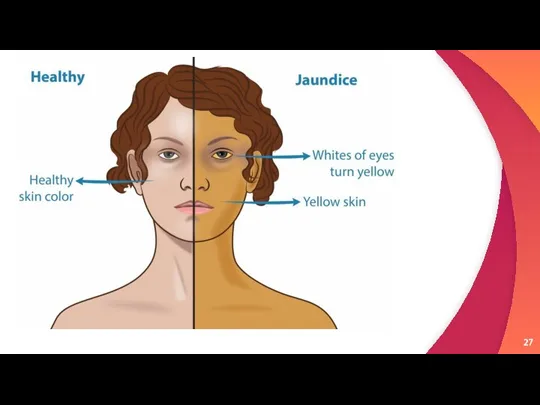
- 26. Epitaxis Jaundice
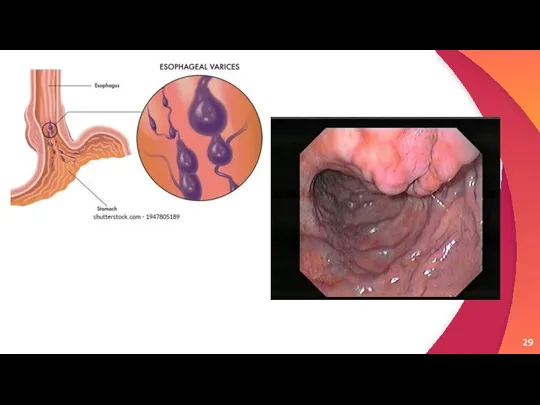
- 28. Portal hypertension Liver cirrhosis increases resistance to blood flow and leads to higher pressure in the
- 31. Advanced disease As the disease progresses, complications may develop. In some people, these may be the
- 32. Bruising Cachexic patient with jaundice
- 33. Lab findings The following findings are typical in cirrhosis: Thrombocytopenia – typically multifactorial. Due to alcoholic
- 34. Prothrombin time – increases, since the liver synthesizes clotting factors. Globulins – increased due to shunting
- 35. Other laboratory studies performed in newly diagnosed cirrhosis may include: Serology for hepatitis viruses, autoantibodies (ANA,
- 36. Liver ultrasound to assess the severity of cirrhosis. Liver biopsy to identify liver cell changes &
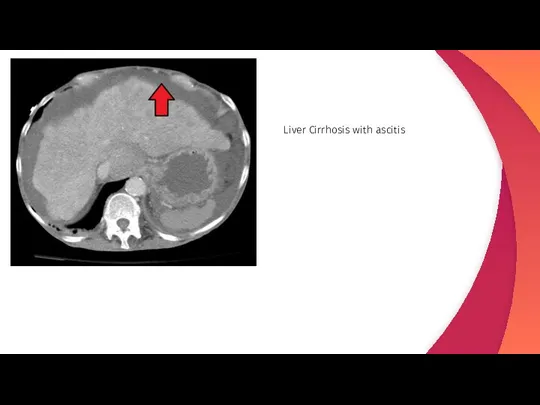
- 37. Liver Cirrhosis with ascitis
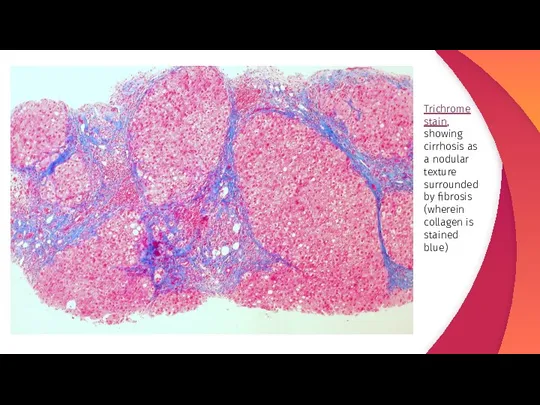
- 38. Trichrome stain, showing cirrhosis as a nodular texture surrounded by fibrosis (wherein collagen is stained blue)
- 39. Treatment & Prevention 3
- 40. Treatment for cirrhosis varies based on what caused it and how far the disorder has progressed.
- 41. Practicing sex with a barrier method can reduce the risk of getting hepatitis B or C.
- 43. Скачать презентацию

Слайд 3Liver cirrhosis is a chronic liver disease accompanied by irreversible replacement of
Liver cirrhosis is a chronic liver disease accompanied by irreversible replacement of
Слайд 4 Etiology
Alcohol
Hepatitis B can cause liver inflammation and damage that can
Etiology
Alcohol
Hepatitis B can cause liver inflammation and damage that can
Слайд 5Damage to the bile ducts, which function to drain bile: One example
Damage to the bile ducts, which function to drain bile: One example
Слайд 6Classification
1
Classification
1
Слайд 7According to etiology:
Postinfectious cirrhosis- viruses, parasites, syphilis, bacterial infection of biliary tract
Toxic
According to etiology:
Postinfectious cirrhosis- viruses, parasites, syphilis, bacterial infection of biliary tract
Toxic
Слайд 8According to macroscopic appearance:
Micronodular cirrhosis
Macronodular cirrhosis
According to microscopic appearance:
Monolobular cirrhosis
Multilobular
According to macroscopic appearance:
Micronodular cirrhosis
Macronodular cirrhosis
According to microscopic appearance:
Monolobular cirrhosis
Multilobular
Слайд 9According to course:
Active
Inactive
According to course:
Active
Inactive

Слайд 10 Pathogenesis
2
Pathogenesis
2
Слайд 12Irrespective of the aetiology, cirrhosis in general is initiated by hepatocellular necrosis
Irrespective of the aetiology, cirrhosis in general is initiated by hepatocellular necrosis
Слайд 13ECM regulates cellular activity and availability of growth factors
Decorin and biglycan
ECM regulates cellular activity and availability of growth factors
Decorin and biglycan
Слайд 14HSC activation represents a critical event in the fibrosis
This cell become
HSC activation represents a critical event in the fibrosis
This cell become
Слайд 15Sources of ECM
HSC
Bone marrow derive cells
Epithelial mesenchymal transition
Portal
Sources of ECM
HSC
Bone marrow derive cells
Epithelial mesenchymal transition
Portal
Слайд 17CYTOKINES AND SIGNALING PATHWAYS
Inflammatory cytokines play a key role in fibrosis, given
CYTOKINES AND SIGNALING PATHWAYS
Inflammatory cytokines play a key role in fibrosis, given
Слайд 19 Systemic Syndromes
Systemic Syndromes
Слайд 20Clinical Features
3
Clinical Features
3
Слайд 21 More serious symptoms include:
confusion and difficulty thinking clearly
abdominal swelling (ascites)
swelling of the
More serious symptoms include:
confusion and difficulty thinking clearly
abdominal swelling (ascites)
swelling of the
Слайд 22
Liver dysfunction
The following features are a direct consequence of liver cells
Liver dysfunction
The following features are a direct consequence of liver cells
Слайд 23Spider angiomata
Palmnar Erythema
Spider angiomata
Palmnar Erythema

Слайд 26Epitaxis
Jaundice
Epitaxis
Jaundice
Слайд 28
Portal hypertension
Liver cirrhosis increases resistance to blood flow and leads to higher
Portal hypertension
Liver cirrhosis increases resistance to blood flow and leads to higher

Слайд 31
Advanced disease
As the disease progresses, complications may develop. In some people, these
Advanced disease
As the disease progresses, complications may develop. In some people, these
Слайд 32Bruising
Cachexic patient with jaundice
Bruising
Cachexic patient with jaundice

Слайд 33
Lab findings
The following findings are typical in cirrhosis:
Thrombocytopenia – typically multifactorial. Due to
Lab findings
The following findings are typical in cirrhosis:
Thrombocytopenia – typically multifactorial. Due to
Слайд 34Prothrombin time – increases, since the liver synthesizes clotting factors.
Globulins – increased due to
Prothrombin time – increases, since the liver synthesizes clotting factors.
Globulins – increased due to
Слайд 35Other laboratory studies performed in newly diagnosed cirrhosis may include:
Serology for hepatitis viruses, autoantibodies (ANA, anti-smooth
Other laboratory studies performed in newly diagnosed cirrhosis may include:
Serology for hepatitis viruses, autoantibodies (ANA, anti-smooth
Слайд 36Liver ultrasound to assess the severity of cirrhosis.
Liver biopsy to identify
Liver ultrasound to assess the severity of cirrhosis.
Liver biopsy to identify
Слайд 37Liver Cirrhosis with ascitis
Liver Cirrhosis with ascitis
Слайд 38Trichrome stain, showing cirrhosis as a nodular texture surrounded by fibrosis (wherein
Trichrome stain, showing cirrhosis as a nodular texture surrounded by fibrosis (wherein
Слайд 39 Treatment & Prevention
3
Treatment & Prevention
3
Слайд 40Treatment for cirrhosis varies based on what caused it and how far
Слайд 41Practicing sex with a barrier method can reduce the risk of getting
Practicing sex with a barrier method can reduce the risk of getting
 Эпителиальные ткани железы
Эпителиальные ткани железы Особенности течения и распространения болезней печени и желчных путей. Гепатиты разных видов животных (лекция № 15)
Особенности течения и распространения болезней печени и желчных путей. Гепатиты разных видов животных (лекция № 15) Тепловая защита новорожденного
Тепловая защита новорожденного Культевые штифтовые вкладки Pentron под металлокерамику
Культевые штифтовые вкладки Pentron под металлокерамику Инвалидность и социальная политика. Анализ ситуации
Инвалидность и социальная политика. Анализ ситуации Клинико-фармакологическая характеристика лекарственных средств, применяемых при сахарном диабете
Клинико-фармакологическая характеристика лекарственных средств, применяемых при сахарном диабете Физкультминутка для глаз
Физкультминутка для глаз ГИПЕРТЕНЗИЯ (2 часть)
ГИПЕРТЕНЗИЯ (2 часть) Ветряная оспа, ветрянка
Ветряная оспа, ветрянка Дефекты длинных трубчатых костей и укорочение конечности
Дефекты длинных трубчатых костей и укорочение конечности Работа с людьми с последствиями детского церебрального паралича (ДЦП)
Работа с людьми с последствиями детского церебрального паралича (ДЦП) Профилактические мероприятия в организациях отдыха детей и их оздоровления в условиях сохранения рисков распространения COVID-19
Профилактические мероприятия в организациях отдыха детей и их оздоровления в условиях сохранения рисков распространения COVID-19 Узкий таз в акушерстве
Узкий таз в акушерстве Лечение скрытого апроксимального кариеса зуба
Лечение скрытого апроксимального кариеса зуба Организация медицинского страхования в РФ
Организация медицинского страхования в РФ Я думаю, что с ребенком что-то не так: куда обратиться?
Я думаю, что с ребенком что-то не так: куда обратиться? Поликистозная болезнь почек
Поликистозная болезнь почек Миокард инфаркты кезіндегі клиникалық
Миокард инфаркты кезіндегі клиникалық Искусственный интеллект в медицине
Искусственный интеллект в медицине Оценка статистической значимости выявленной связи между исходом и фактором риска клинического течения беременности и родов
Оценка статистической значимости выявленной связи между исходом и фактором риска клинического течения беременности и родов Грипп - острая вирусная инфекционная болезнь
Грипп - острая вирусная инфекционная болезнь Модернизация амбулаторно-поликлинической помощи
Модернизация амбулаторно-поликлинической помощи Условно рассасывающиеся шовные материалы
Условно рассасывающиеся шовные материалы Деменция с тельцами Леви
Деменция с тельцами Леви Часто задаваемые вопросы о вакцинации
Часто задаваемые вопросы о вакцинации От проективной геометрии – к неевклидовой (вокруг абсолюта). Перспектива
От проективной геометрии – к неевклидовой (вокруг абсолюта). Перспектива Mikrobiota_cheloveka
Mikrobiota_cheloveka Ревматоидный артрит
Ревматоидный артрит