- path anatomy git

Содержание
- 2. Pancreatic cancer occurs when changes (mutations) in the pancreas cells lead them to multiply out of
- 3. There are two types of tumors that grow in the pancreas: exocrine or neuroendocrine tumors. About
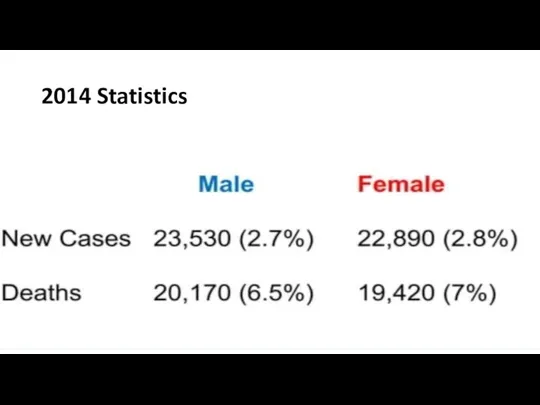
- 5. 2014 Statistics
- 6. Risk factors for pancreatic cancer include the following Smoking Obesity Personal history of diabetes or chronic
- 7. Symptoms Most patients present with pain (in the back) weight loss or jaundice Tumors in the
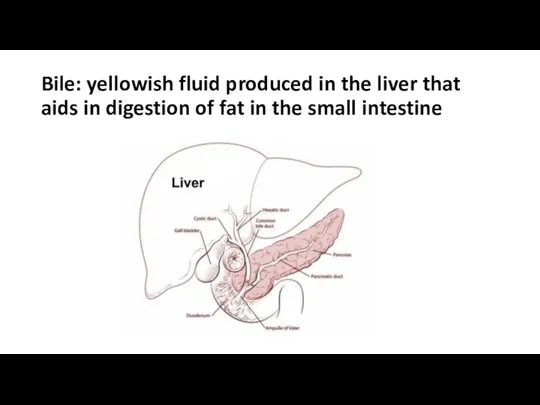
- 8. Bile: yellowish fluid produced in the liver that aids in digestion of fat in the small
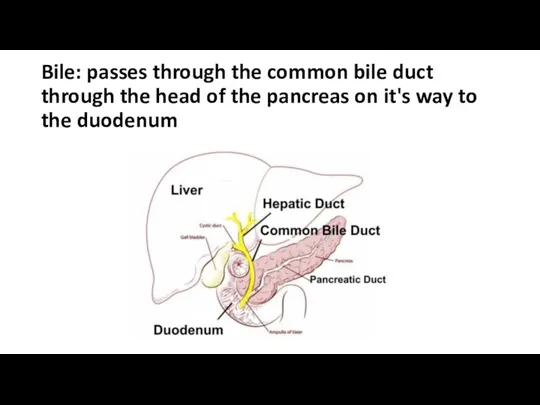
- 9. Bile: passes through the common bile duct through the head of the pancreas on it's way
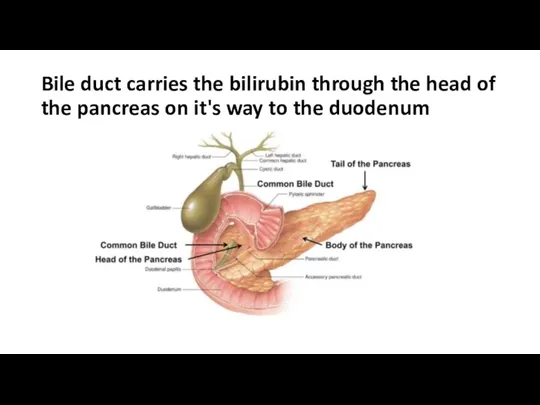
- 10. Bile duct carries the bilirubin through the head of the pancreas on it's way to the
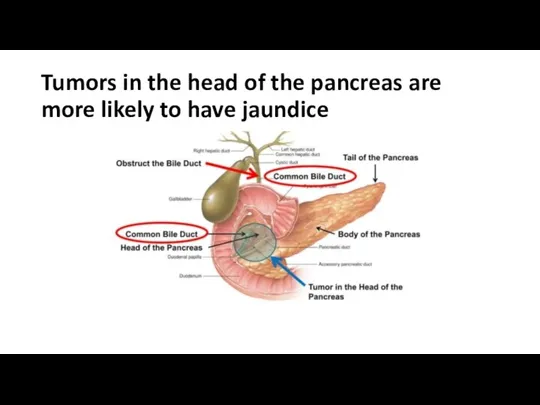
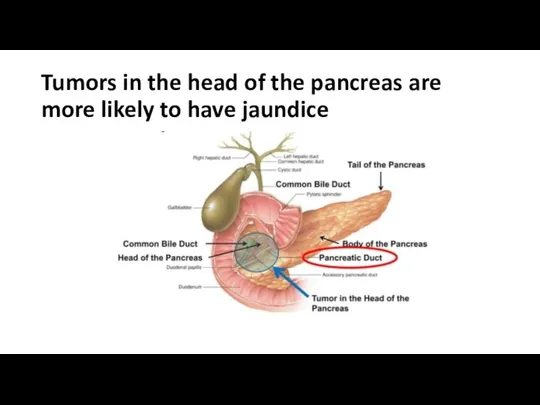
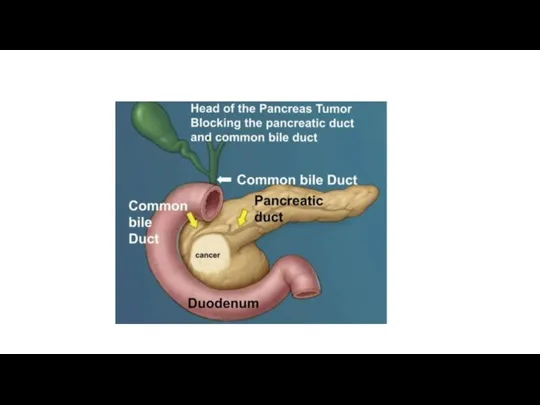
- 11. Tumors in the head of the pancreas are more likely to have jaundice
- 12. Tumors in the head of the pancreas are more likely to have jaundice
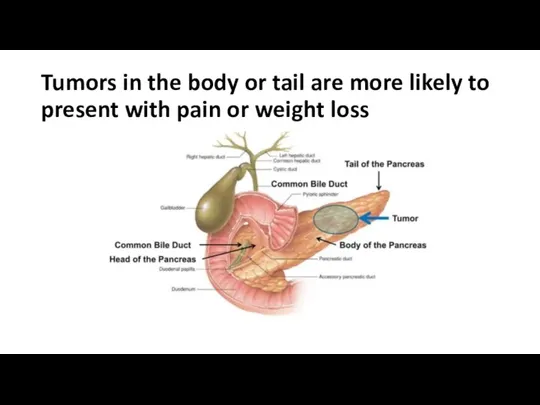
- 14. Tumors in the body or tail are more likely to present with pain or weight loss
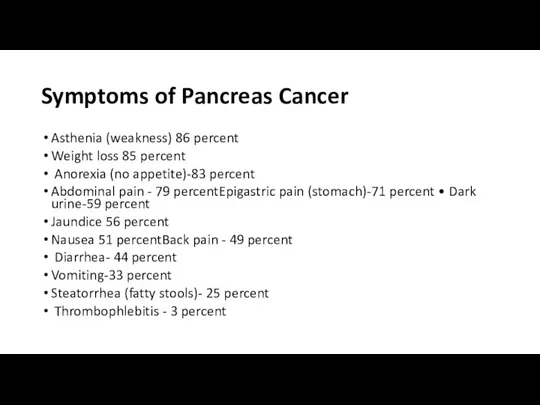
- 15. Symptoms of Pancreas Cancer Asthenia (weakness) 86 percent Weight loss 85 percent Anorexia (no appetite)-83 percent
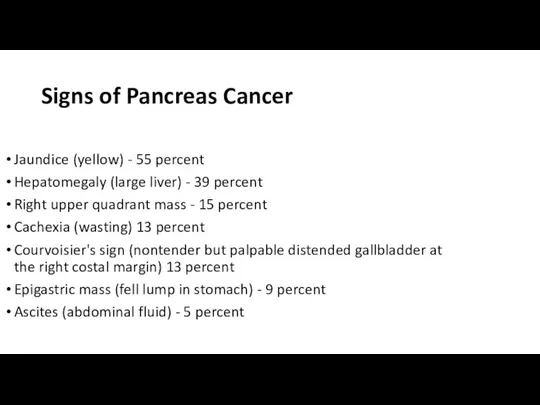
- 16. Signs of Pancreas Cancer Jaundice (yellow) - 55 percent Hepatomegaly (large liver) - 39 percent Right
- 17. Pathology Ductal adenocarcinoma accounts for about 85% of all neoplasms. And more than 95% of all
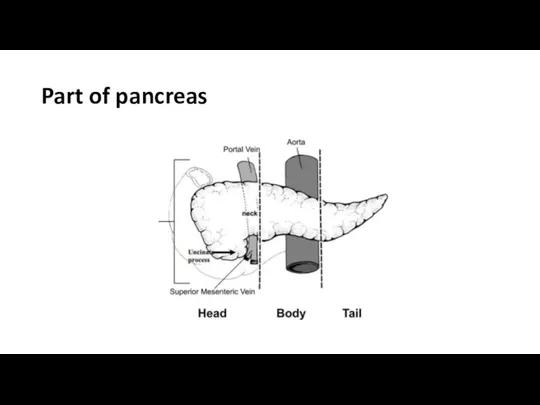
- 18. Part of pancreas
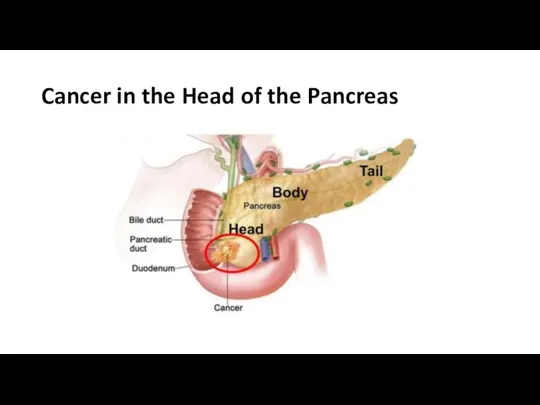
- 19. Cancer in the Head of the Pancreas
- 20. Location of Pancreas Cancer 60 to 70 percent of exocrine pancreatic cancers are localized to the
- 21. Tests used to evaluate and stage pancreas cancer Routine blood tests e.g. liver products like bilirubin
- 22. CA 19-9 The reported sensitivity and specificity rates of CA 19-9 for pancreatic cancer range from
- 23. Elevated CA 19-9 Cancer Pancreas Biliary Cancer (gallbladder, cholangiocarcinoma,ampullary)- Hepatocellular Gastric, ovarian, colorectal (less often) Lung,
- 24. Ultrasound study of 900 patients who underwent ultrasound to work up painless jaundice, anorexia, or unexplained
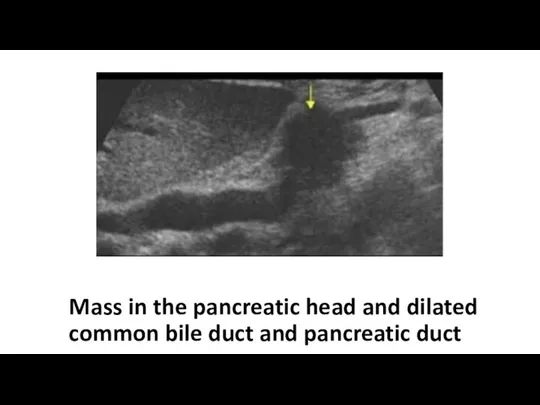
- 25. Mass in the pancreatic head and dilated common bile duct and pancreatic duct
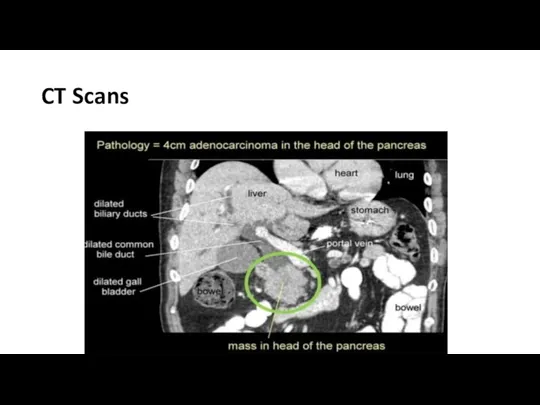
- 26. CT Sensitivity of CT for pancreatic cancer depends on technique and is highest (89 to 97
- 27. Endoscopy or ERCP or EUS
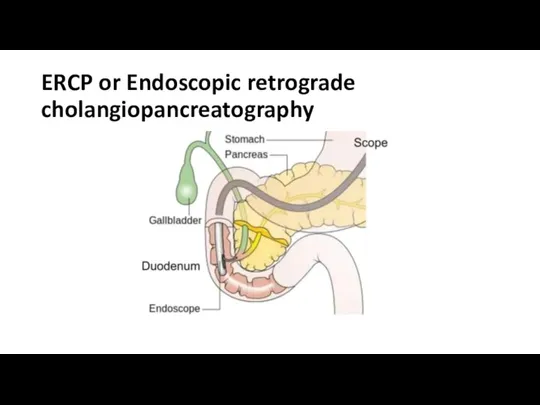
- 28. ERCP or Endoscopic retrograde cholangiopancreatography
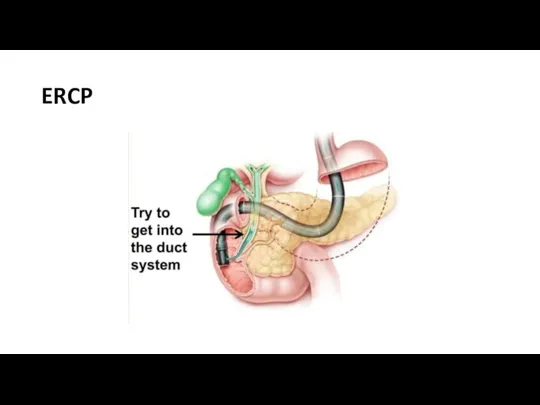
- 29. ERCP
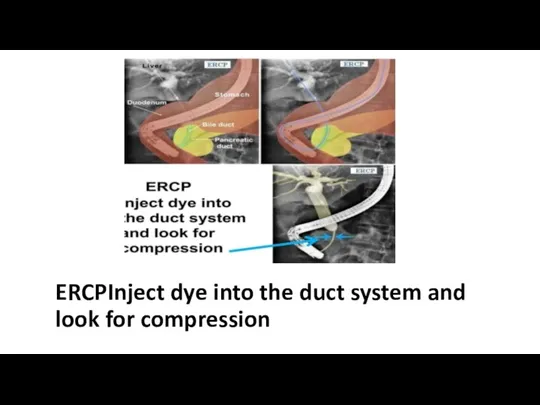
- 30. ERCPInject dye into the duct system and look for compression
- 31. ERCP Sensitivity of 92 percent and Specificity of 96 percent for diagnosing cancer of the pancreas
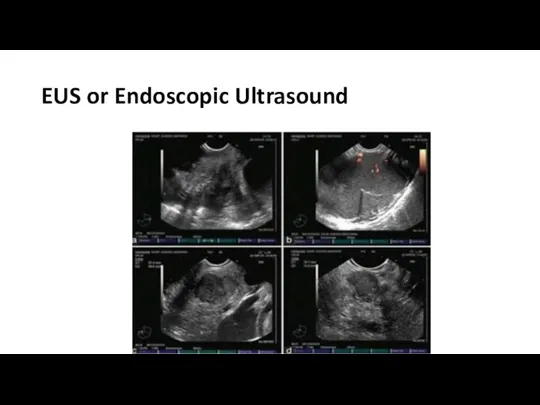
- 32. EUS or Endoscopic Ultrasound
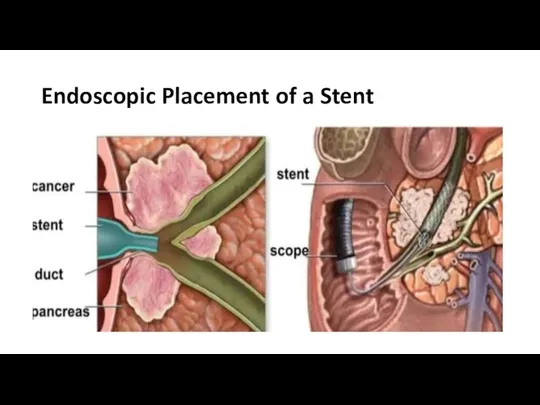
- 33. Endoscopic Placement of a Stent
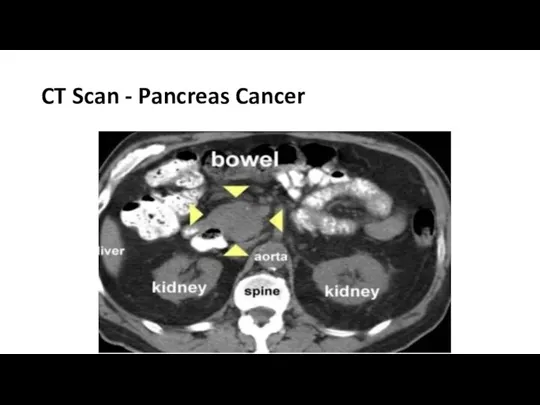
- 34. CT Scan - Pancreas Cancer
- 35. CT Scans
- 36. CT or PET Scan
- 38. PET Scans
- 39. Stage IA (T1aNOMO)
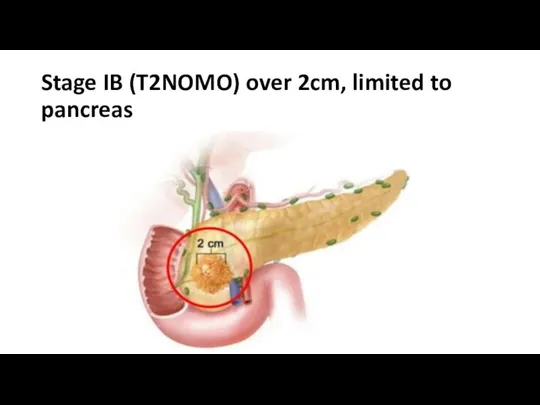
- 40. Stage IB (T2NOMO) over 2cm, limited to pancreas
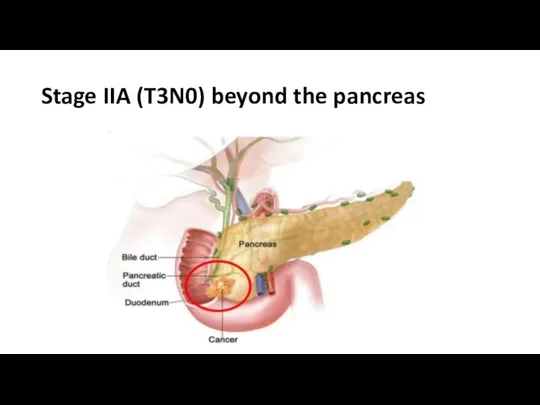
- 41. Stage IIA (T3N0) beyond the pancreas
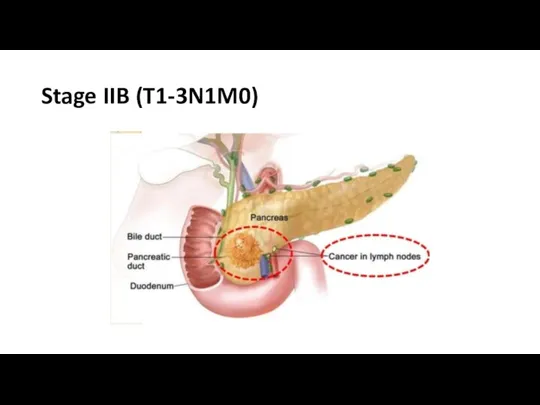
- 42. Stage IIB (T1-3N1M0)
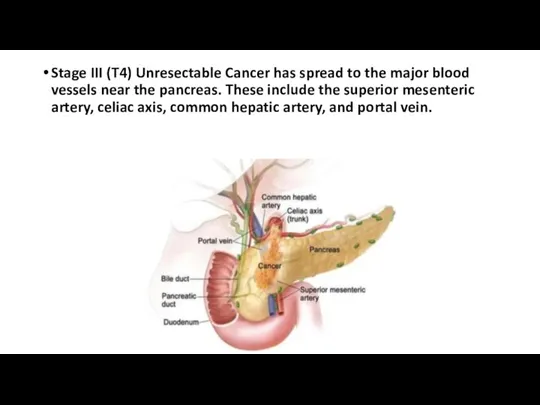
- 43. Stage III (T4) Unresectable Cancer has spread to the major blood vessels near the pancreas. These
- 45. Скачать презентацию
Слайд 3There are two types of tumors that grow in the pancreas: exocrine
There are two types of tumors that grow in the pancreas: exocrine

Слайд 52014 Statistics
2014 Statistics
Слайд 6Risk factors for pancreatic cancer include the following
Smoking
Obesity
Personal history of diabetes or
Risk factors for pancreatic cancer include the following
Smoking
Obesity
Personal history of diabetes or
Слайд 7Symptoms
Most patients present with pain (in the back) weight loss or jaundice
Tumors
Symptoms
Most patients present with pain (in the back) weight loss or jaundice
Tumors
Слайд 8Bile: yellowish fluid produced in the liver that aids in digestion of
Bile: yellowish fluid produced in the liver that aids in digestion of
Слайд 9Bile: passes through the common bile duct through the head of the
Bile: passes through the common bile duct through the head of the
Слайд 10Bile duct carries the bilirubin through the head of the pancreas on
Bile duct carries the bilirubin through the head of the pancreas on
Слайд 11Tumors in the head of the pancreas are more likely to have
Tumors in the head of the pancreas are more likely to have
Слайд 12Tumors in the head of the pancreas are more likely to have
Tumors in the head of the pancreas are more likely to have
Слайд 14Tumors in the body or tail are more likely to present with
Tumors in the body or tail are more likely to present with
Слайд 15Symptoms of Pancreas Cancer
Asthenia (weakness) 86 percent
Weight loss 85 percent
Anorexia (no
Symptoms of Pancreas Cancer
Asthenia (weakness) 86 percent
Weight loss 85 percent
Anorexia (no
Слайд 16Signs of Pancreas Cancer
Jaundice (yellow) - 55 percent
Hepatomegaly (large liver) - 39
Signs of Pancreas Cancer
Jaundice (yellow) - 55 percent
Hepatomegaly (large liver) - 39
Слайд 17Pathology
Ductal adenocarcinoma accounts for about 85% of all neoplasms. And more
Pathology
Ductal adenocarcinoma accounts for about 85% of all neoplasms. And more
Слайд 18Part of pancreas
Part of pancreas
Слайд 19Cancer in the Head of the Pancreas
Cancer in the Head of the Pancreas
Слайд 20Location of Pancreas Cancer
60 to 70 percent of exocrine pancreatic cancers are
Location of Pancreas Cancer
60 to 70 percent of exocrine pancreatic cancers are
Слайд 21Tests used to evaluate and stage pancreas cancer
Routine blood tests e.g. liver
Tests used to evaluate and stage pancreas cancer
Routine blood tests e.g. liver
Слайд 22CA 19-9
The reported sensitivity and specificity rates of CA 19-9 for pancreatic
CA 19-9
The reported sensitivity and specificity rates of CA 19-9 for pancreatic
Слайд 23Elevated CA 19-9
Cancer
Pancreas
Biliary Cancer (gallbladder, cholangiocarcinoma,ampullary)- Hepatocellular
Gastric, ovarian, colorectal (less often)
Lung,
Elevated CA 19-9
Cancer
Pancreas
Biliary Cancer (gallbladder, cholangiocarcinoma,ampullary)- Hepatocellular
Gastric, ovarian, colorectal (less often)
Lung,
Слайд 24Ultrasound
study of 900 patients who underwent ultrasound to work up painless jaundice,
Ultrasound
study of 900 patients who underwent ultrasound to work up painless jaundice,
Слайд 25Mass in the pancreatic head and dilated common bile duct and pancreatic
Mass in the pancreatic head and dilated common bile duct and pancreatic
Слайд 26CT
Sensitivity of CT for pancreatic cancer depends on technique and is highest
CT
Sensitivity of CT for pancreatic cancer depends on technique and is highest

Слайд 27Endoscopy or ERCP or EUS
Endoscopy or ERCP or EUS
Слайд 28ERCP or Endoscopic retrograde cholangiopancreatography
ERCP or Endoscopic retrograde cholangiopancreatography
Слайд 29ERCP
ERCP
Слайд 30ERCPInject dye into the duct system and look for compression
ERCPInject dye into the duct system and look for compression
Слайд 31ERCP
Sensitivity of 92 percent and Specificity of 96 percent for diagnosing cancer
ERCP
Sensitivity of 92 percent and Specificity of 96 percent for diagnosing cancer
Слайд 32EUS or Endoscopic Ultrasound
EUS or Endoscopic Ultrasound
Слайд 33Endoscopic Placement of a Stent
Endoscopic Placement of a Stent
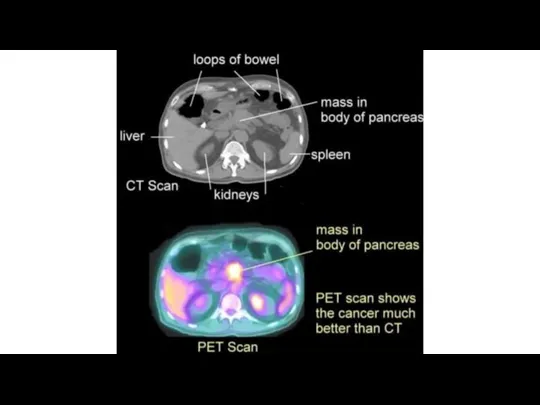
Слайд 34CT Scan - Pancreas Cancer
CT Scan - Pancreas Cancer
Слайд 35CT Scans
CT Scans
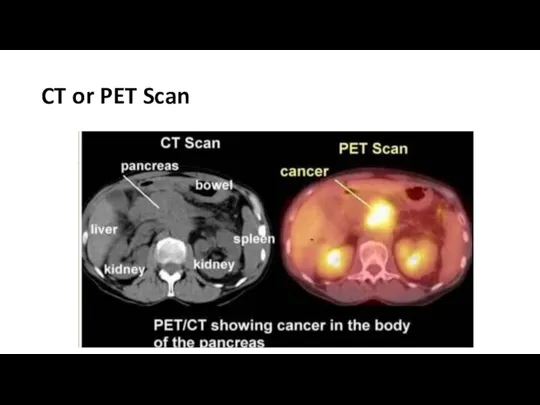
Слайд 36CT or PET Scan
CT or PET Scan
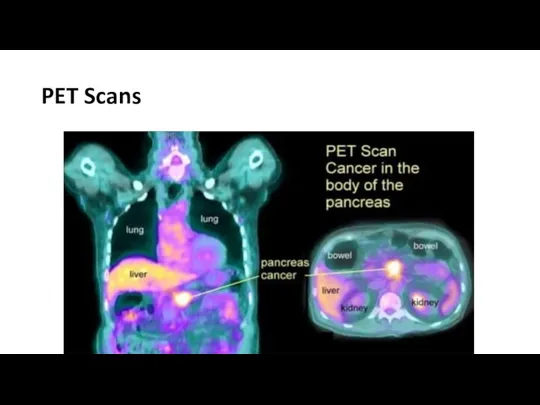
Слайд 38PET Scans
PET Scans
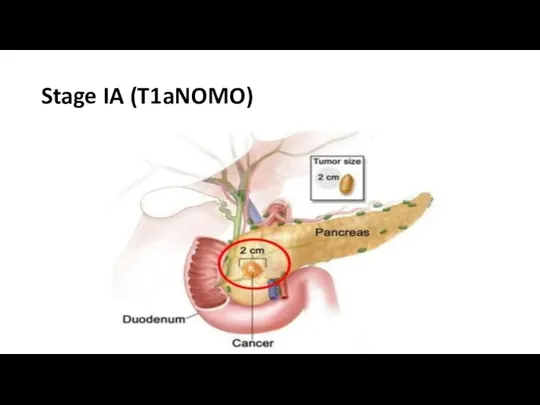
Слайд 39Stage IA (T1aNOMO)
Stage IA (T1aNOMO)
Слайд 40Stage IB (T2NOMO) over 2cm, limited to pancreas
Stage IB (T2NOMO) over 2cm, limited to pancreas
Слайд 41Stage IIA (T3N0) beyond the pancreas
Stage IIA (T3N0) beyond the pancreas
Слайд 42Stage IIB (T1-3N1M0)
Stage IIB (T1-3N1M0)
Слайд 43Stage III (T4) Unresectable Cancer has spread to the major blood vessels
Stage III (T4) Unresectable Cancer has spread to the major blood vessels
 Полезная и вредная еда
Полезная и вредная еда ПЕРВАЯ ПОМОЩЬ ПРИ СИНДРОМЕ ДЛИТЕЛЬНОГО СДАВЛЕНИЯ (1)
ПЕРВАЯ ПОМОЩЬ ПРИ СИНДРОМЕ ДЛИТЕЛЬНОГО СДАВЛЕНИЯ (1) Нарушения нижней конечности (косолапость, дисплазия и вывих тазобедренного сустава)
Нарушения нижней конечности (косолапость, дисплазия и вывих тазобедренного сустава) Деменция. Болезнь Альцгеймера
Деменция. Болезнь Альцгеймера Питайся правильно и предотврати заболевание раком
Питайся правильно и предотврати заболевание раком Вспомогательные репродуктивные технологии
Вспомогательные репродуктивные технологии Тихвинская межрайонная больница имени А.Ф. Калмыкова
Тихвинская межрайонная больница имени А.Ф. Калмыкова Осанка - стройная спина
Осанка - стройная спина першин hallux valgus
першин hallux valgus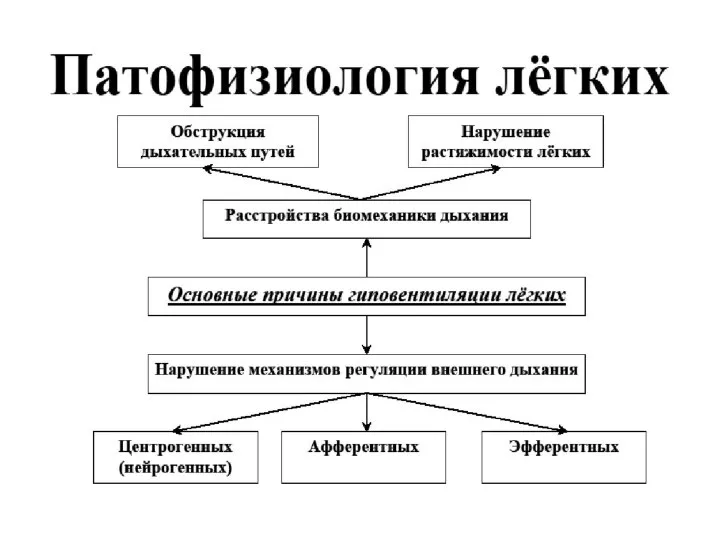 Дыхательная недостаточность
Дыхательная недостаточность Таспа құрттар
Таспа құрттар ПаЃ£а†ђђл Ґ•§•≠®п аЃ§ЃҐ Л®з≠л© §Ѓ™вЃа
ПаЃ£а†ђђл Ґ•§•≠®п аЃ§ЃҐ Л®з≠л© §Ѓ™вЃа Философия и медицина: современное взаимодействие
Философия и медицина: современное взаимодействие Врачебный контроль за детьми и подростками при занятиях спортом
Врачебный контроль за детьми и подростками при занятиях спортом Федор Иванович Валькер
Федор Иванович Валькер Terapeitiskā terapija, kas atbilst vairāk pacientu grupu
Terapeitiskā terapija, kas atbilst vairāk pacientu grupu Инфекционные болезни
Инфекционные болезни Координационные способности и их развитие
Координационные способности и их развитие Анализ работы амбулаторнополиклинической службы за 2020 год
Анализ работы амбулаторнополиклинической службы за 2020 год Аномалии развития ЗЧС
Аномалии развития ЗЧС Рак поджелудочной железы
Рак поджелудочной железы Врождённые аномалии развития носа и околоносовых пазух
Врождённые аномалии развития носа и околоносовых пазух Роль диссеминированных опухолевых клеток в костном мозге у пациенток с люминальным типом рака молочной железы
Роль диссеминированных опухолевых клеток в костном мозге у пациенток с люминальным типом рака молочной железы Современные подходы к лечению РС
Современные подходы к лечению РС 7
7 Медицинская протозоология
Медицинская протозоология Применение методологии клинической лингвистики в исследовании психоаналитического дискурса
Применение методологии клинической лингвистики в исследовании психоаналитического дискурса Нарушение глотания. Взгляд с точки зрения терапии и ухода
Нарушение глотания. Взгляд с точки зрения терапии и ухода