- _____МЖ__ новый_17 apr_connent

Содержание
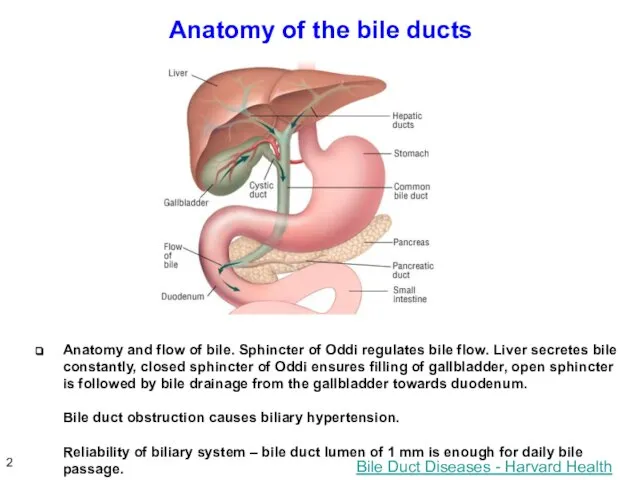
- 2. Anatomy of the bile ducts Bile Duct Diseases - Harvard Health Anatomy and flow of bile.
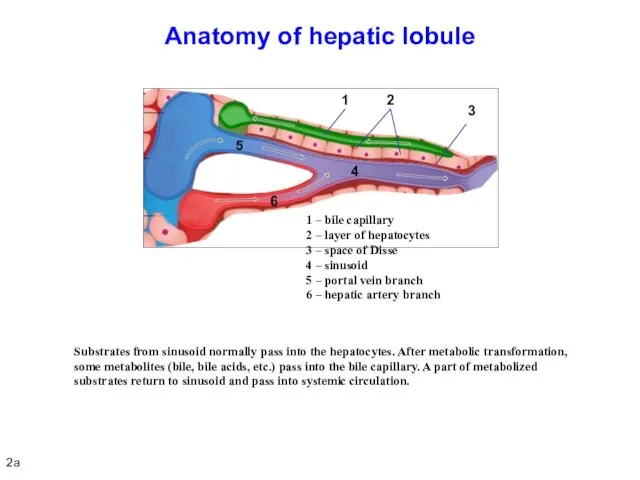
- 3. Anatomy of hepatic lobule Substrates from sinusoid normally pass into the hepatocytes. After metabolic transformation, some
- 4. Definition: any impairment of secretion and release of bile from the hepatocyte to the major duodenal
- 5. Cholemia Homeostasis disorders: vascular dilatation, reduced peripheral vascular resistance and total blood volume, bradycardia, vagal effects,
- 6. Painful and painless obstructive jaundice Various rates of biliary hypertension development (fast, sudden or slow, gradual)
- 7. PAINFUL OBSTRUCTIVE JAUNDICE 5
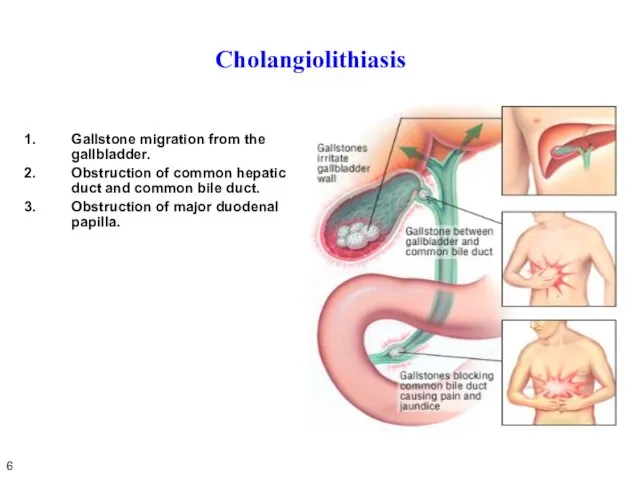
- 8. Cholangiolithiasis Gallstone migration from the gallbladder. Obstruction of common hepatic duct and common bile duct. Obstruction
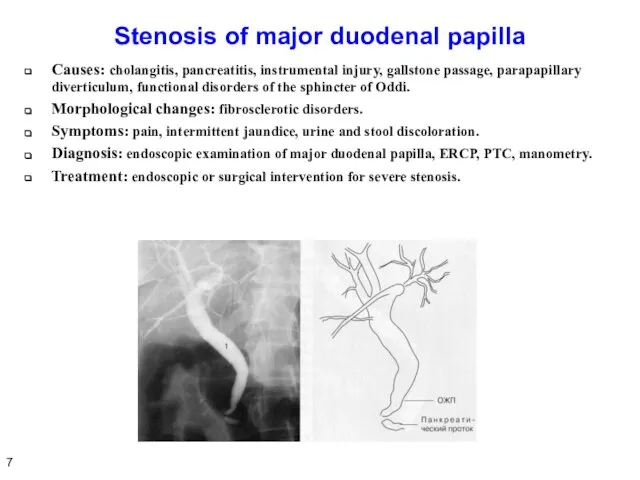
- 9. Stenosis of major duodenal papilla Causes: cholangitis, pancreatitis, instrumental injury, gallstone passage, parapapillary diverticulum, functional disorders
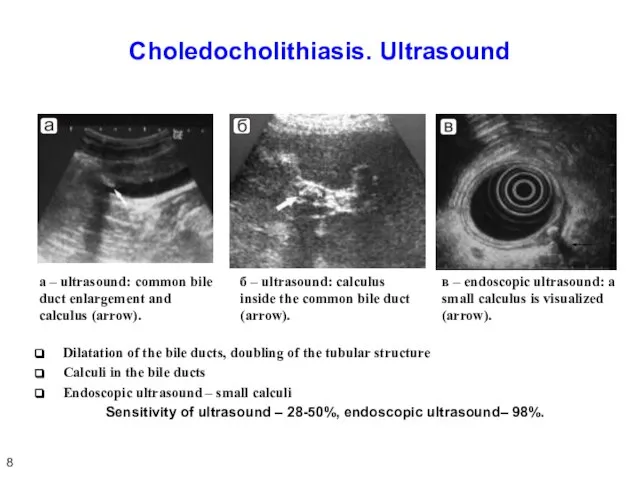
- 10. Choledocholithiasis. Ultrasound Dilatation of the bile ducts, doubling of the tubular structure Calculi in the bile
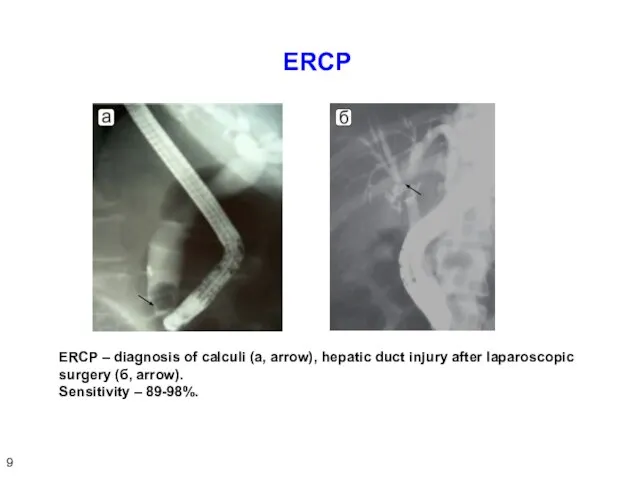
- 11. ERCP ERCP – diagnosis of calculi (а, arrow), hepatic duct injury after laparoscopic surgery (б, arrow).
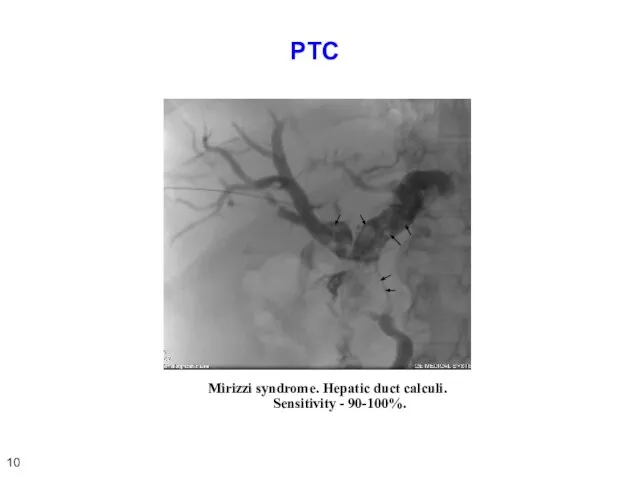
- 12. PTC Mirizzi syndrome. Hepatic duct calculi. Sensitivity - 90-100%. 10
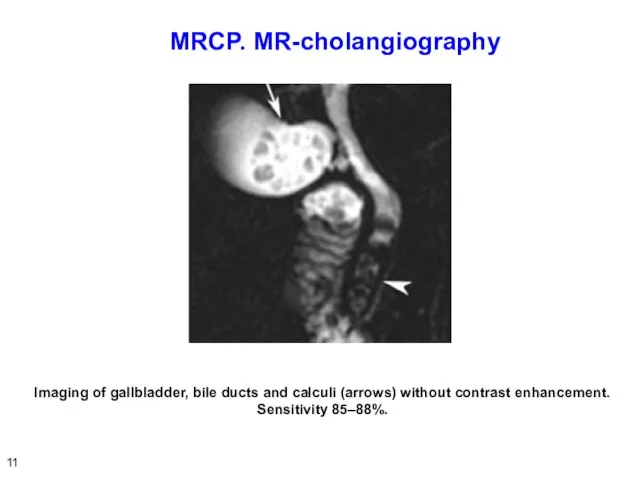
- 13. MRCP. МR-cholangiography Imaging of gallbladder, bile ducts and calculi (arrows) without contrast enhancement. Sensitivity 85–88%. 11
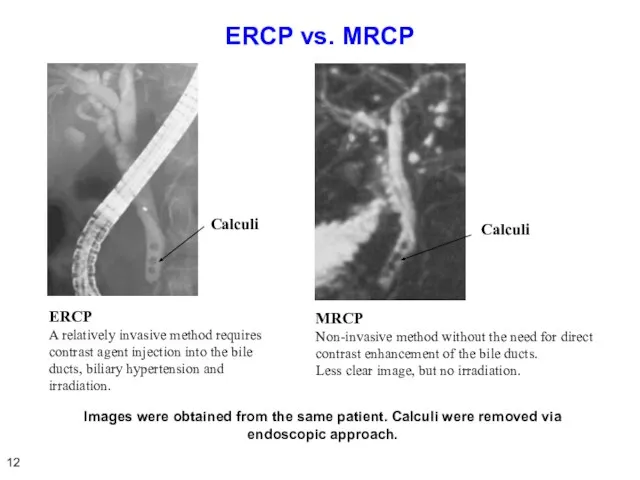
- 14. ERCP vs. MRCP ERCP A relatively invasive method requires contrast agent injection into the bile ducts,
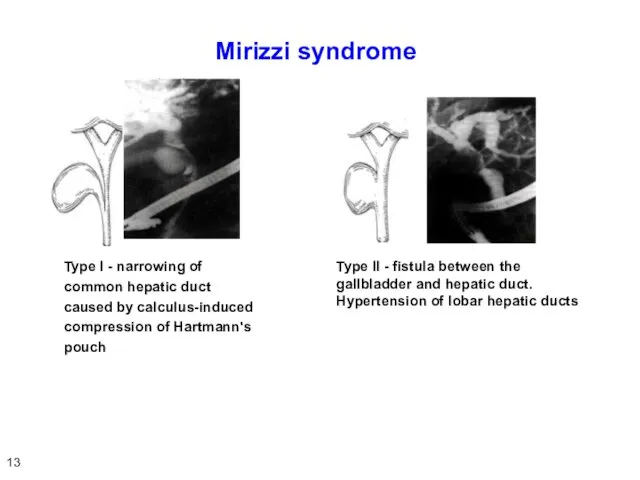
- 15. Mirizzi syndrome Type I - narrowing of common hepatic duct caused by calculus-induced compression of Hartmann's
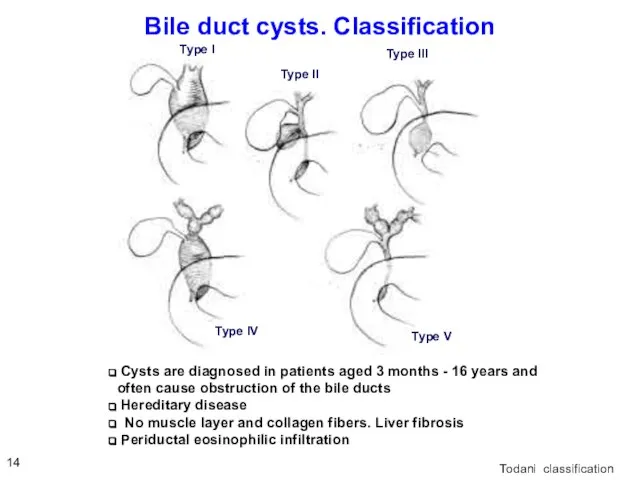
- 16. Bile duct cysts. Classification Todani classification Cysts are diagnosed in patients aged 3 months - 16
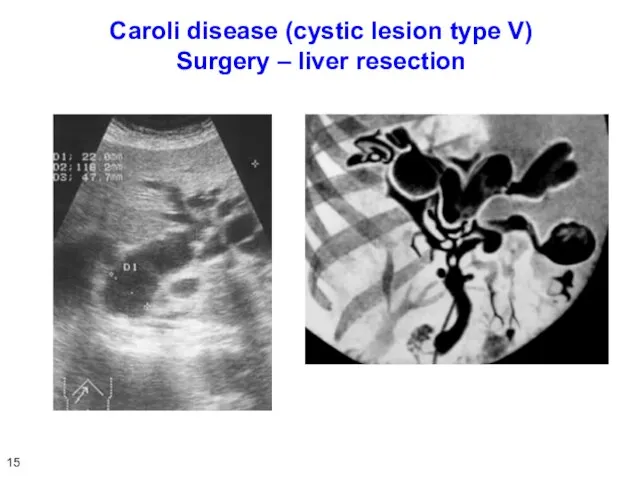
- 17. Caroli disease (cystic lesion type V) Surgery – liver resection 15
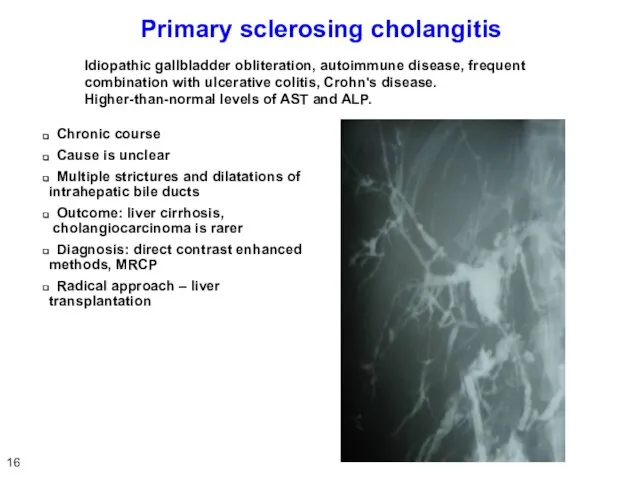
- 18. Primary sclerosing cholangitis Chronic course Cause is unclear Multiple strictures and dilatations of intrahepatic bile ducts
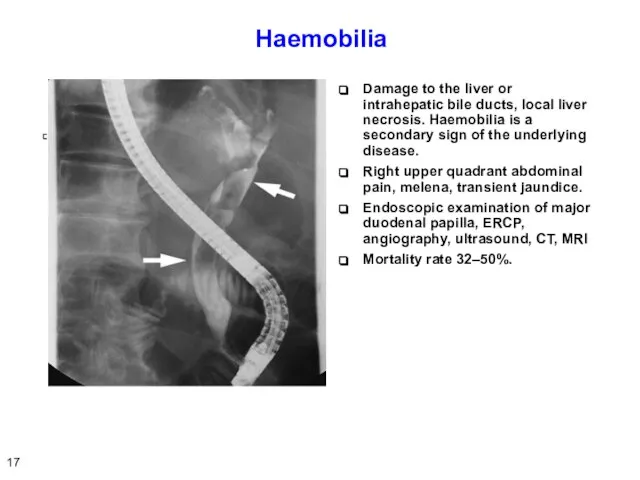
- 19. Haemobilia Damage to the liver or intrahepatic bile ducts, local liver necrosis. Haemobilia is a secondary
- 20. Parasitic invasion Opisthorchiasis (Ob, Volga basin, East Asia) Echinococcosis, alveococcosis, ascariasis, Fascioliasis– Fasciola gigantica Schistosomiasis –
- 21. Symptoms and diagnosis of painful obstructive jaundice Acute onset Scleral icterus Pain attack Dark urine, stool
- 22. ACUTE CHOLANGITIS 20
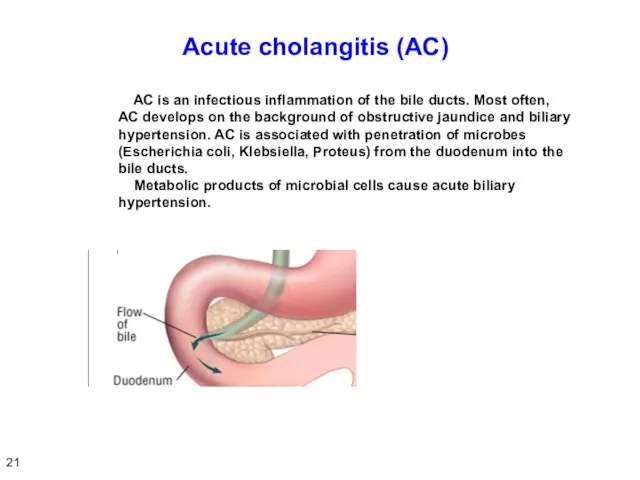
- 23. Acute cholangitis (AC) AC is an infectious inflammation of the bile ducts. Most often, AC develops
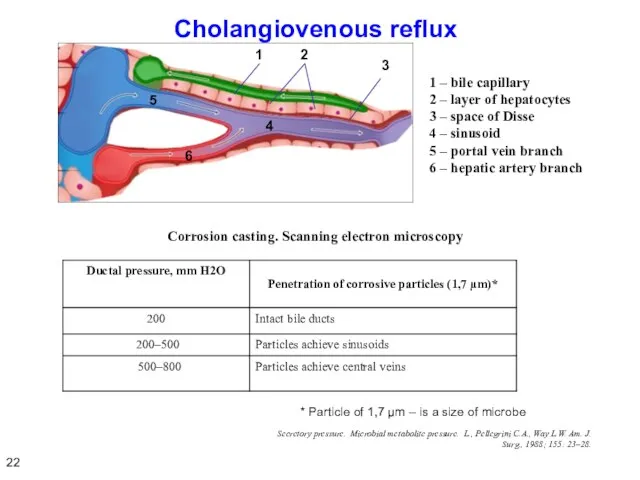
- 24. Cholangiovenous reflux Corrosion casting. Scanning electron microscopy Secretory pressure. Microbial metabolite pressure. L., Pellegrini C.A., Way
- 25. Symptoms of acute cholangitis Chills, fever Leukocytosis Infection Symptoms associated with biliary hypertension and obstructive jaundice
- 26. Causes of short-term SIRS and symptoms of sepsis Two factors: Large purulent surface of gallbladder, direct
- 27. Criteria of SIRS and sepsis Body temperature > 38ºC or Heart rate > 90 beats per
- 28. Organ dysfunction criteria CVS – hypotension requiring dopamine support CNS – impaired consciousness Respiratory system –
- 29. Renal failure in acute cholangitis Kidney is a main organ secreting bile components – cholemic nephropathy.
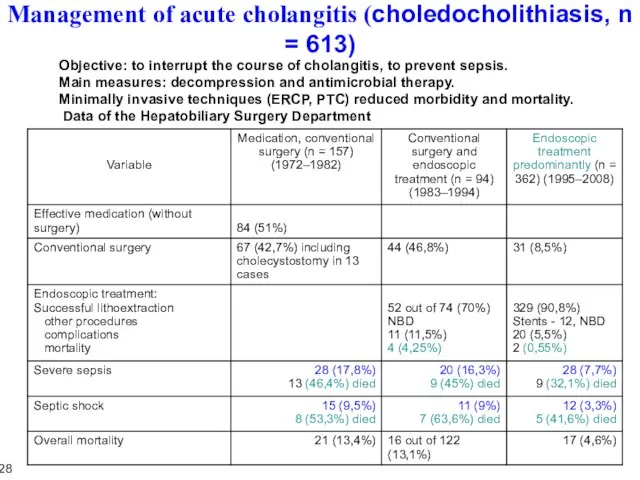
- 30. Management of acute cholangitis (choledocholithiasis, n = 613) Objective: to interrupt the course of cholangitis, to
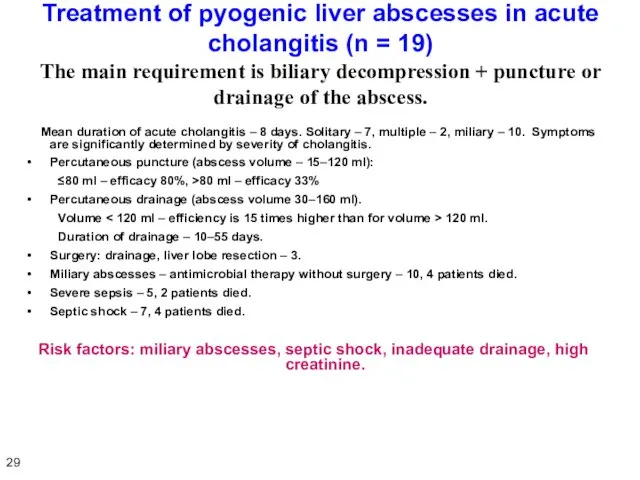
- 31. Treatment of pyogenic liver abscesses in acute cholangitis (n = 19) The main requirement is biliary
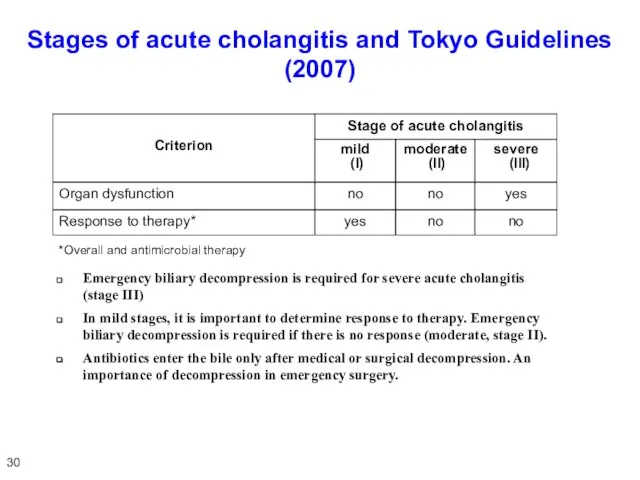
- 32. Stages of acute cholangitis and Tokyo Guidelines (2007) *Overall and antimicrobial therapy Emergency biliary decompression is
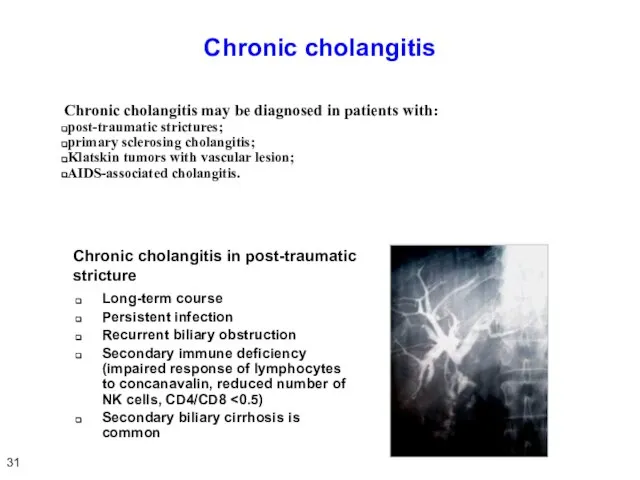
- 33. Chronic cholangitis Chronic cholangitis may be diagnosed in patients with: post-traumatic strictures; primary sclerosing cholangitis; Klatskin
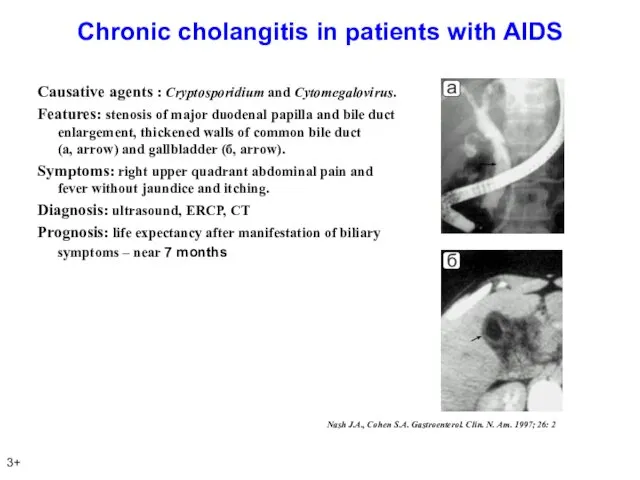
- 34. Chronic cholangitis in patients with AIDS Causative agents : Cryptosporidium and Cytomegalovirus. Features: stenosis of major
- 35. Conclusion Acute cholangitis is characterized by purulent process proceeding on the background of cholemia and acholia
- 36. PAINLESS OBSTRUCTIVE JAUNDICE 35
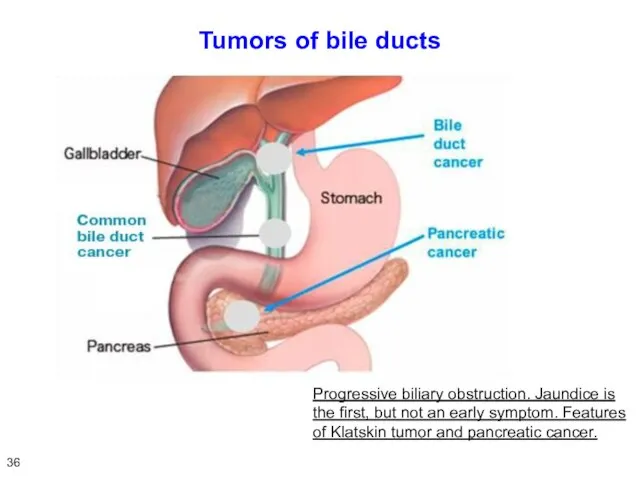
- 37. Tumors of bile ducts Progressive biliary obstruction. Jaundice is the first, but not an early symptom.
- 38. Symptoms of painless obstructive jaundice Icteric sclera and skin Itching Dark urine and stool discoloration No
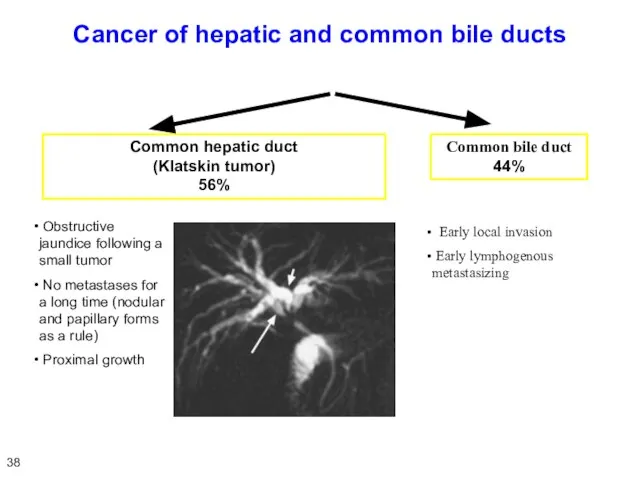
- 39. Cancer of hepatic and common bile ducts Common hepatic duct (Klatskin tumor) 56% Common bile duct
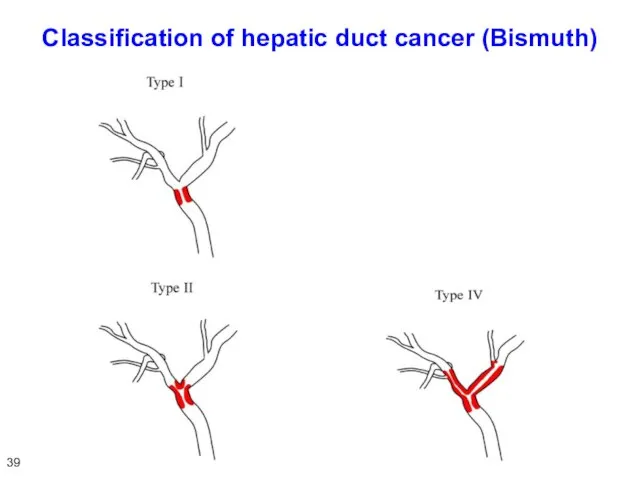
- 40. Classification of hepatic duct cancer (Bismuth) 39
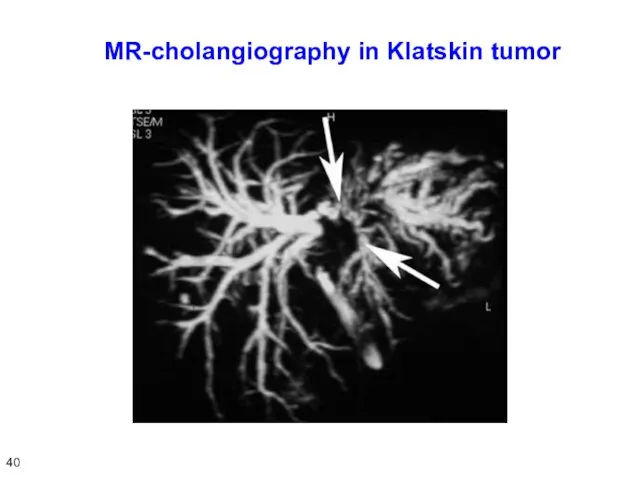
- 41. MR-cholangiography in Klatskin tumor 40
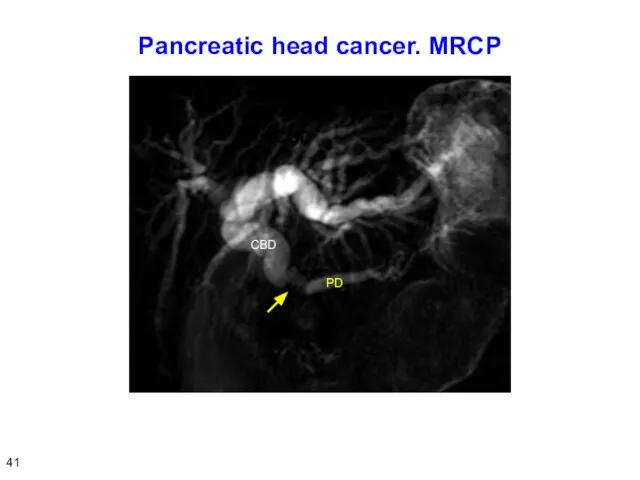
- 42. Pancreatic head cancer. MRCP 41
- 43. Differential diagnosis of obstructive and parenchymatous jaundice Patients with a painless obstructive jaundice do not notice
- 44. Functional and morphological features of liver in painless obstructive jaundice Increased levels of direct and indirect
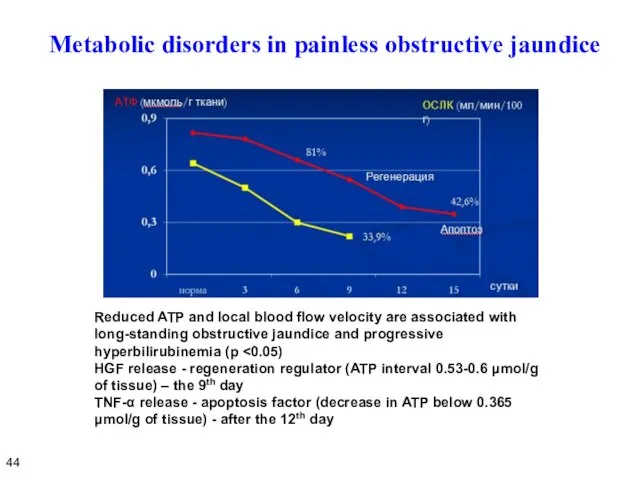
- 45. Metabolic disorders in painless obstructive jaundice Reduced ATP and local blood flow velocity are associated with
- 46. Conclusion on disorders arising in painless obstructive jaundice Painless obstructive jaundice causes severe functional and morphological
- 47. PREOPERATIVE DECOMPRESSION 46
- 48. Preoperative decompression of the bile ducts Methods of preoperative biliary decompression: Percutaneous cholangiostomy. Endoscopic nasobiliary drainage
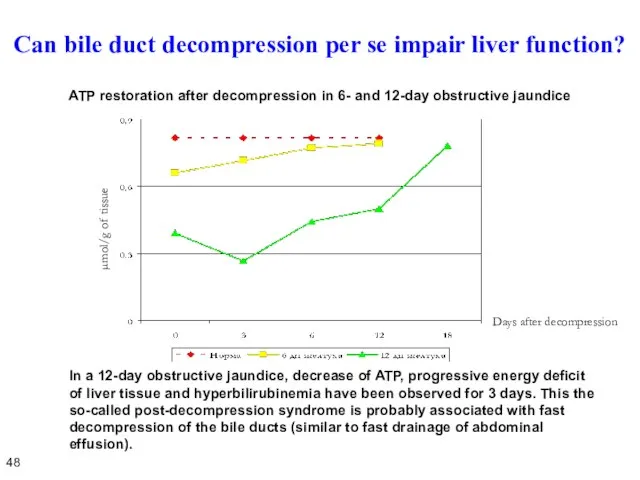
- 49. Can bile duct decompression per se impair liver function? In a 12-day obstructive jaundice, decrease of
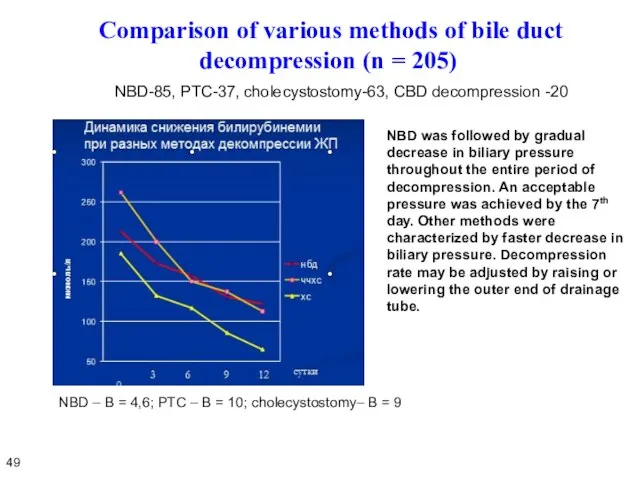
- 50. Comparison of various methods of bile duct decompression (n = 205) NBD-85, PTC-37, cholecystostomy-63, CBD decompression
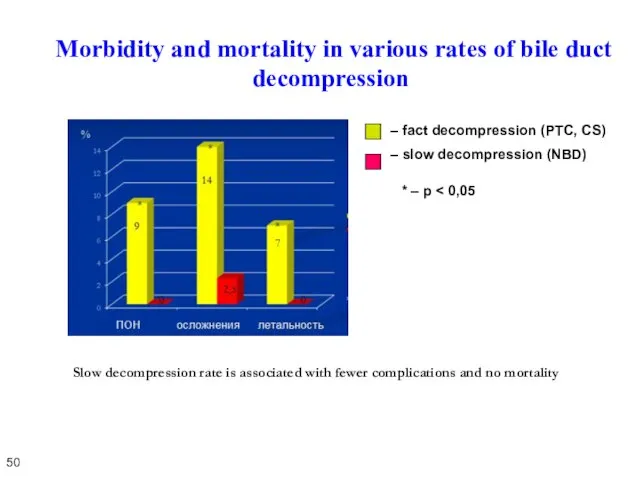
- 51. Morbidity and mortality in various rates of bile duct decompression * – p Slow decompression rate
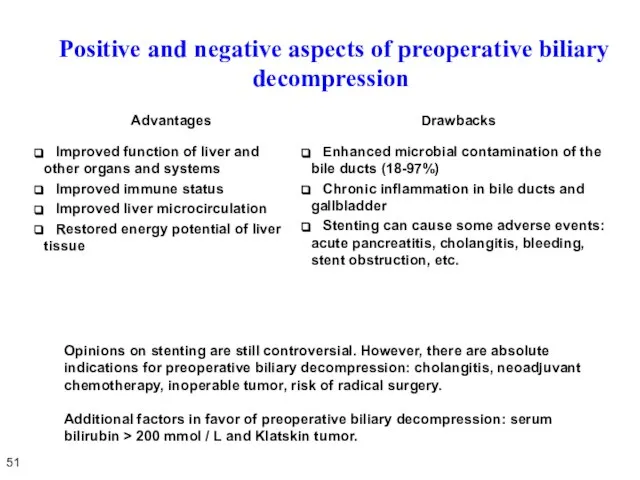
- 52. Positive and negative aspects of preoperative biliary decompression 51 Opinions on stenting are still controversial. However,
- 53. Features of preoperative biliary decompression in Klatskin tumor 52 Radical surgery for Klatskin tumor implies extended
- 55. Скачать презентацию
Слайд 3Anatomy of hepatic lobule
Substrates from sinusoid normally pass into the hepatocytes. After
Anatomy of hepatic lobule
Substrates from sinusoid normally pass into the hepatocytes. After
Слайд 4Definition: any impairment of secretion and release of bile from the hepatocyte
Definition: any impairment of secretion and release of bile from the hepatocyte
Слайд 5Cholemia
Homeostasis disorders: vascular dilatation, reduced peripheral vascular resistance and total blood volume,
Cholemia
Homeostasis disorders: vascular dilatation, reduced peripheral vascular resistance and total blood volume,
Слайд 6Painful and painless obstructive jaundice
Various rates of biliary hypertension development (fast, sudden
Painful and painless obstructive jaundice
Various rates of biliary hypertension development (fast, sudden
Слайд 7PAINFUL OBSTRUCTIVE JAUNDICE
5
PAINFUL OBSTRUCTIVE JAUNDICE
5
Слайд 8Cholangiolithiasis
Gallstone migration from the gallbladder.
Obstruction of common hepatic duct and common bile
Cholangiolithiasis
Gallstone migration from the gallbladder.
Obstruction of common hepatic duct and common bile
Слайд 9Stenosis of major duodenal papilla
Causes: cholangitis, pancreatitis, instrumental injury, gallstone passage, parapapillary
Stenosis of major duodenal papilla
Causes: cholangitis, pancreatitis, instrumental injury, gallstone passage, parapapillary
Слайд 10Choledocholithiasis. Ultrasound
Dilatation of the bile ducts, doubling of the tubular structure
Calculi in
Choledocholithiasis. Ultrasound
Dilatation of the bile ducts, doubling of the tubular structure
Calculi in
Слайд 11ERCP
ERCP – diagnosis of calculi (а, arrow), hepatic duct injury after laparoscopic
ERCP
ERCP – diagnosis of calculi (а, arrow), hepatic duct injury after laparoscopic
Слайд 12PTC
Mirizzi syndrome. Hepatic duct calculi.
Sensitivity - 90-100%.
10
PTC
Mirizzi syndrome. Hepatic duct calculi.
Sensitivity - 90-100%.
10
Слайд 13MRCP. МR-cholangiography
Imaging of gallbladder, bile ducts and calculi (arrows) without contrast enhancement.
Sensitivity
MRCP. МR-cholangiography
Imaging of gallbladder, bile ducts and calculi (arrows) without contrast enhancement. Sensitivity
Слайд 14ERCP vs. MRCP
ERCP
A relatively invasive method requires contrast agent injection into
ERCP vs. MRCP
ERCP
A relatively invasive method requires contrast agent injection into
Слайд 15Mirizzi syndrome
Type I - narrowing of common hepatic duct caused by calculus-induced
Mirizzi syndrome
Type I - narrowing of common hepatic duct caused by calculus-induced
Слайд 16Bile duct cysts. Classification
Todani classification
Cysts are diagnosed in patients aged 3
Bile duct cysts. Classification
Todani classification
Cysts are diagnosed in patients aged 3
Слайд 17Caroli disease (cystic lesion type V)
Surgery – liver resection
15
Caroli disease (cystic lesion type V)
Surgery – liver resection
15
Слайд 18Primary sclerosing cholangitis
Chronic course
Cause is unclear
Multiple strictures and dilatations
Primary sclerosing cholangitis
Chronic course
Cause is unclear
Multiple strictures and dilatations
Слайд 19Haemobilia
Damage to the liver or intrahepatic bile ducts, local liver necrosis.
Haemobilia
Damage to the liver or intrahepatic bile ducts, local liver necrosis.
Слайд 20Parasitic invasion
Opisthorchiasis (Ob, Volga basin, East Asia)
Echinococcosis, alveococcosis, ascariasis,
Parasitic invasion
Opisthorchiasis (Ob, Volga basin, East Asia)
Echinococcosis, alveococcosis, ascariasis,
Слайд 21Symptoms and diagnosis of painful obstructive jaundice
Acute onset
Scleral icterus
Pain attack
Dark urine, stool
Symptoms and diagnosis of painful obstructive jaundice
Acute onset
Scleral icterus
Pain attack
Dark urine, stool
Слайд 22ACUTE CHOLANGITIS
20
ACUTE CHOLANGITIS
20
Слайд 23Acute cholangitis (AC)
AC is an infectious inflammation of the bile ducts.
Acute cholangitis (AC)
AC is an infectious inflammation of the bile ducts.
Слайд 24Cholangiovenous reflux
Corrosion casting. Scanning electron microscopy
Secretory pressure. Microbial metabolite pressure.
Cholangiovenous reflux
Corrosion casting. Scanning electron microscopy
Secretory pressure. Microbial metabolite pressure.
Слайд 25
Symptoms of acute cholangitis
Chills, fever
Leukocytosis
Infection
Symptoms associated with biliary
Symptoms of acute cholangitis
Chills, fever
Leukocytosis
Infection
Symptoms associated with biliary
Слайд 26Causes of short-term SIRS and symptoms of sepsis
Two factors:
Large purulent surface
Causes of short-term SIRS and symptoms of sepsis
Two factors:
Large purulent surface
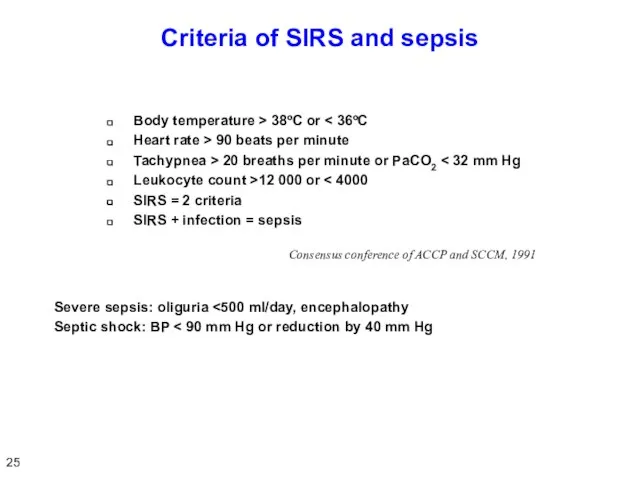
Слайд 27Criteria of SIRS and sepsis
Body temperature > 38ºC or < 36ºC
Heart rate
Criteria of SIRS and sepsis
Body temperature > 38ºC or < 36ºC
Heart rate
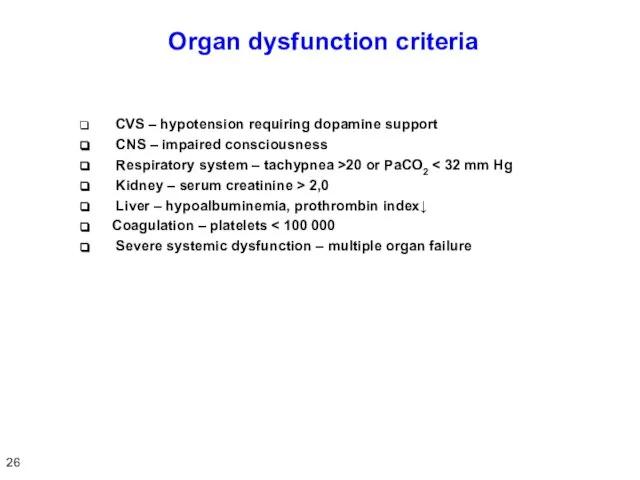
Слайд 28 Organ dysfunction criteria
CVS – hypotension requiring dopamine support
CNS
Organ dysfunction criteria
CVS – hypotension requiring dopamine support
CNS
Слайд 29Renal failure in acute cholangitis
Kidney is a main organ secreting bile components
Renal failure in acute cholangitis
Kidney is a main organ secreting bile components
Слайд 30Management of acute cholangitis (choledocholithiasis, n = 613)
Objective: to interrupt the course
Management of acute cholangitis (choledocholithiasis, n = 613)
Objective: to interrupt the course
Слайд 31Treatment of pyogenic liver abscesses in acute cholangitis (n = 19)
The
Treatment of pyogenic liver abscesses in acute cholangitis (n = 19) The
Слайд 32Stages of acute cholangitis and Tokyo Guidelines (2007)
*Overall and antimicrobial therapy
Emergency biliary
Stages of acute cholangitis and Tokyo Guidelines (2007)
*Overall and antimicrobial therapy
Emergency biliary
Слайд 33Chronic cholangitis
Chronic cholangitis may be diagnosed in patients with:
post-traumatic strictures;
primary sclerosing
Chronic cholangitis may be diagnosed in patients with:
post-traumatic strictures;
primary sclerosing
Слайд 34Chronic cholangitis in patients with AIDS
Causative agents : Cryptosporidium and Cytomegalovirus.
Chronic cholangitis in patients with AIDS
Causative agents : Cryptosporidium and Cytomegalovirus.
Слайд 35Conclusion
Acute cholangitis is characterized by purulent process proceeding on the background of
Conclusion
Acute cholangitis is characterized by purulent process proceeding on the background of
Слайд 36PAINLESS OBSTRUCTIVE JAUNDICE
35
PAINLESS OBSTRUCTIVE JAUNDICE
35
Слайд 37Tumors of bile ducts
Progressive biliary obstruction. Jaundice is the first, but not
Tumors of bile ducts
Progressive biliary obstruction. Jaundice is the first, but not
Слайд 38Symptoms of painless obstructive jaundice
Icteric sclera and skin
Itching
Dark urine and stool discoloration
No
Symptoms of painless obstructive jaundice
Icteric sclera and skin
Itching
Dark urine and stool discoloration
No
Слайд 39Cancer of hepatic and common bile ducts
Common hepatic duct
(Klatskin tumor)
56%
Common bile
Cancer of hepatic and common bile ducts
Common hepatic duct
(Klatskin tumor)
56%
Common bile
Слайд 40Classification of hepatic duct cancer (Bismuth)
39
Classification of hepatic duct cancer (Bismuth)
39
Слайд 41MR-cholangiography in Klatskin tumor
40
MR-cholangiography in Klatskin tumor
40
Слайд 42Pancreatic head cancer. MRCP
41
Pancreatic head cancer. MRCP
41
Слайд 43Differential diagnosis of obstructive and parenchymatous jaundice
Patients with a painless obstructive jaundice
Differential diagnosis of obstructive and parenchymatous jaundice
Patients with a painless obstructive jaundice
Слайд 44Functional and morphological features of liver in painless obstructive jaundice
Increased levels of
Functional and morphological features of liver in painless obstructive jaundice
Increased levels of
Слайд 45Metabolic disorders in painless obstructive jaundice
Reduced ATP and local blood flow velocity
Metabolic disorders in painless obstructive jaundice
Reduced ATP and local blood flow velocity
Слайд 46Conclusion on disorders arising in painless obstructive jaundice
Painless obstructive jaundice causes severe
Conclusion on disorders arising in painless obstructive jaundice
Painless obstructive jaundice causes severe
Слайд 47PREOPERATIVE DECOMPRESSION
46
PREOPERATIVE DECOMPRESSION
46
Слайд 48Preoperative decompression of the bile ducts
Methods of preoperative biliary decompression:
Percutaneous cholangiostomy.
Preoperative decompression of the bile ducts
Methods of preoperative biliary decompression:
Percutaneous cholangiostomy.
Слайд 49Can bile duct decompression per se impair liver function?
In a 12-day obstructive
Can bile duct decompression per se impair liver function?
In a 12-day obstructive
Слайд 50 Comparison of various methods of bile duct decompression (n = 205)
NBD-85,
Comparison of various methods of bile duct decompression (n = 205)
NBD-85,
Слайд 51 Morbidity and mortality in various rates of bile duct decompression
* –
Morbidity and mortality in various rates of bile duct decompression
* –
Слайд 52 Positive and negative aspects of preoperative biliary decompression
51
Opinions on stenting are
Positive and negative aspects of preoperative biliary decompression
51
Opinions on stenting are
Слайд 53 Features of preoperative biliary decompression in Klatskin tumor
52
Radical surgery for Klatskin
Features of preoperative biliary decompression in Klatskin tumor
52
Radical surgery for Klatskin
 Прием пациента в стационар. Лекция №1
Прием пациента в стационар. Лекция №1 Измерение уровня глюкозы без глюкометра
Измерение уровня глюкозы без глюкометра Цистаденома и опухолевидные образования
Цистаденома и опухолевидные образования Внутриутробная инфекция (ВУИ). Инфекция в перинатологии
Внутриутробная инфекция (ВУИ). Инфекция в перинатологии Болезнь Альцгеймера (деменция альцгеймеровского типа)
Болезнь Альцгеймера (деменция альцгеймеровского типа) Предупреждение заболеваний почек. Питьевой режим
Предупреждение заболеваний почек. Питьевой режим Артериальная гипертензия (АГ)
Артериальная гипертензия (АГ) Корисний йогурт
Корисний йогурт Ведение беременных с резус-отрицательной кровью
Ведение беременных с резус-отрицательной кровью Паливизумаб
Паливизумаб Гигиена, санитария и производственный контроль при организации труда. Санитарно-эпидемиологические требования к парикмахерским
Гигиена, санитария и производственный контроль при организации труда. Санитарно-эпидемиологические требования к парикмахерским Гломерулонефриты
Гломерулонефриты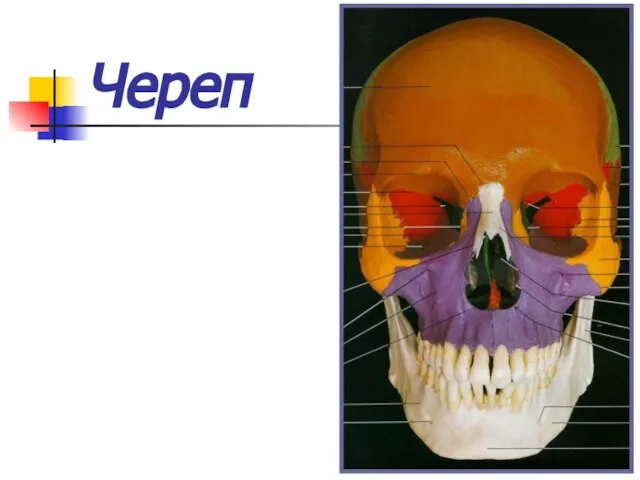 Череп. Развитие
Череп. Развитие Порядок создания и организации работы психолого-медико-педагогического консилиума. Шаблон
Порядок создания и организации работы психолого-медико-педагогического консилиума. Шаблон Эффективность рекламы и брендинга Уроки США и Европы
Эффективность рекламы и брендинга Уроки США и Европы Презентация агентства Maximum Maximorum presented by Maximorum adv.ag.
Презентация агентства Maximum Maximorum presented by Maximorum adv.ag. Опорно-двигательная система, ее функции
Опорно-двигательная система, ее функции Фармакотерапия в сестринской практике
Фармакотерапия в сестринской практике Анатомия зубов
Анатомия зубов Определение Гиперлипопротеинемий по Фридрексену
Определение Гиперлипопротеинемий по Фридрексену Этиология и патогенез ЗЧА
Этиология и патогенез ЗЧА Действие антихолинэстеразных лекарственных средств
Действие антихолинэстеразных лекарственных средств Особенности развития костной системы младшего школьника
Особенности развития костной системы младшего школьника Необходимость прямого скрининга на выявление атеросклероза
Необходимость прямого скрининга на выявление атеросклероза Дефекты зрения
Дефекты зрения Болезнь Андерсена
Болезнь Андерсена Отличное зрение
Отличное зрение Ирумед. Базовая информация. Основные принципы терапии артериальной гипертонии
Ирумед. Базовая информация. Основные принципы терапии артериальной гипертонии