- Cirrhosis (1)

Содержание
- 2. CIRRHOSIS • End stage liver disease (irreversible) • Result from many causes of chronic liver disease:
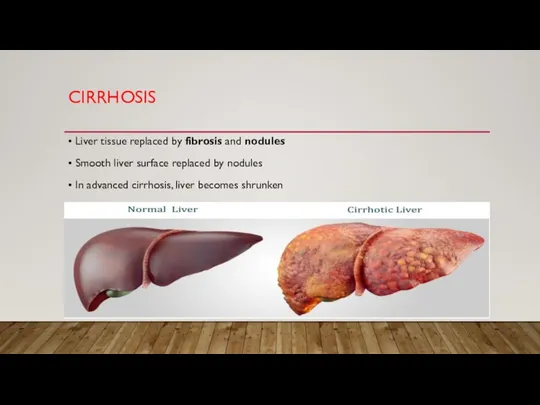
- 3. CIRRHOSIS • Liver tissue replaced by fibrosis and nodules • Smooth liver surface replaced by nodules
- 4. CLINICAL FEATURES • Hyperammonemia • Asterixis, confusion, coma
- 5. HYPERAMMONEMIA TREATMENT • Low protein diet • Lactulose • Synthetic disaccharide (laxative) • Colon breakdown by
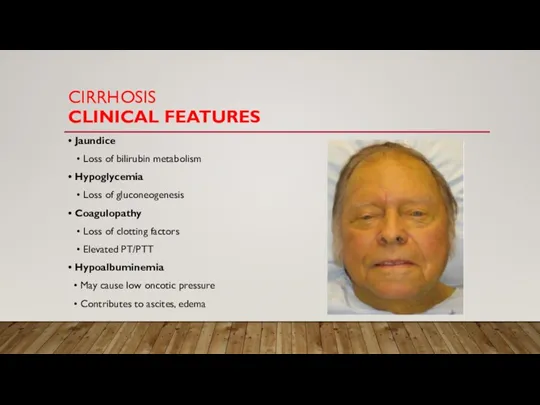
- 6. CIRRHOSIS CLINICAL FEATURES • Jaundice • Loss of bilirubin metabolism • Hypoglycemia • Loss of gluconeogenesis
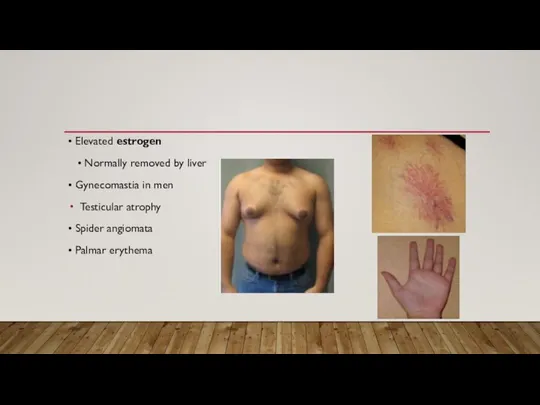
- 7. • Elevated estrogen • Normally removed by liver • Gynecomastia in men Testicular atrophy • Spider
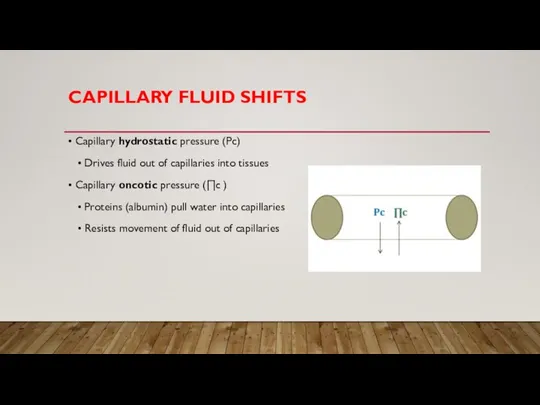
- 8. CAPILLARY FLUID SHIFTS • Capillary hydrostatic pressure (Pc) • Drives fluid out of capillaries into tissues
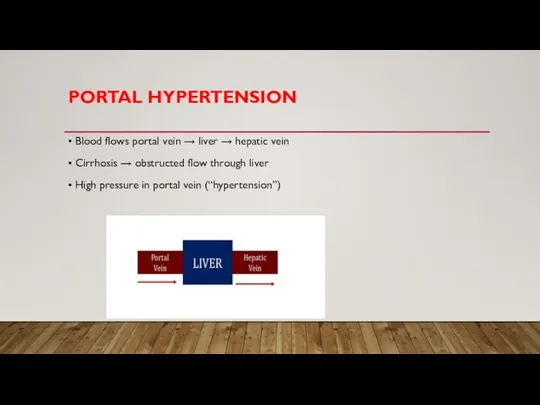
- 9. PORTAL HYPERTENSION • Blood flows portal vein → liver → hepatic vein • Cirrhosis → obstructed
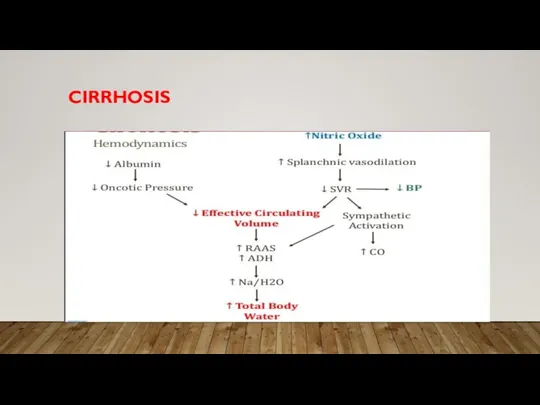
- 10. CIRRHOSIS
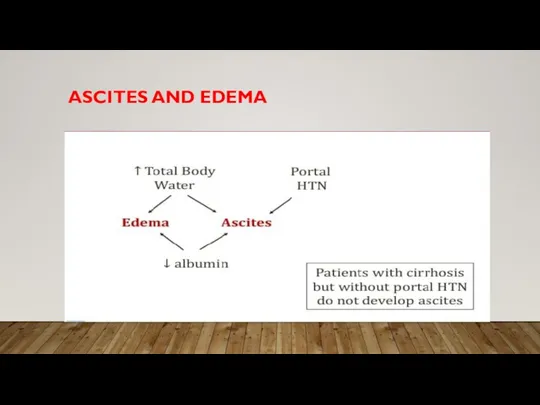
- 11. ASCITES AND EDEMA
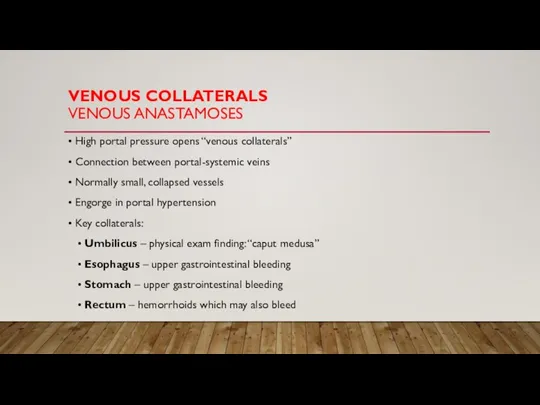
- 12. VENOUS COLLATERALS VENOUS ANASTAMOSES • High portal pressure opens “venous collaterals” • Connection between portal-systemic veins
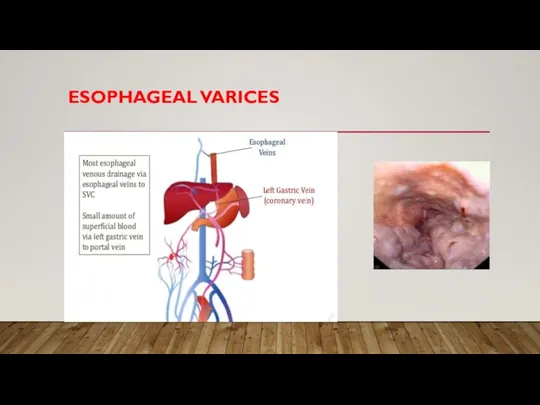
- 13. ESOPHAGEAL VARICES
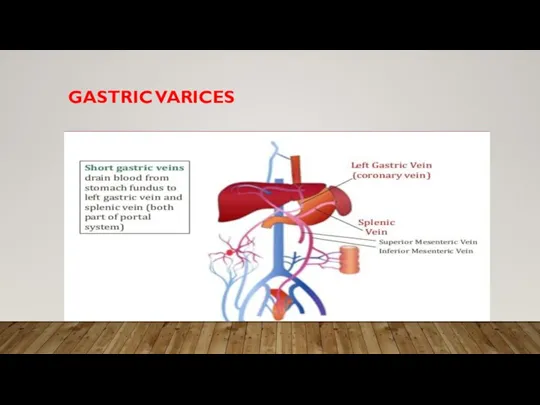
- 14. GASTRIC VARICES
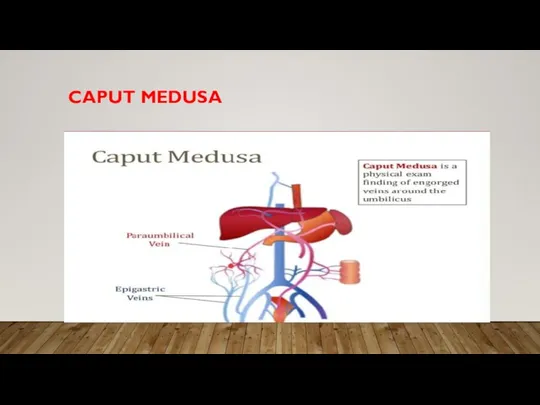
- 15. CAPUT MEDUSA
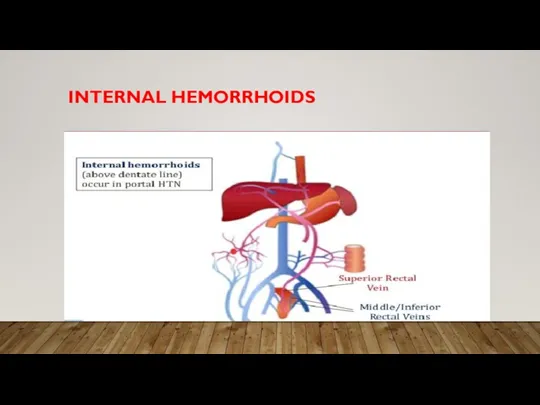
- 16. INTERNAL HEMORRHOIDS
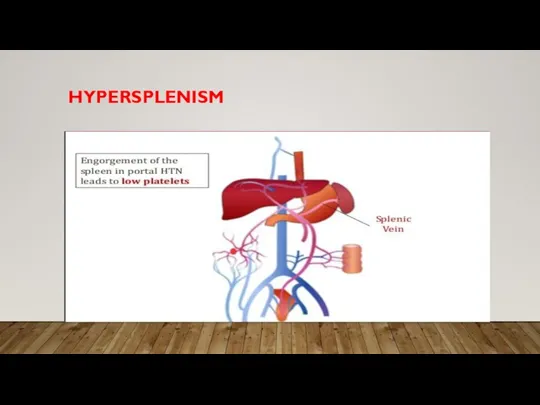
- 17. HYPERSPLENISM
- 18. PORTAL VEIN THROMBOSIS • Rare cause of portal hypertension • Acute onset abdominal pain • Splenomegaly
- 19. ASCITES • Accumulation of fluid in peritoneal cavity • In liver disease, from portal hypertension +/-
- 20. SAAG SERUM ASCITES ALBUMIN GRADIENT • Test of ascitic fluid • Two reasons for new/worsening ascites
- 21. SAAG SERUM ASCITES ALBUMIN GRADIENT • SAAG >1.1 g/dL • Large difference between serum and ascites
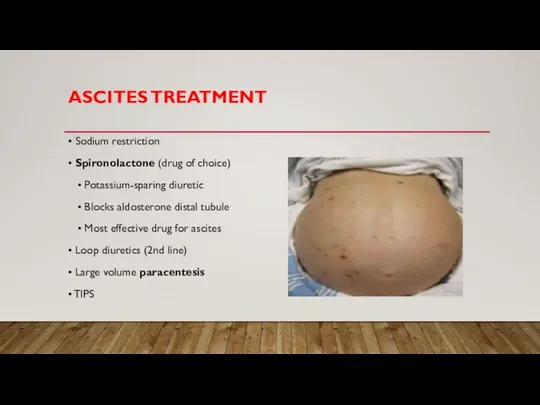
- 22. ASCITES TREATMENT • Sodium restriction • Spironolactone (drug of choice) • Potassium-sparing diuretic • Blocks aldosterone
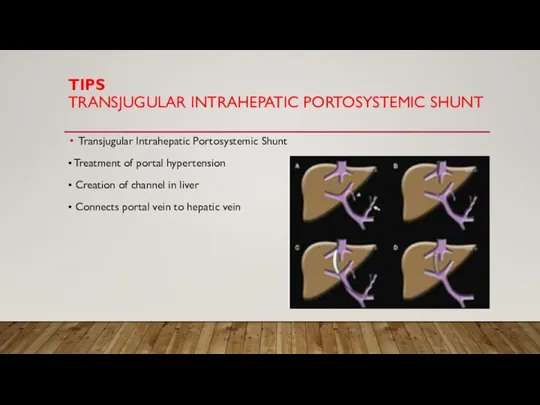
- 23. TIPS TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNT Transjugular Intrahepatic Portosystemic Shunt • Treatment of portal hypertension • Creation
- 24. SBP SPONTANEOUS BACTERIAL PERITONITIS • Ascitic fluid infection • Bacteria in gut gain entry into ascitic
- 25. MELD SCORE MODEL FOR END-STAGE LIVER DISEASE • Scoring system for chronic liver disease or cirrhosis
- 26. CHILD-PUGH CLASSIFICATION • Five variables to predict risk/survival • Points for encephalopathy, ascites, bilirubin, albumin, PT
- 27. CIRRHOSIS DIAGNOSIS Gold standard is liver biopsy • Not required if diagnosis is clear from history
- 29. Скачать презентацию
Слайд 3CIRRHOSIS
• Liver tissue replaced by fibrosis and nodules
• Smooth liver surface replaced
CIRRHOSIS
• Liver tissue replaced by fibrosis and nodules
• Smooth liver surface replaced
Слайд 4CLINICAL FEATURES
• Hyperammonemia
• Asterixis, confusion, coma
CLINICAL FEATURES
• Hyperammonemia
• Asterixis, confusion, coma
Слайд 5HYPERAMMONEMIA
TREATMENT
• Low protein diet
• Lactulose
• Synthetic disaccharide (laxative)
HYPERAMMONEMIA
TREATMENT
• Low protein diet
• Lactulose
• Synthetic disaccharide (laxative)
Слайд 6CIRRHOSIS
CLINICAL FEATURES
• Jaundice
• Loss of bilirubin metabolism
• Hypoglycemia
• Loss
CIRRHOSIS
CLINICAL FEATURES
• Jaundice
• Loss of bilirubin metabolism
• Hypoglycemia
• Loss
Слайд 7• Elevated estrogen
• Normally removed by liver
• Gynecomastia in
• Elevated estrogen
• Normally removed by liver
• Gynecomastia in
Слайд 8CAPILLARY FLUID SHIFTS
• Capillary hydrostatic pressure (Pc)
• Drives fluid out of
CAPILLARY FLUID SHIFTS
• Capillary hydrostatic pressure (Pc)
• Drives fluid out of
Слайд 9PORTAL HYPERTENSION
• Blood flows portal vein → liver → hepatic vein
• Cirrhosis
PORTAL HYPERTENSION
• Blood flows portal vein → liver → hepatic vein
• Cirrhosis
Слайд 10CIRRHOSIS
CIRRHOSIS
Слайд 11ASCITES AND EDEMA
ASCITES AND EDEMA
Слайд 12VENOUS COLLATERALS
VENOUS ANASTAMOSES
• High portal pressure opens “venous collaterals”
• Connection between
VENOUS COLLATERALS
VENOUS ANASTAMOSES
• High portal pressure opens “venous collaterals”
• Connection between
Слайд 13ESOPHAGEAL VARICES
ESOPHAGEAL VARICES
Слайд 14GASTRIC VARICES
GASTRIC VARICES
Слайд 15CAPUT MEDUSA
CAPUT MEDUSA
Слайд 16INTERNAL HEMORRHOIDS
INTERNAL HEMORRHOIDS
Слайд 17HYPERSPLENISM
HYPERSPLENISM
Слайд 18PORTAL VEIN THROMBOSIS
• Rare cause of portal hypertension
• Acute onset abdominal
PORTAL VEIN THROMBOSIS
• Rare cause of portal hypertension
• Acute onset abdominal
Слайд 19ASCITES
• Accumulation of fluid in peritoneal cavity
• In liver disease, from
ASCITES
• Accumulation of fluid in peritoneal cavity
• In liver disease, from
Слайд 20SAAG
SERUM ASCITES ALBUMIN GRADIENT
• Test of ascitic fluid
• Two reasons
SAAG
SERUM ASCITES ALBUMIN GRADIENT
• Test of ascitic fluid
• Two reasons
Слайд 21SAAG
SERUM ASCITES ALBUMIN GRADIENT
• SAAG >1.1 g/dL
• Large difference
SAAG
SERUM ASCITES ALBUMIN GRADIENT
• SAAG >1.1 g/dL
• Large difference
Слайд 22ASCITES TREATMENT
• Sodium restriction
• Spironolactone (drug of choice)
• Potassium-sparing diuretic
ASCITES TREATMENT
• Sodium restriction
• Spironolactone (drug of choice)
• Potassium-sparing diuretic
Слайд 23TIPS
TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNT
Transjugular Intrahepatic Portosystemic Shunt
• Treatment of portal
TIPS
TRANSJUGULAR INTRAHEPATIC PORTOSYSTEMIC SHUNT
Transjugular Intrahepatic Portosystemic Shunt
• Treatment of portal
Слайд 24SBP
SPONTANEOUS BACTERIAL PERITONITIS
• Ascitic fluid infection
• Bacteria in gut gain
SBP
SPONTANEOUS BACTERIAL PERITONITIS
• Ascitic fluid infection
• Bacteria in gut gain
Слайд 25MELD SCORE
MODEL FOR END-STAGE LIVER DISEASE
• Scoring system for chronic liver
MELD SCORE
MODEL FOR END-STAGE LIVER DISEASE
• Scoring system for chronic liver
Слайд 26CHILD-PUGH CLASSIFICATION
• Five variables to predict risk/survival
• Points for encephalopathy,
CHILD-PUGH CLASSIFICATION
• Five variables to predict risk/survival
• Points for encephalopathy,
Слайд 27CIRRHOSIS
DIAGNOSIS
Gold standard is liver biopsy
• Not required if diagnosis is
CIRRHOSIS
DIAGNOSIS
Gold standard is liver biopsy
• Not required if diagnosis is
 Алынғнан нәтижелерді түсіндіру үшін ақпараттық қолдау
Алынғнан нәтижелерді түсіндіру үшін ақпараттық қолдау Основы фармакогнозии. Основные группы биологически активных соединений (БАС). Основные принципы фитотерапии
Основы фармакогнозии. Основные группы биологически активных соединений (БАС). Основные принципы фитотерапии Строение ВНЧС в норме, при дистальном и мезиальном прикусах
Строение ВНЧС в норме, при дистальном и мезиальном прикусах Рекомендации по питанию
Рекомендации по питанию Partie antibio pdf corrections
Partie antibio pdf corrections Реактивность организма
Реактивность организма Опорно-двигательная система
Опорно-двигательная система Иммунокоррекция больного при лечении туберкулёза
Иммунокоррекция больного при лечении туберкулёза Диф. Диагностика
Диф. Диагностика Нутритивная поддержка пациентов, нуждающихся в паллиативной помощи
Нутритивная поддержка пациентов, нуждающихся в паллиативной помощи Жулдикораева
Жулдикораева Сироп из фиников
Сироп из фиников Анатомо-физиологические особенности детей старшего возраста
Анатомо-физиологические особенности детей старшего возраста Моделирование ожогов (критический обзор литературы и собственные разработки)
Моделирование ожогов (критический обзор литературы и собственные разработки) Умные системы повсеместного здравоохранения: исследования и перспективы
Умные системы повсеместного здравоохранения: исследования и перспективы Влияние токсичных веществ выделяемых из базисов стоматологических протезов, на организм человека
Влияние токсичных веществ выделяемых из базисов стоматологических протезов, на организм человека Реабилитация пациентов при заболеваниях обмена веществ, в хирургии
Реабилитация пациентов при заболеваниях обмена веществ, в хирургии Рекомендации по диагностике и лечению хронической тромбоэмболической легочной гипертензии (часть I)
Рекомендации по диагностике и лечению хронической тромбоэмболической легочной гипертензии (часть I) Заболевания щитовидной железы и беременность
Заболевания щитовидной железы и беременность Лимфа жүйесінің құрылысы
Лимфа жүйесінің құрылысы Физиология кровообращения
Физиология кровообращения Мутация клетки кроветворной системы. Опухоли системы крови
Мутация клетки кроветворной системы. Опухоли системы крови Регуляция кровообращения
Регуляция кровообращения Мұнай өнімдерінің (бензол,толуол) теріге әсері
Мұнай өнімдерінің (бензол,толуол) теріге әсері Индикаторы работы рентгенологического отделения
Индикаторы работы рентгенологического отделения Системный анализ и организация здравоохранения. Методологические основы системного анализа
Системный анализ и организация здравоохранения. Методологические основы системного анализа Новые возможности в лечении вируса гепатита С. Викейра пак
Новые возможности в лечении вируса гепатита С. Викейра пак ГИГИЕНА ПИТАНИЯ В МУНИЦИПАЛЬНОМ КАЗЕННОМ ДОШКОЛЬНОМ ОБРАЗОВАТЕЛЬНОМ УЧРЕЖДЕНИИ
ГИГИЕНА ПИТАНИЯ В МУНИЦИПАЛЬНОМ КАЗЕННОМ ДОШКОЛЬНОМ ОБРАЗОВАТЕЛЬНОМ УЧРЕЖДЕНИИ