- Principles of external fixators

Содержание
- 2. Indications External fixation has a vital role in both provisional and definitive fracture fixation. In provisional
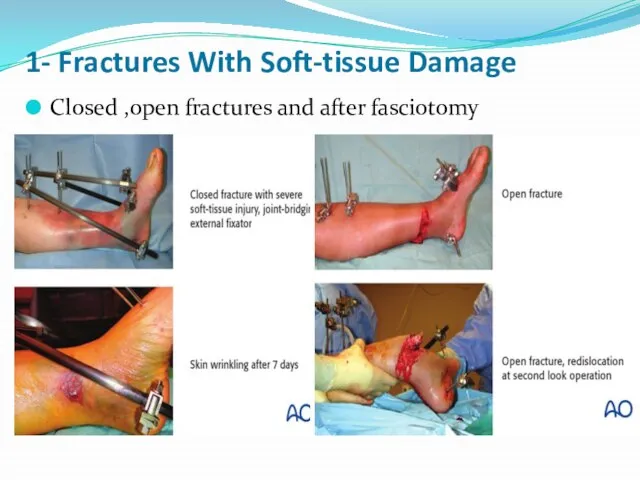
- 3. 1- Fractures With Soft-tissue Damage Closed ,open fractures and after fasciotomy
- 4. 2- Polytrauma—Damage Control Surgery Provisional application of external fixator as fast as possible to stablise the
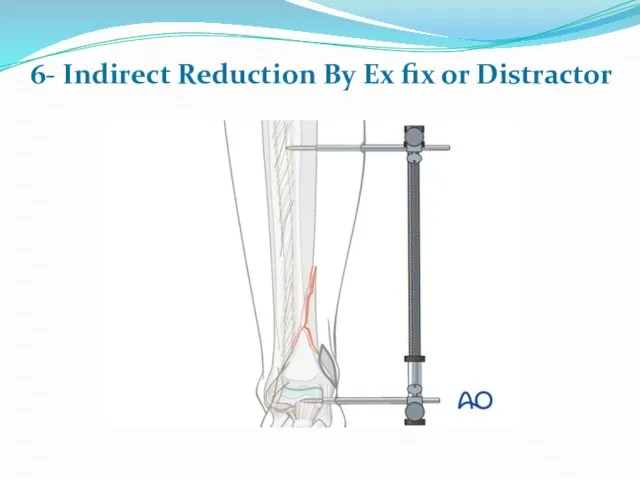
- 5. 6- Indirect Reduction By Ex fix or Distractor
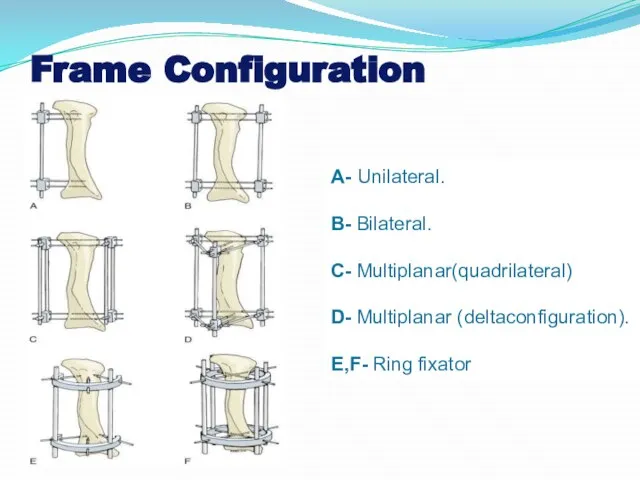
- 6. Frame Configuration A- Unilateral. B- Bilateral. C- Multiplanar(quadrilateral) D- Multiplanar (deltaconfiguration). E,F- Ring fixator
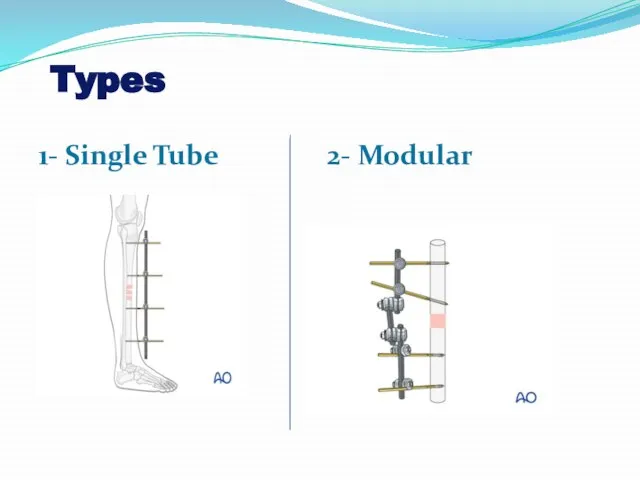
- 7. Types 1- Single Tube 2- Modular
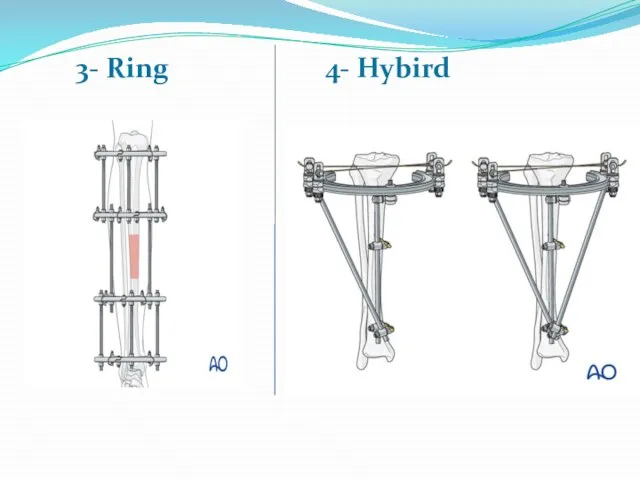
- 8. 3- Ring 4- Hybird
- 9. 5- Monolateral Dynamic Lrs and ball joint spaning orthofix
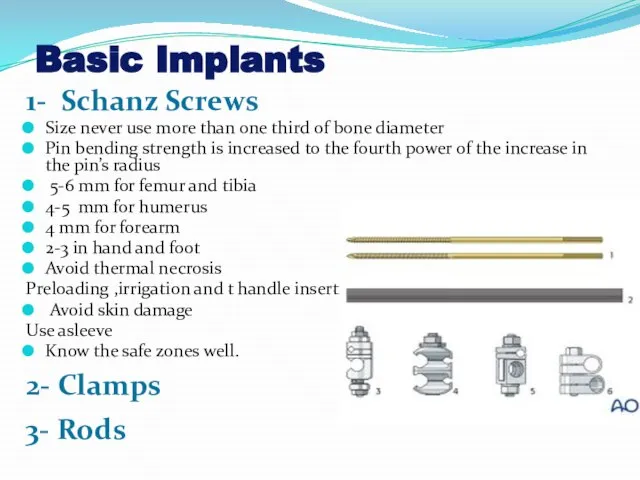
- 10. Basic Implants 1- Schanz Screws Size never use more than one third of bone diameter Pin
- 11. Safe Zones Humerus Pins (5 mm) are placed anterolaterally in the proximal humerus, taking care to
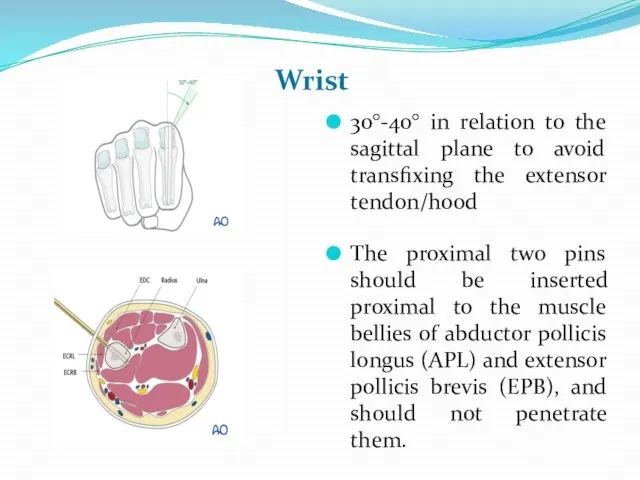
- 12. Wrist 30°-40° in relation to the sagittal plane to avoid transfixing the extensor tendon/hood The proximal
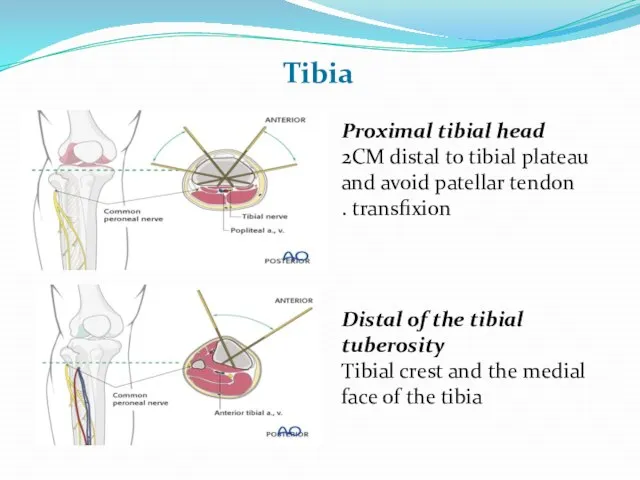
- 13. Tibia Proximal tibial head 2CM distal to tibial plateau and avoid patellar tendon transfixion . Distal
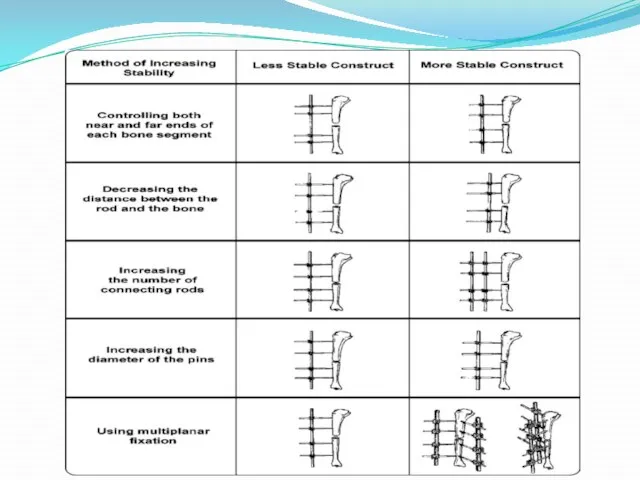
- 14. Factors Adding To Stability Of External FixationI 1- The stiffness of the frame increases with the
- 17. Скачать презентацию
Слайд 31- Fractures With Soft-tissue Damage
Closed ,open fractures and after fasciotomy
1- Fractures With Soft-tissue Damage
Closed ,open fractures and after fasciotomy
Слайд 42- Polytrauma—Damage Control Surgery
Provisional application of external fixator as fast as possible
2- Polytrauma—Damage Control Surgery
Provisional application of external fixator as fast as possible
Provisional application of external fixator as fast as possible
Слайд 56- Indirect Reduction By Ex fix or Distractor
6- Indirect Reduction By Ex fix or Distractor
Слайд 6Frame Configuration
A- Unilateral.
B- Bilateral.
C- Multiplanar(quadrilateral)
D- Multiplanar (deltaconfiguration).
E,F- Ring fixator
Frame Configuration
A- Unilateral.
B- Bilateral.
C- Multiplanar(quadrilateral)
D- Multiplanar (deltaconfiguration).
E,F- Ring fixator
Слайд 7Types
1- Single Tube 2- Modular
Types
1- Single Tube 2- Modular
Слайд 83- Ring 4- Hybird
3- Ring 4- Hybird
Слайд 95- Monolateral Dynamic Lrs and ball joint spaning orthofix
5- Monolateral Dynamic Lrs and ball joint spaning orthofix

Слайд 10Basic Implants
1- Schanz Screws
Size never use more than one third
Basic Implants
1- Schanz Screws
Size never use more than one third
Слайд 11Safe Zones
Humerus
Pins (5 mm) are placed anterolaterally in the proximal humerus, taking
Safe Zones
Humerus
Pins (5 mm) are placed anterolaterally in the proximal humerus, taking
Слайд 12Wrist
30°-40° in relation to the sagittal plane to avoid transfixing the extensor
Wrist
30°-40° in relation to the sagittal plane to avoid transfixing the extensor
Слайд 13Tibia
Proximal tibial head
2CM distal to tibial plateau and avoid patellar
Tibia
Proximal tibial head
2CM distal to tibial plateau and avoid patellar
Слайд 14Factors Adding To Stability Of External FixationI
1- The stiffness of the frame
Factors Adding To Stability Of External FixationI
1- The stiffness of the frame
 Периферическая нервная система!
Периферическая нервная система! Tolerance, autoimmunity, allogenicity
Tolerance, autoimmunity, allogenicity Классификация медицинских отходов по степени их эпидемической, токсикологической и радиационной опасности
Классификация медицинских отходов по степени их эпидемической, токсикологической и радиационной опасности Серологические методы исследования
Серологические методы исследования NASLEDSTVENNYE_BOLEZNI_ChELOVEKA (1)
NASLEDSTVENNYE_BOLEZNI_ChELOVEKA (1) COVID-инфекция и глаз
COVID-инфекция и глаз Рак мочевого пузыря
Рак мочевого пузыря Нервная система головного мозга
Нервная система головного мозга Иммуноглобулин. Комплемент жүйесі
Иммуноглобулин. Комплемент жүйесі Остеология. Добавочный скелет
Остеология. Добавочный скелет Аритмия. Определение
Аритмия. Определение Демодекоз
Демодекоз Аускультация сердца и сосудов
Аускультация сердца и сосудов Первые признаки инсульта
Первые признаки инсульта Клиническая фармакология и принципы выбора антиаритмических препаратов
Клиническая фармакология и принципы выбора антиаритмических препаратов Понятие и виды психических процессов
Понятие и виды психических процессов Потребности детей грудного возраста и способы их удовлетворения
Потребности детей грудного возраста и способы их удовлетворения Миома матки
Миома матки 1226900 (1) (1)
1226900 (1) (1) Антибиотики
Антибиотики Improving the Odds Against Stroke
Improving the Odds Against Stroke Острое легочное сердце: дифференциальный диагноз
Острое легочное сердце: дифференциальный диагноз Дифтерия. Источники дифтерии
Дифтерия. Источники дифтерии Аутизм, РАС – биокоррекция при аутизме и РАС
Аутизм, РАС – биокоррекция при аутизме и РАС Профилактика и коррекция нарушения зрения
Профилактика и коррекция нарушения зрения Этическое и правовое регулирование научных исследований
Этическое и правовое регулирование научных исследований Қоғамдық тамақтандыруда өндірілетін негізгі екінші тамақтардың органолептикалық, физико-химиялық көрсетіштерін анықтау әдістері
Қоғамдық тамақтандыруда өндірілетін негізгі екінші тамақтардың органолептикалық, физико-химиялық көрсетіштерін анықтау әдістері Современные дезинфицирующие средства
Современные дезинфицирующие средства