- colonf

Содержание
- 2. anatomy
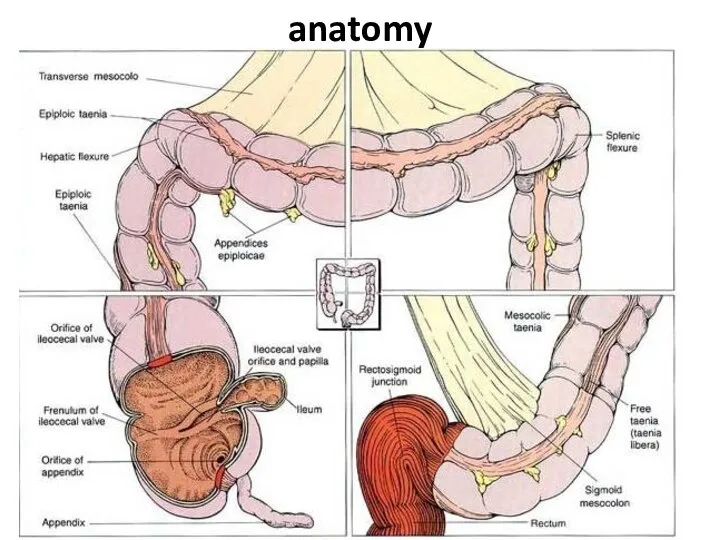
- 3. anatomy
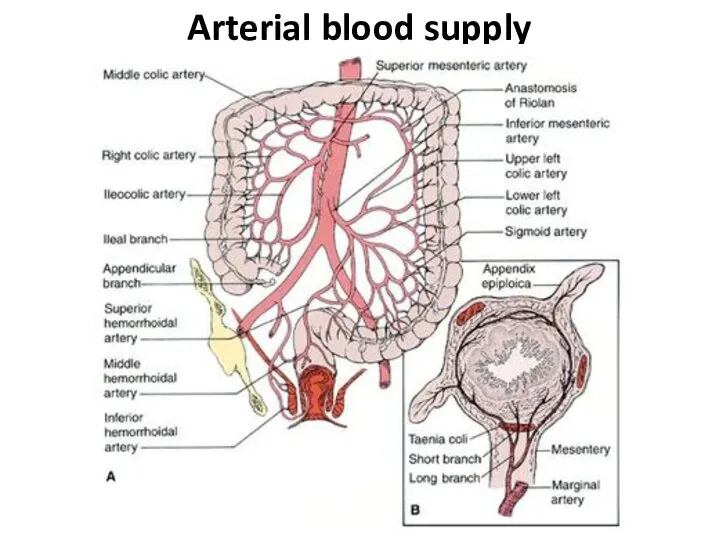
- 4. Arterial blood supply
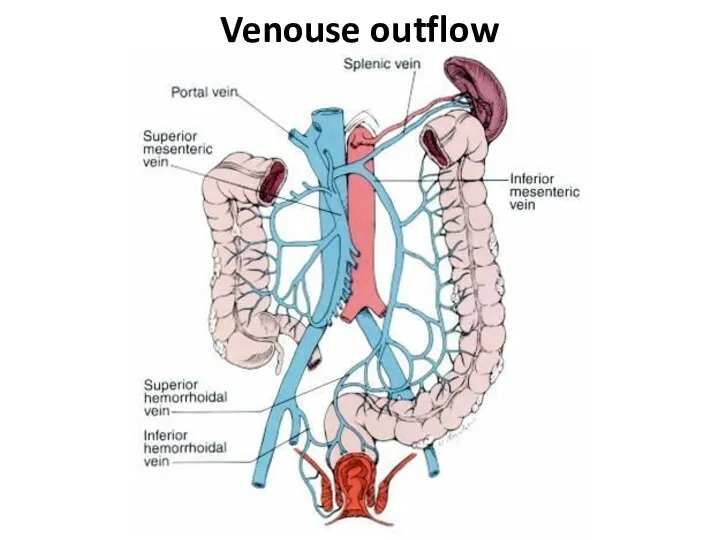
- 5. Venouse outflow
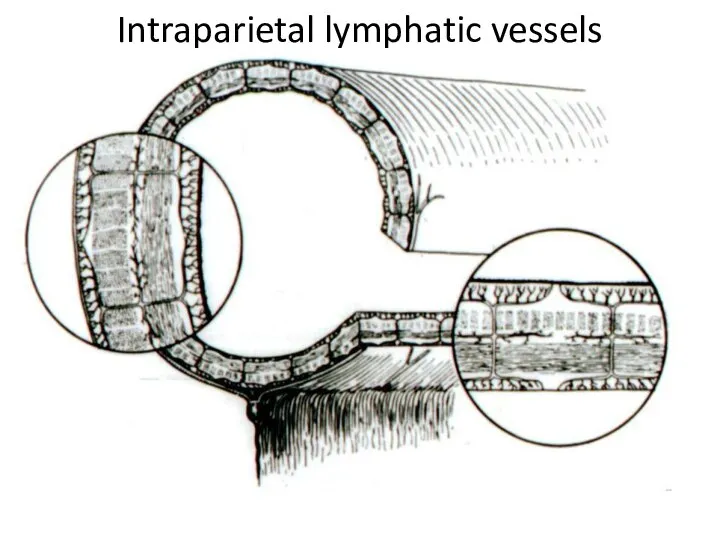
- 6. Intraparietal lymphatic vessels
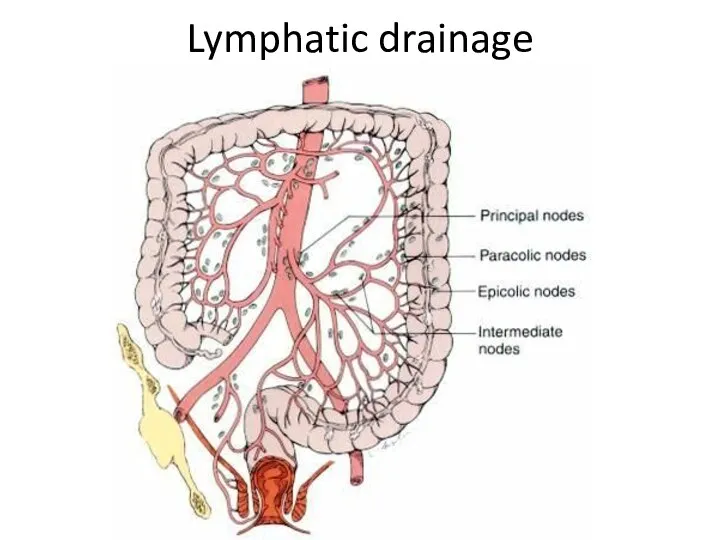
- 7. Lymphatic drainage
- 8. Differences of the right and left half Anatomy: on the right the lumen is wider, than
- 9. Special investigation methods 1. Physical investiga-tion 2. A proctosigmoido-scopy 3. Fibrocolonoscopy
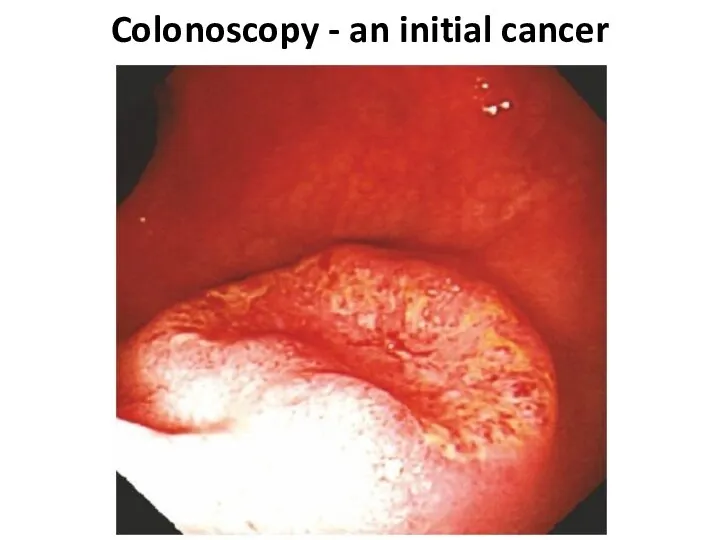
- 10. Colonoscopy - an initial cancer
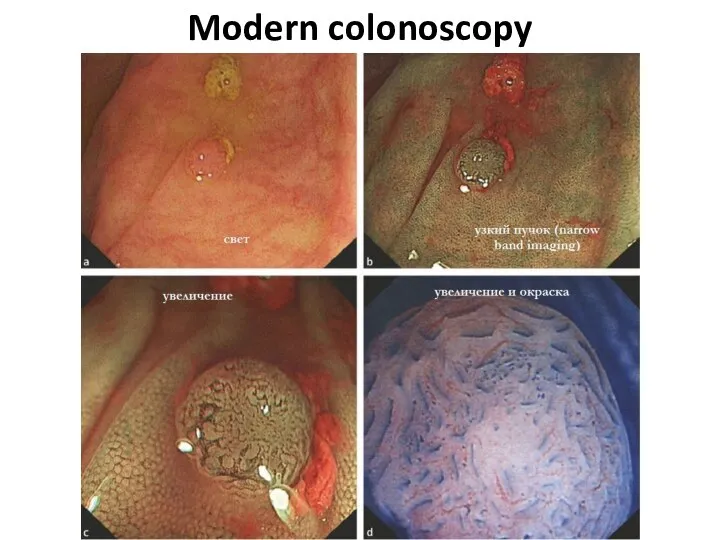
- 11. Modern colonoscopy
- 12. Special investigation methods 4. irrigoscopy (including virtu-al) 5. abdominal cavity US 6. radial methods (CТ, PET,
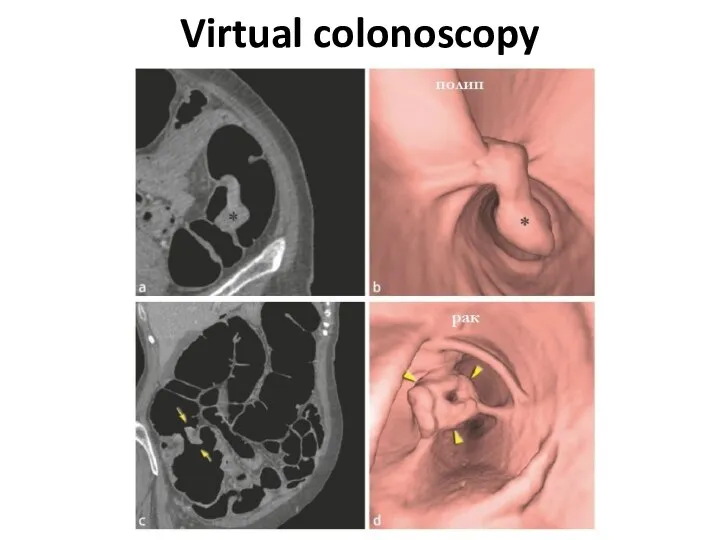
- 13. Virtual colonoscopy
- 14. At what a cancer localization more often anemy?
- 15. At what a cancer localization more often Visible bleeding?
- 16. AT WHAT A CANCER LOCALIZATION MORE OFTEN Disturbance of passability
- 17. AT WHAT A CANCER LOCALIZATION MORE OFTEN Perforation is more possible?
- 18. AT WHAT A CANCER LOCALIZATION MORE OFTEN Fistulas, phlegmons are possible?
- 19. Colon cancer localisation
- 20. Cancer clinical signs 1. Functional signs without intestinal disorders (a pain, etc.) 2. Intestinal disorders (diarrheas,
- 21. Cancer clinical forms 1) toxico-anemic 2) enterocolitic 3) dyspeptic 4) obturational 5) pseudo-inflammatory 6) tumoral
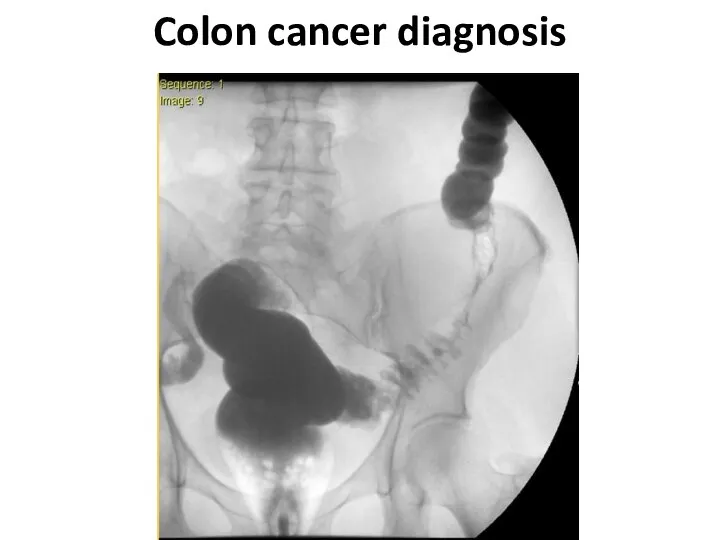
- 22. Colon cancer diagnosis
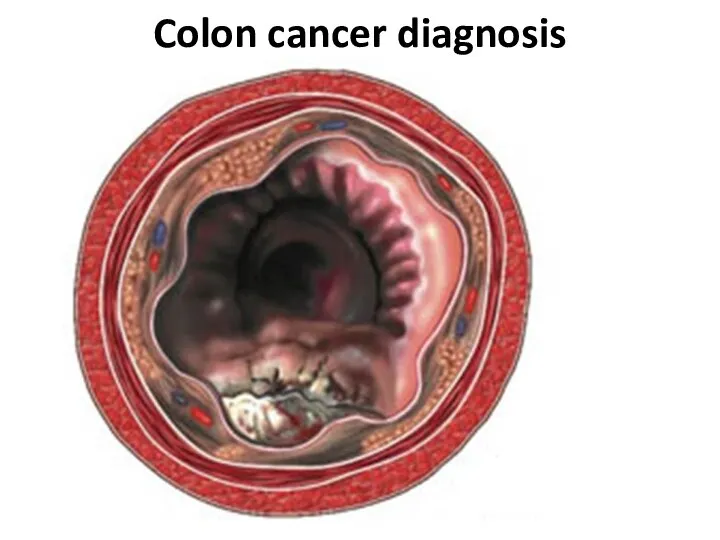
- 23. Colon cancer diagnosis
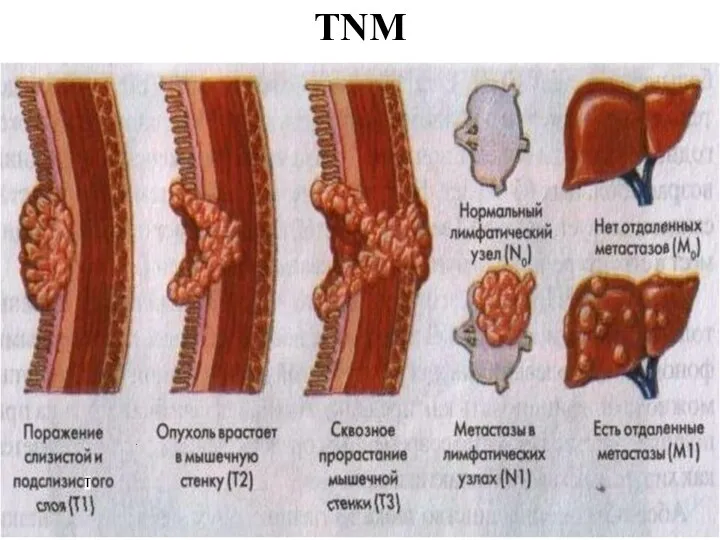
- 26. TNM
- 27. TNM - T Tx - the estimation of a primary tumour is impossible T0 - the
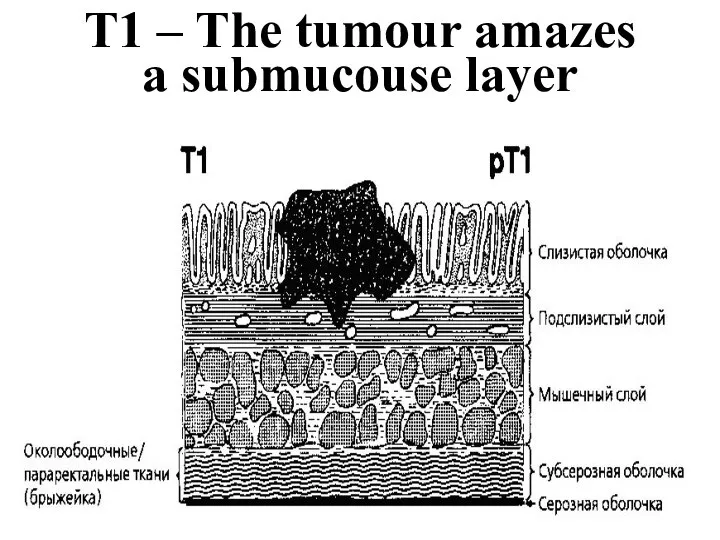
- 28. T1 – The tumour amazes a submucouse layer
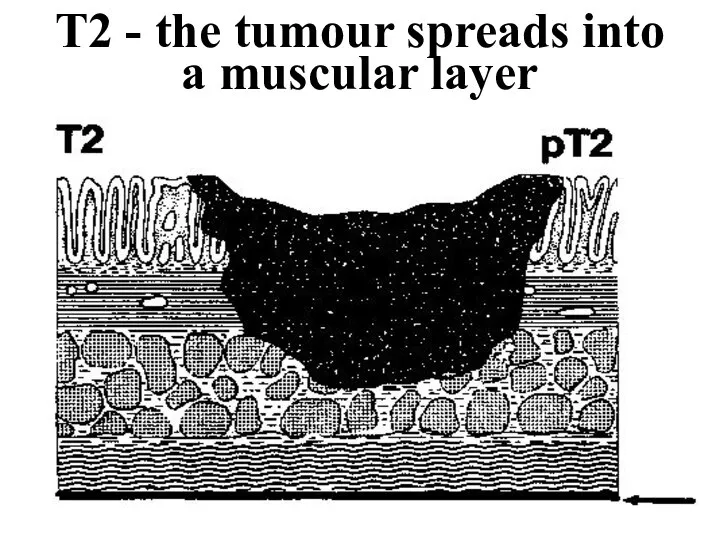
- 29. T2 - the tumour spreads into a muscular layer
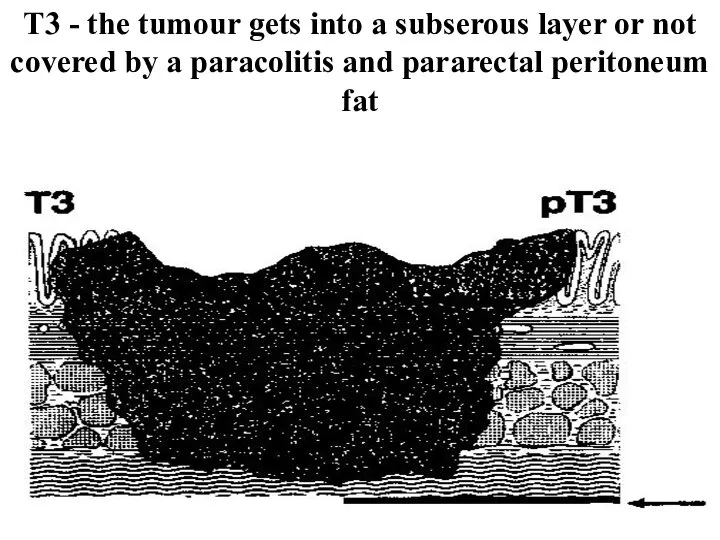
- 30. Т3 - the tumour gets into a subserous layer or not covered by a paracolitis and
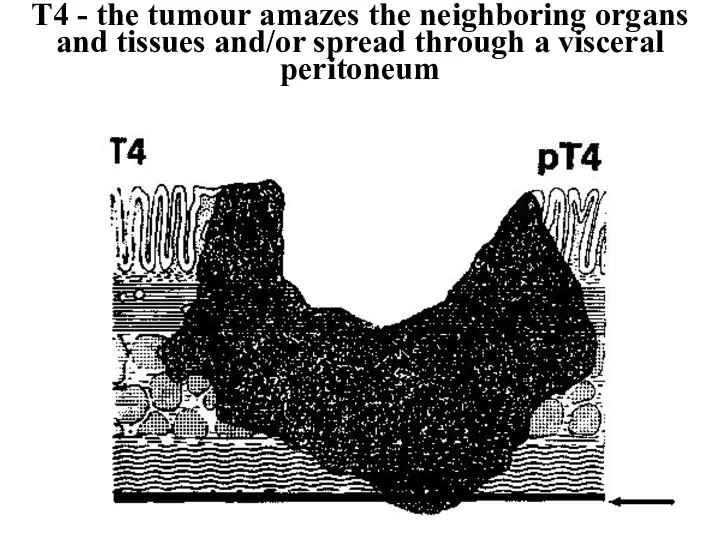
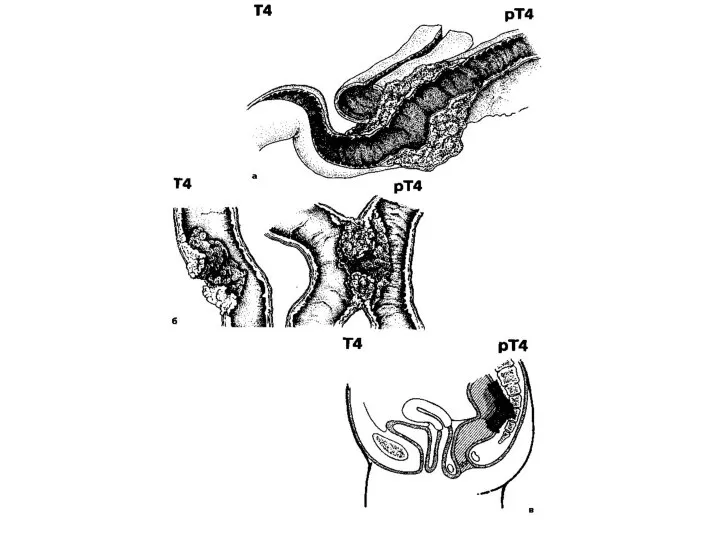
- 31. Т4 - the tumour amazes the neighboring organs and tissues and/or spread through a visceral peritoneum
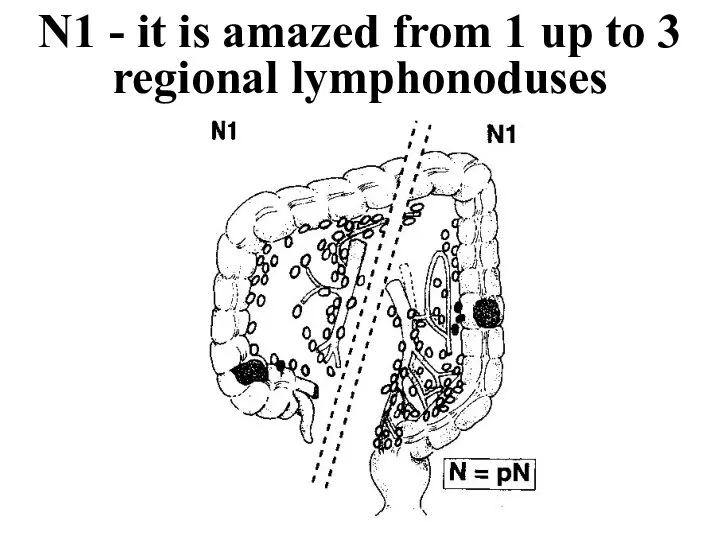
- 33. N1 - it is amazed from 1 up to 3 regional lymphonoduses
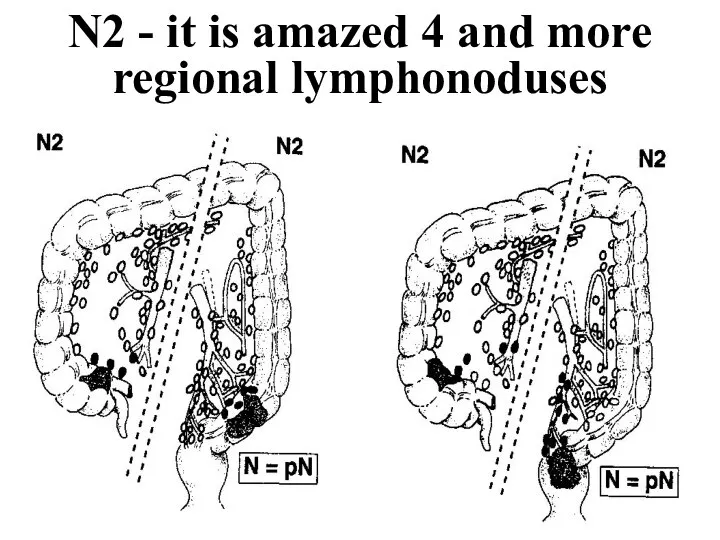
- 34. N2 - it is amazed 4 and more regional lymphonoduses
- 35. Manual suturing of an intestine
- 36. Staplers
- 37. Hardware seam
- 38. Hardware seam
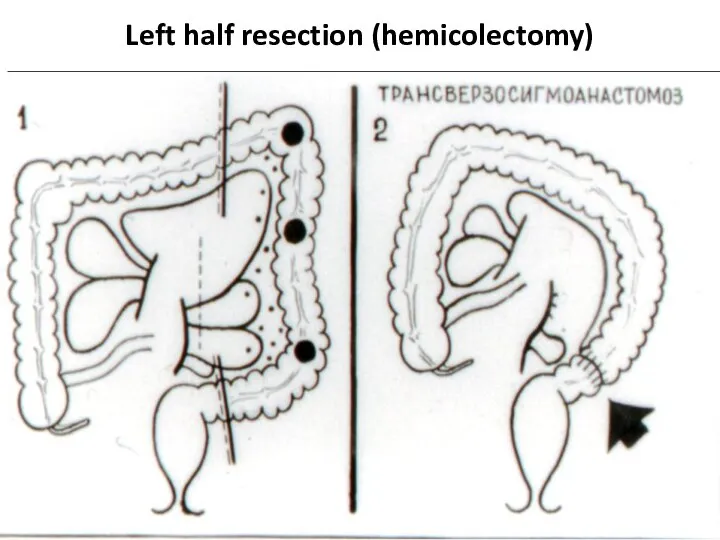
- 39. Left half resection (hemicolectomy)
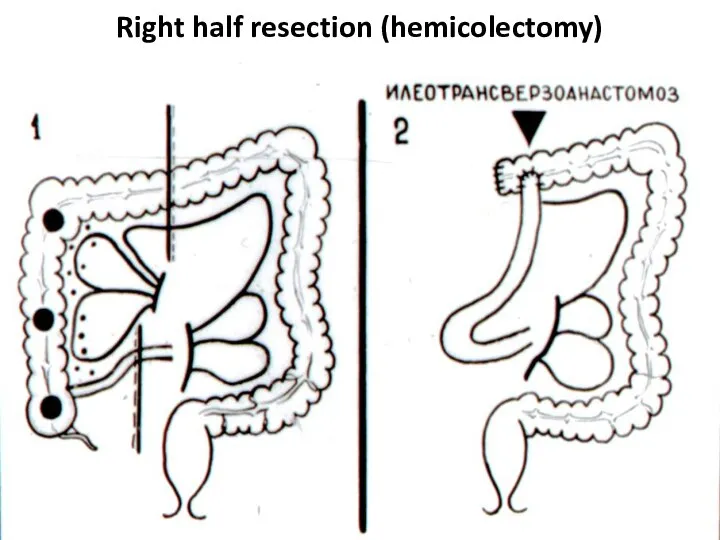
- 40. Right half resection (hemicolectomy)
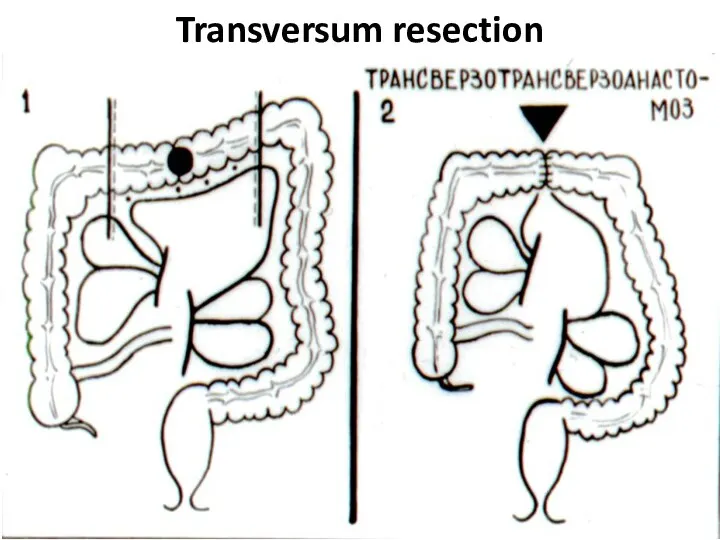
- 41. Transversum resection
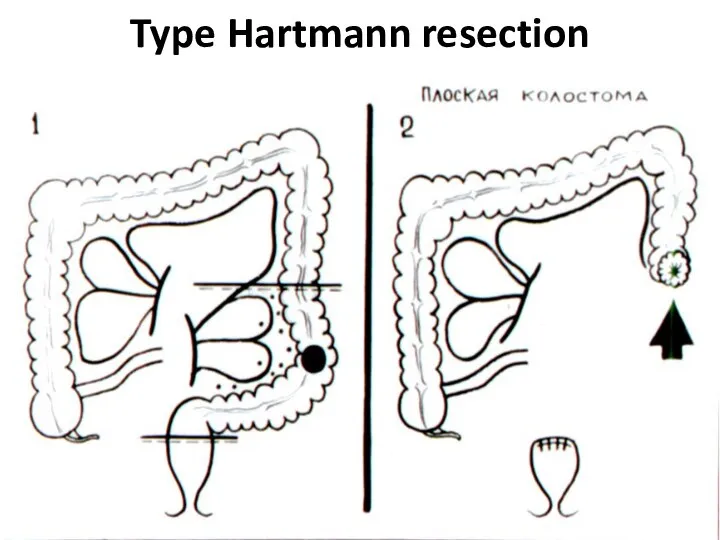
- 42. Type Hartmann resection
- 43. Terminal flat colostomy on E.G.Topuzov
- 44. Terminal flat colostomy on E.G.Topuzov
- 45. Terminal flat colostomy on E.G.Topuzov
- 46. Terminal flat colostomy on E.G.Topuzov
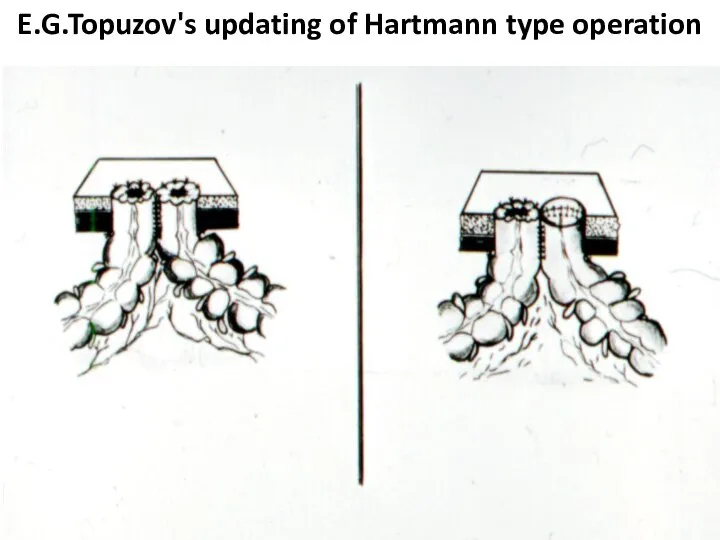
- 47. E.G.Topuzov's updating of Hartmann type operation
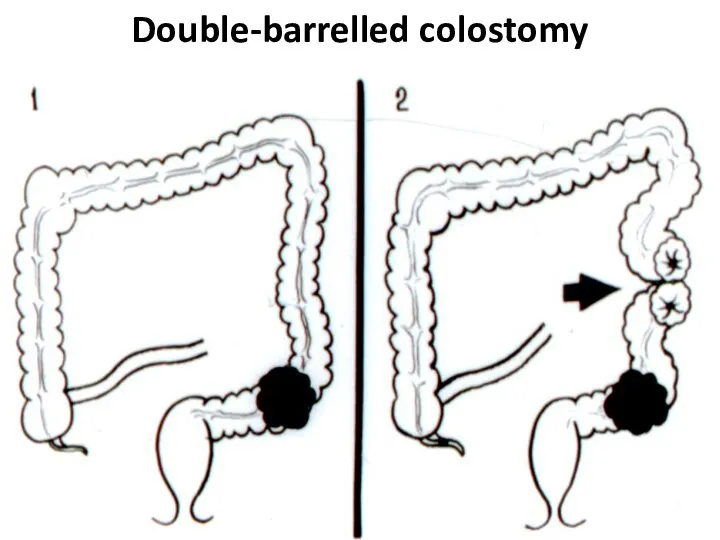
- 48. Double-barrelled colostomy
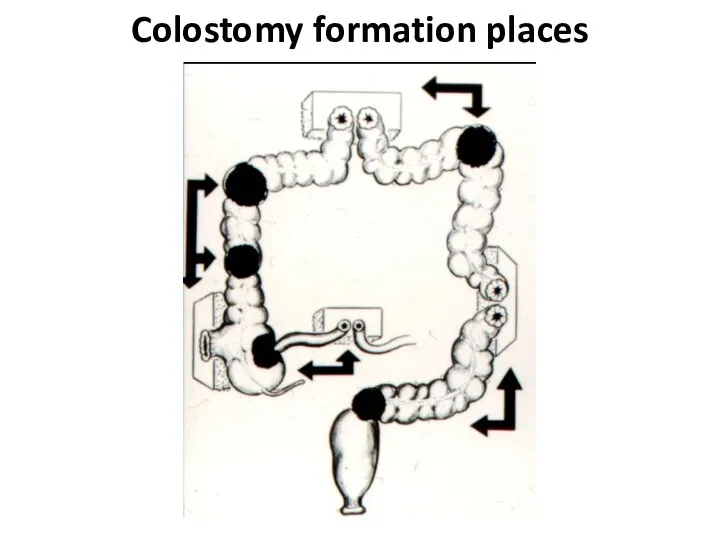
- 49. Colostomy formation places
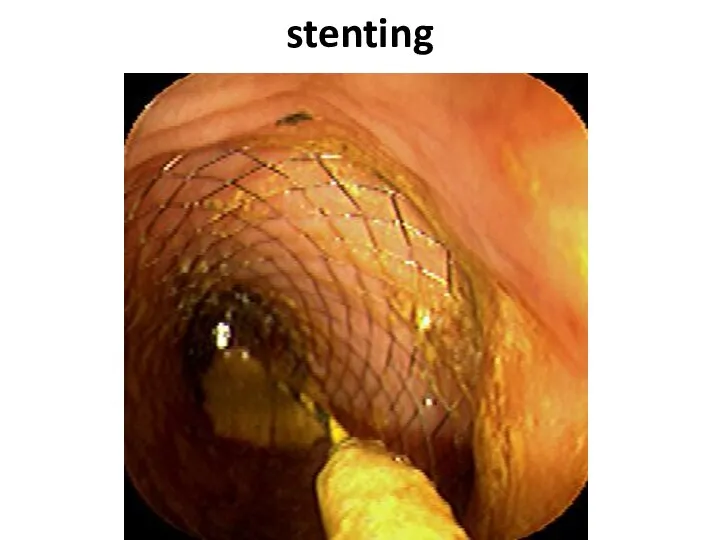
- 50. stenting
- 51. stenting
- 52. complications The intestinal obstruction is most typical for a tu-mor localization in the colon left half
- 53. complications The inflammation in tissues surrounding a tumour (up to phlegmon or abscess de-velopment) is marked
- 54. Question Pain in the right ileal region, a tumour and a heat. With what diseases you
- 55. complications Perforation of an intestine can be as in a zone of the tumour, at its
- 56. Question At what colon can-cer complication Schetkin-Blumberg sign more often is defined?
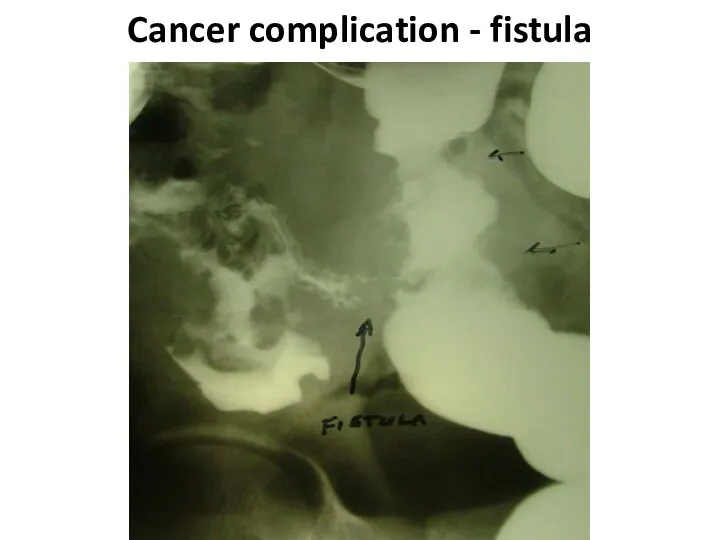
- 57. complications Formation of fistulas at spreading at the nea-rest hollow organs (co-lo-small intestinal, co-lo-gastric, colo-vesical) carry
- 58. Cancer complication - fistula
- 59. Cancer complication - fistula
- 60. Cancer complication - fistula
- 61. complications The intestinal bleeding happens, as a rule, insig-nificant. Sometimes it is shown in the form
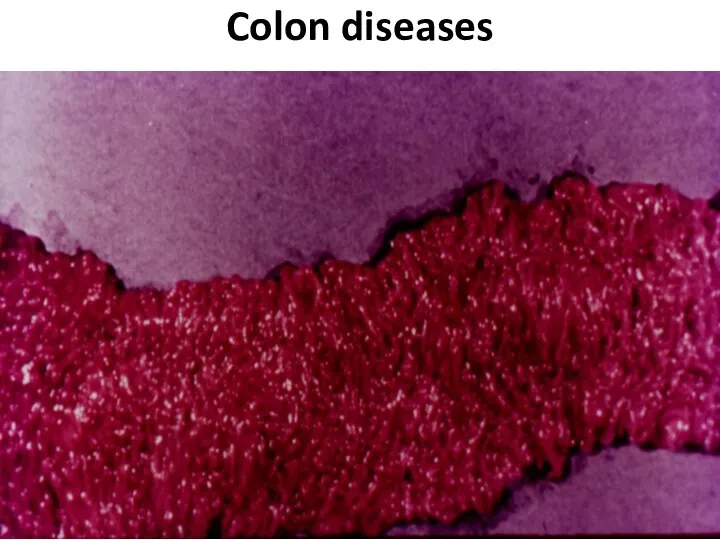
- 62. Colon diseases
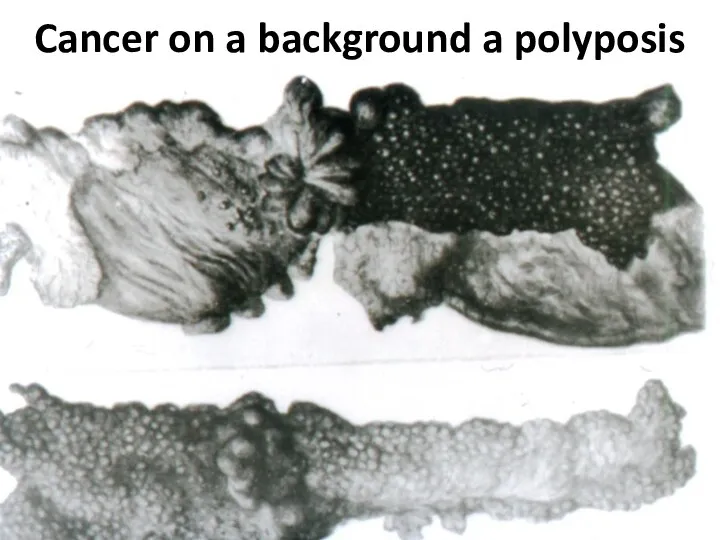
- 63. Cancer on a background a polyposis
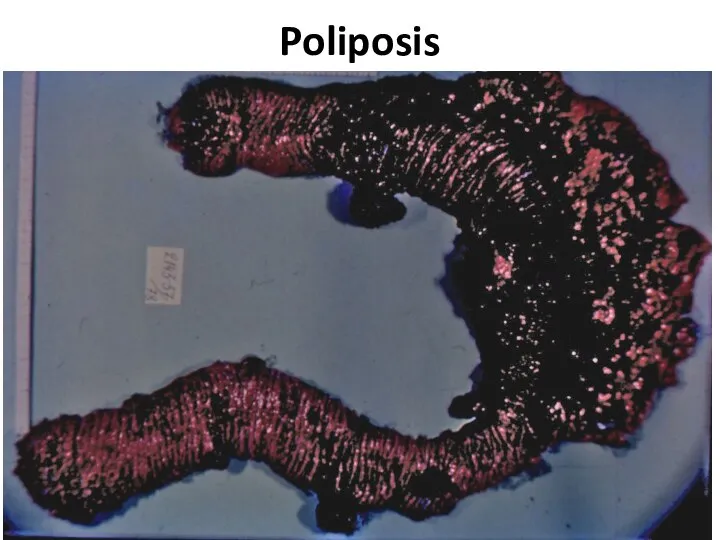
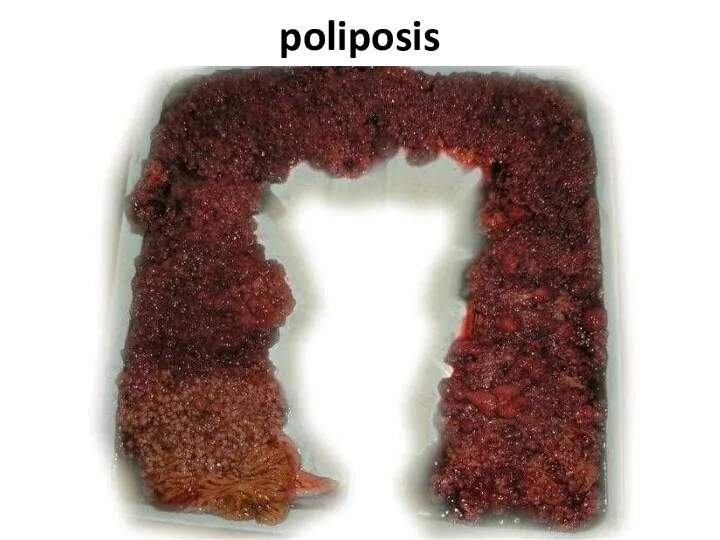
- 64. Poliposis
- 65. Nonspecific colitises 1. Ulcerouse 2. Granulomatous (Crohn's disease) 3. Ischemic
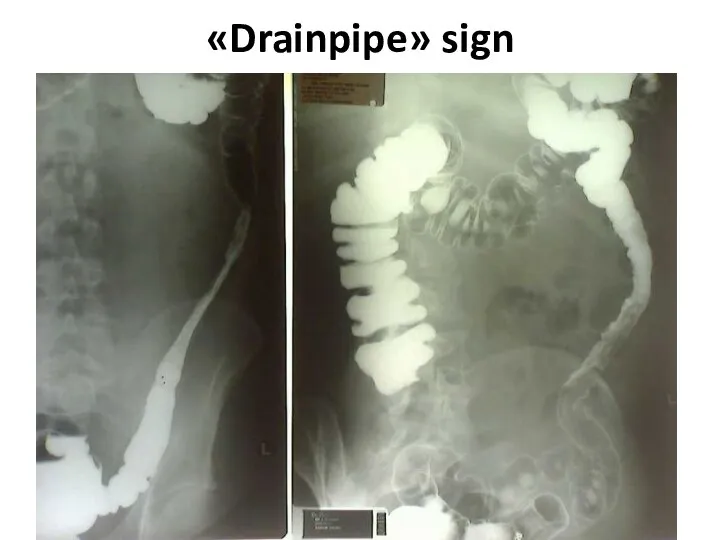
- 66. «Drainpipe» sign
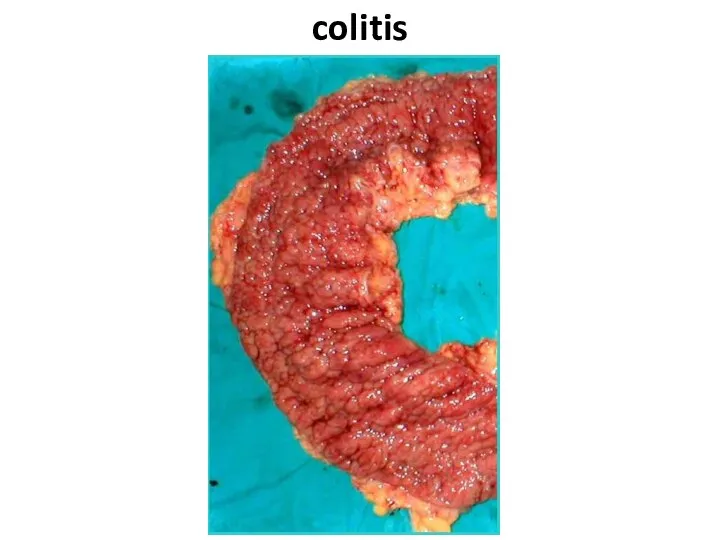
- 67. colitis
- 68. Cystous colitis
- 69. Extraintestinal displays vessels vasculitis thromboembolism liver fatty steatosis chronic active hepatitis primary sclerosing cholangitis joints peripheral
- 70. complications Toxic megacolon Perforation Peritonitis Intestinal obstruction Bleedings Abscesses Fistulas Infiltrates
- 71. Indications to operation at ulcerouse colitis Intestinal bleeding. 1. The frequency of bowel movements 12 or
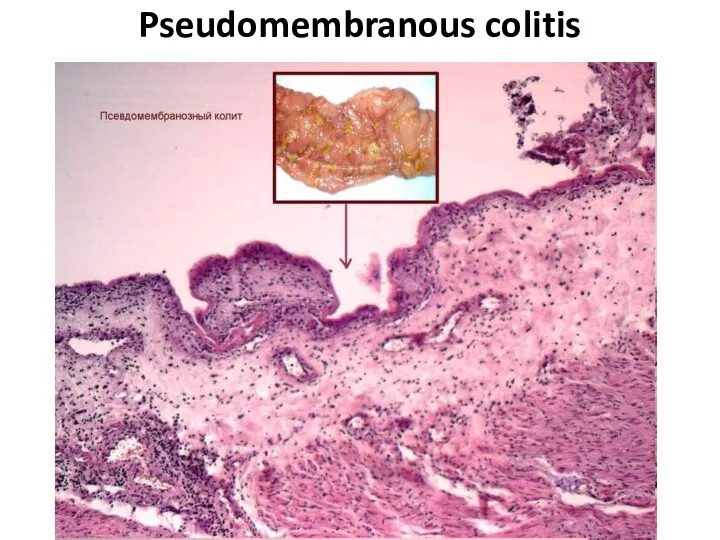
- 72. Pseudomembranous colitis
- 73. Polips Hyperplastic Tubular adenoma Tubulary-villiferous adenoma Villiferous adenoma
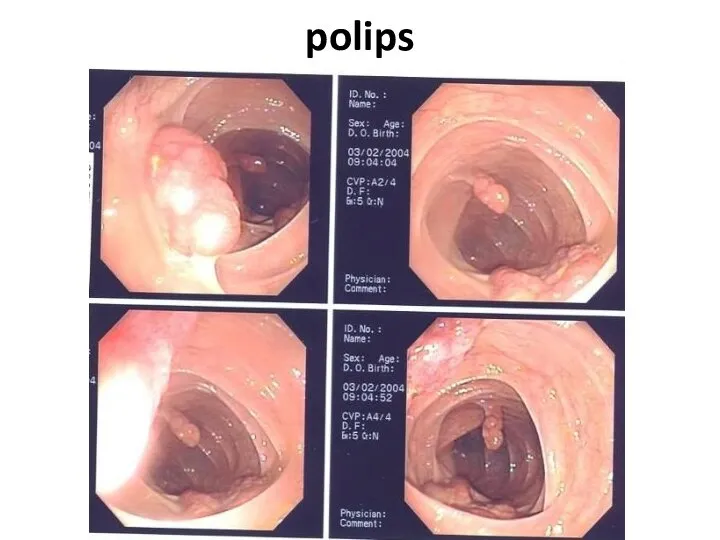
- 74. polips
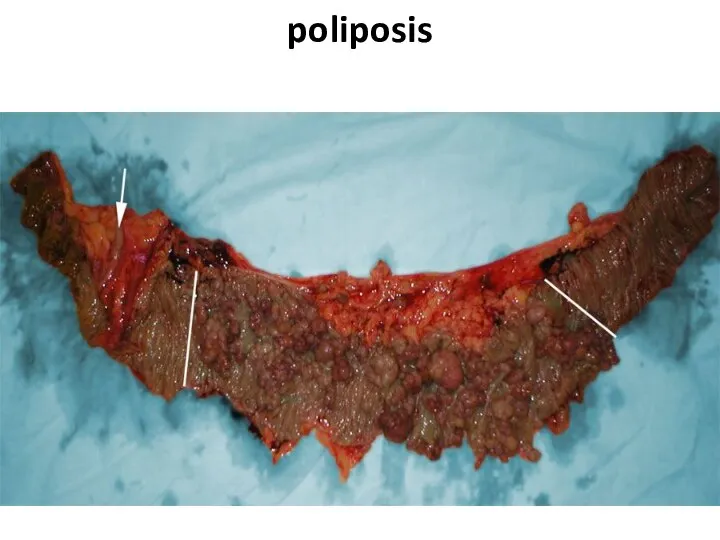
- 75. poliposis
- 76. poliposis
- 77. Congenital diseases 1. Hirshsprung disease 2. Megacolon 3. Dolichocolon
- 78. Hirshsprung disease
- 79. Differential diagnostics 1. Myxedema 2. Medicinal influences (morphinum and so forth) 5. Depressions 6. Schizophrenia 7.
- 80. diverticuls Diverticul Diverticulosis Diverticulitis
- 81. diverticul
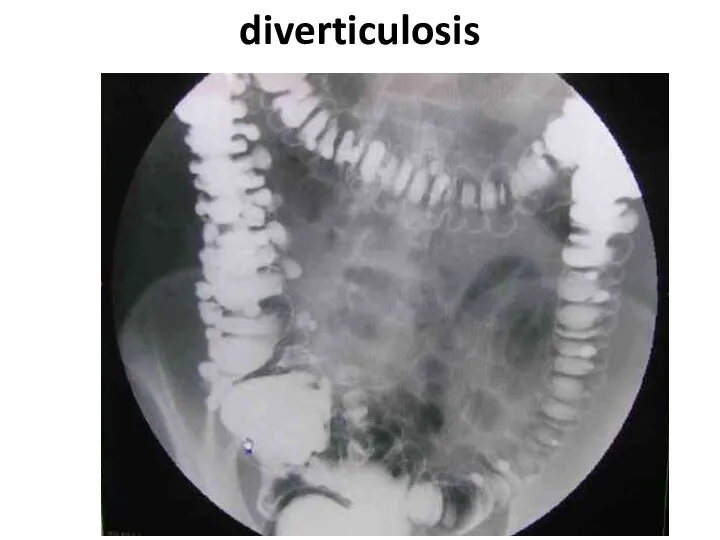
- 83. diverticulosis
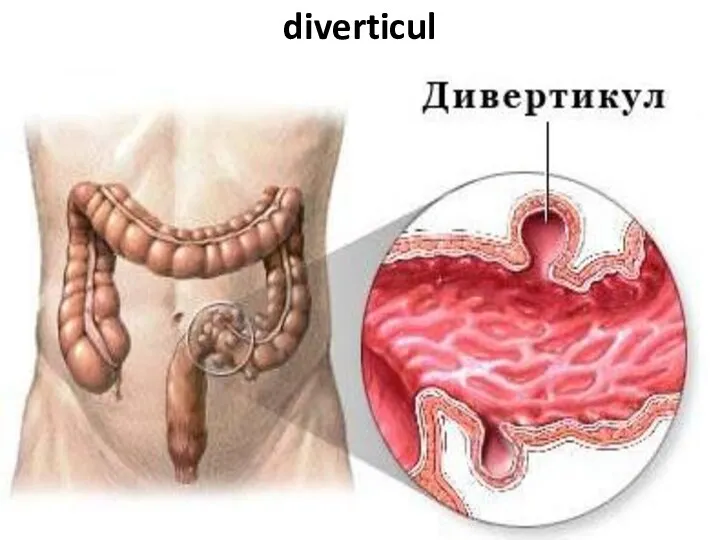
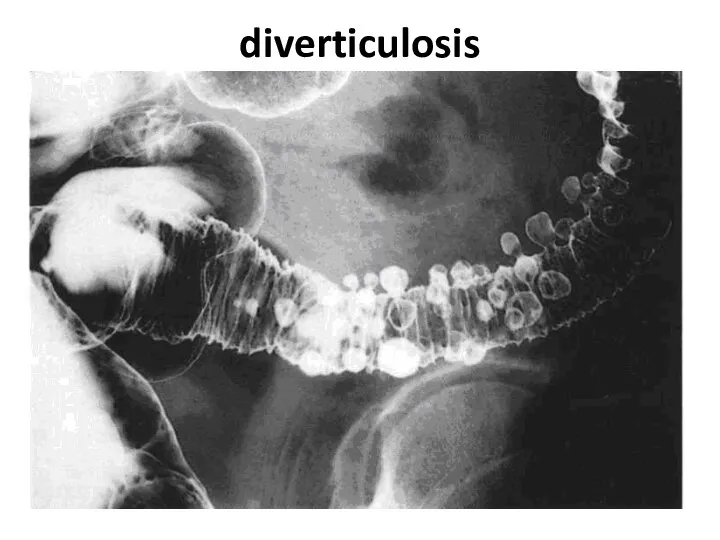
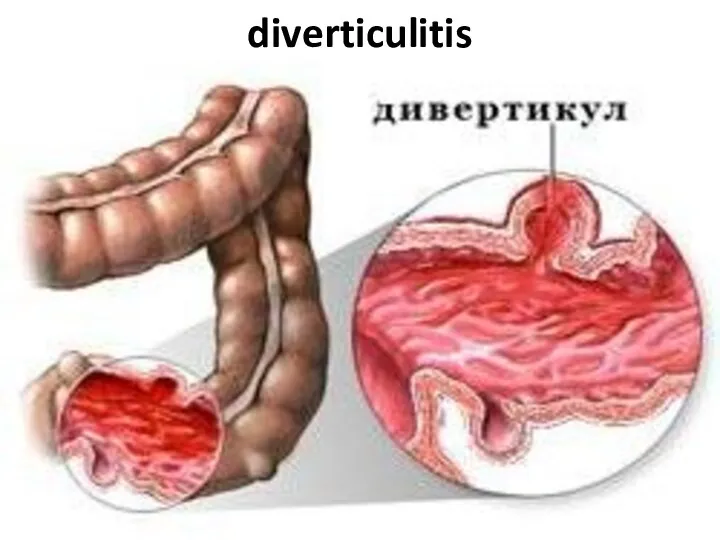
- 84. diverticulosis
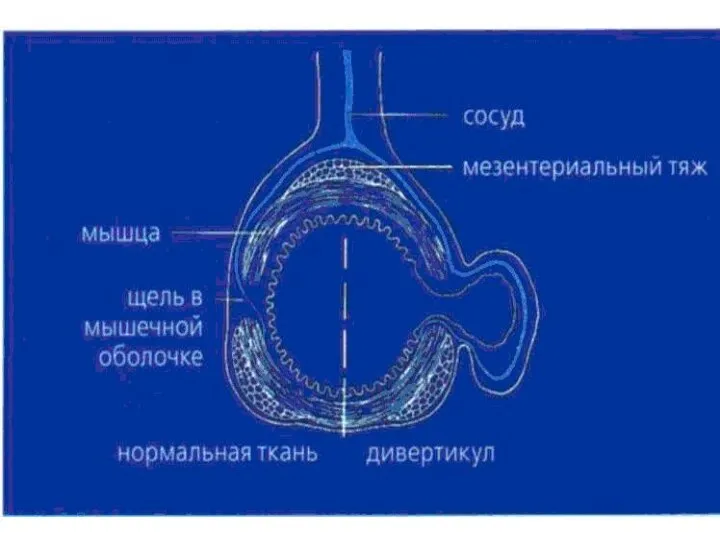
- 85. diverticuls
- 86. Multiple diverticuls
- 87. Diverticul - obturation
- 88. diverticulosis
- 89. Fecal stone in a diverticulum
- 90. diverticulitis
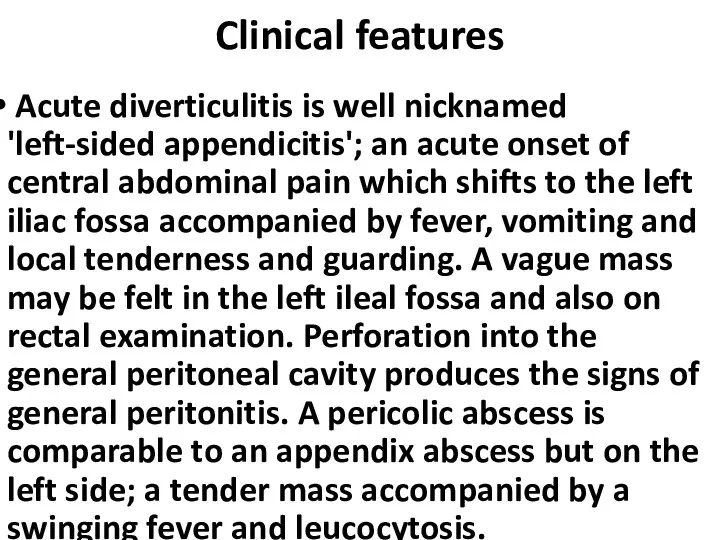
- 91. Clinical features Acute diverticulitis is well nicknamed 'left-sided appendicitis'; an acute onset of central abdominal pain
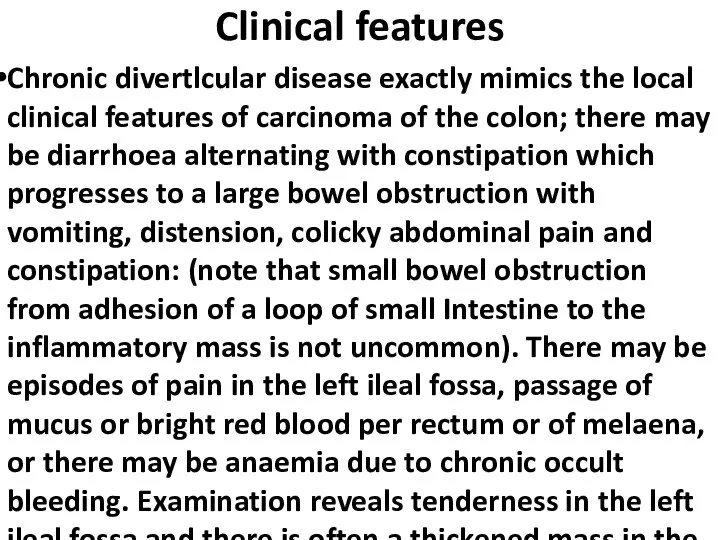
- 92. Clinical features Chronic divertlcular disease exactly mimics the local clinical features of carcinoma of the colon;
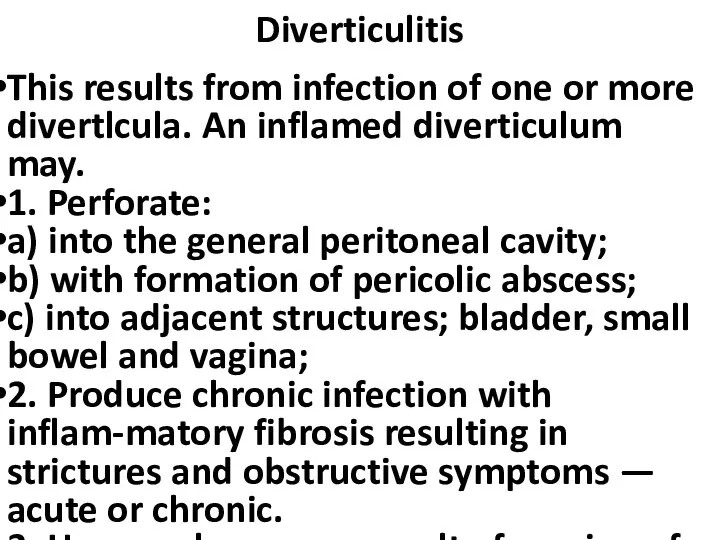
- 93. Diverticulitis This results from infection of one or more divertlcula. An inflamed diverticulum may. 1. Perforate:
- 94. Diverticulitis The Hinchey classification - proposed by Hinchey et al. in 1978[1] classifies a colonic perforation
- 95. diverticulosis, bleeding, subtotal colectomy
- 96. diverticulosis, bleeding, subtotal colectomy
- 98. Скачать презентацию
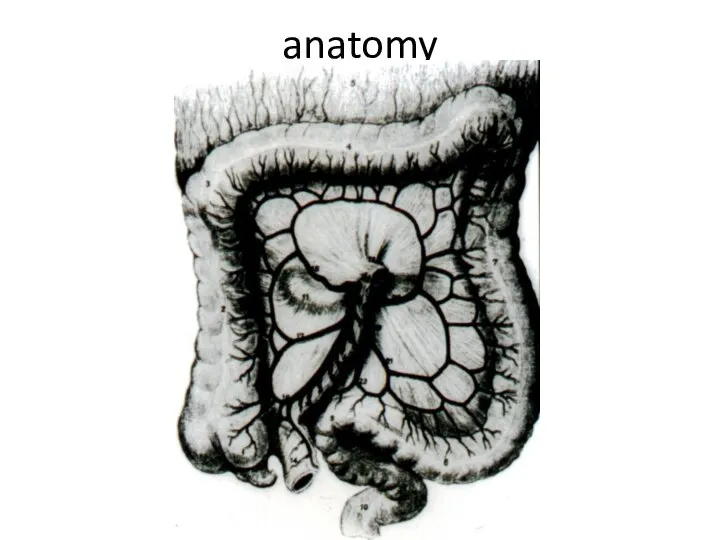
Слайд 3anatomy
anatomy
Слайд 4Arterial blood supply
Arterial blood supply
Слайд 5Venouse outflow
Venouse outflow
Слайд 6Intraparietal lymphatic vessels
Intraparietal lymphatic vessels
Слайд 7Lymphatic drainage
Lymphatic drainage
Слайд 8Differences of the right and left half
Anatomy: on the right the lumen
Differences of the right and left half
Anatomy: on the right the lumen
Слайд 9Special investigation methods
1. Physical investiga-tion
2. A proctosigmoido-scopy
3. Fibrocolonoscopy
Special investigation methods
1. Physical investiga-tion
2. A proctosigmoido-scopy
3. Fibrocolonoscopy
Слайд 10Colonoscopy - an initial cancer
Colonoscopy - an initial cancer
Слайд 11Modern colonoscopy
Modern colonoscopy
Слайд 12Special investigation methods
4. irrigoscopy (including virtu-al)
5. abdominal cavity US
6. radial methods
Special investigation methods
4. irrigoscopy (including virtu-al)
5. abdominal cavity US
6. radial methods
Слайд 13Virtual colonoscopy
Virtual colonoscopy
Слайд 14At what a cancer localization more often
anemy?
At what a cancer localization more often
anemy?
Слайд 15At what a cancer localization more often
Visible bleeding?
At what a cancer localization more often
Visible bleeding?
Слайд 16AT WHAT A CANCER LOCALIZATION MORE OFTEN
Disturbance
of passability
AT WHAT A CANCER LOCALIZATION MORE OFTEN
Disturbance
of passability
Слайд 17AT WHAT A CANCER LOCALIZATION MORE OFTEN
Perforation is more possible?
AT WHAT A CANCER LOCALIZATION MORE OFTEN
Perforation is more possible?
Слайд 18AT WHAT A CANCER LOCALIZATION MORE OFTEN
Fistulas, phlegmons are possible?
AT WHAT A CANCER LOCALIZATION MORE OFTEN
Fistulas, phlegmons are possible?
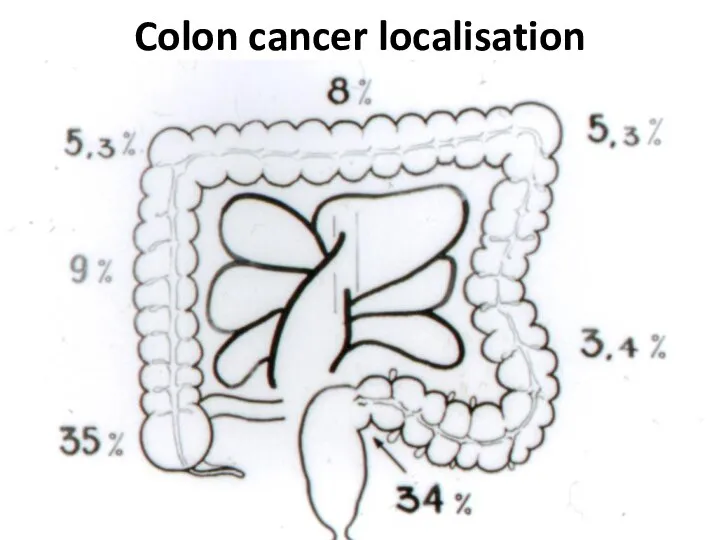
Слайд 19Colon cancer localisation
Colon cancer localisation
Слайд 20Cancer clinical signs
1. Functional signs without intestinal disorders (a pain, etc.)
2. Intestinal
Cancer clinical signs
1. Functional signs without intestinal disorders (a pain, etc.)
2. Intestinal
Слайд 21Cancer clinical forms
1) toxico-anemic
2) enterocolitic
3) dyspeptic
4) obturational
5) pseudo-inflammatory
6) tumoral
Cancer clinical forms
1) toxico-anemic
2) enterocolitic
3) dyspeptic
4) obturational
5) pseudo-inflammatory
6) tumoral
Слайд 22Colon cancer diagnosis
Colon cancer diagnosis
Слайд 23Colon cancer diagnosis
Colon cancer diagnosis

Слайд 26TNM
TNM
Слайд 27TNM - T
Tx - the estimation of a primary tumour is impossible
T0
TNM - T
Tx - the estimation of a primary tumour is impossible
T0
Слайд 28T1 – The tumour amazes
a submucouse layer
T1 – The tumour amazes
a submucouse layer
Слайд 29T2 - the tumour spreads into
a muscular layer
T2 - the tumour spreads into
a muscular layer
Слайд 30Т3 - the tumour gets into a subserous layer or not covered
Т3 - the tumour gets into a subserous layer or not covered
Слайд 31Т4 - the tumour amazes the neighboring organs and tissues and/or spread
Т4 - the tumour amazes the neighboring organs and tissues and/or spread
Слайд 33N1 - it is amazed from 1 up to 3 regional lymphonoduses
N1 - it is amazed from 1 up to 3 regional lymphonoduses
Слайд 34N2 - it is amazed 4 and more regional lymphonoduses
N2 - it is amazed 4 and more regional lymphonoduses
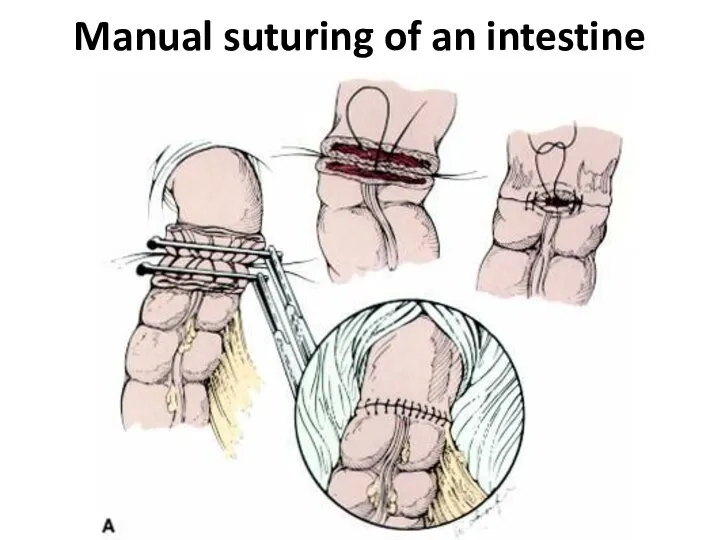
Слайд 35Manual suturing of an intestine
Manual suturing of an intestine
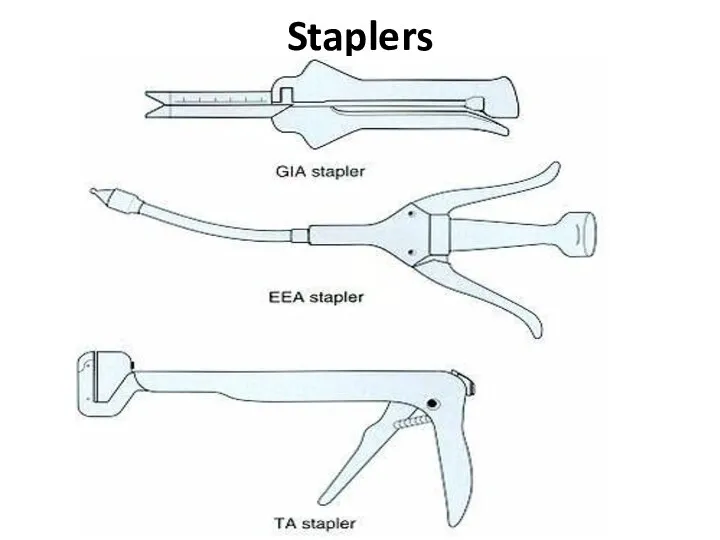
Слайд 36Staplers
Staplers
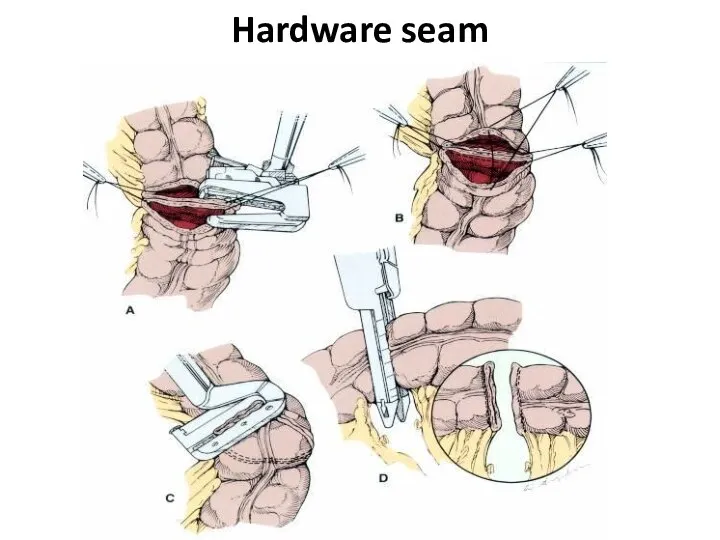
Слайд 37Hardware seam
Hardware seam
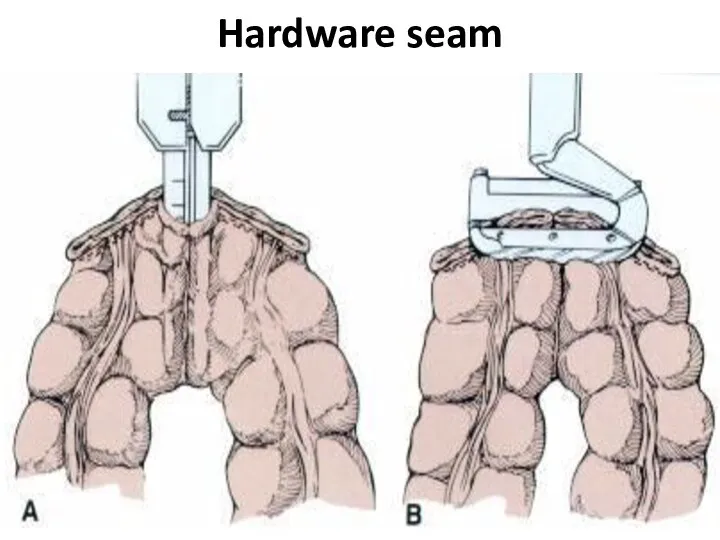
Слайд 38Hardware seam
Hardware seam
Слайд 39Left half resection (hemicolectomy)
Left half resection (hemicolectomy)
Слайд 40Right half resection (hemicolectomy)
Right half resection (hemicolectomy)
Слайд 41Transversum resection
Transversum resection
Слайд 42Type Hartmann resection
Type Hartmann resection
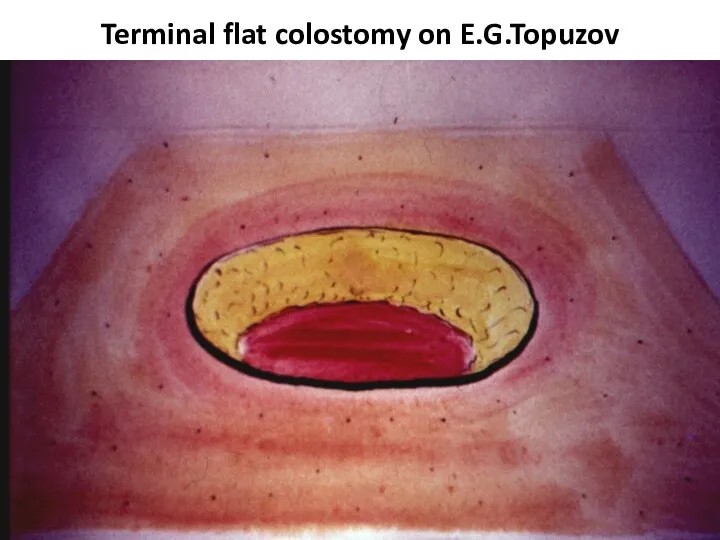
Слайд 43Terminal flat colostomy on E.G.Topuzov
Terminal flat colostomy on E.G.Topuzov
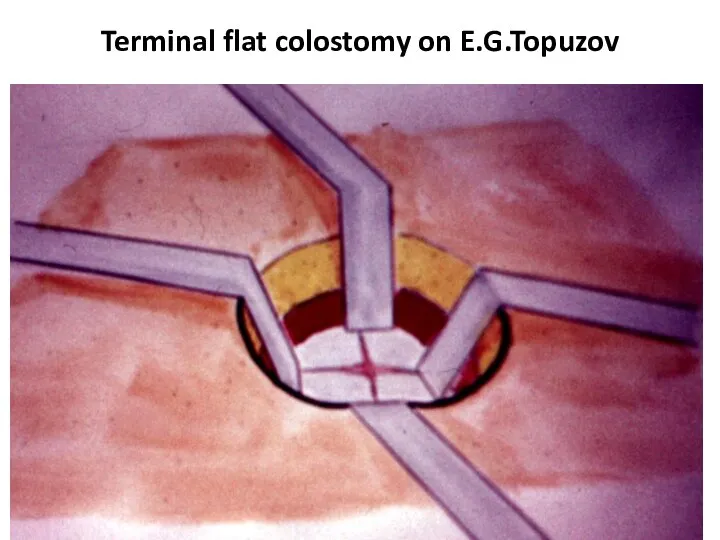
Слайд 44Terminal flat colostomy on E.G.Topuzov
Terminal flat colostomy on E.G.Topuzov
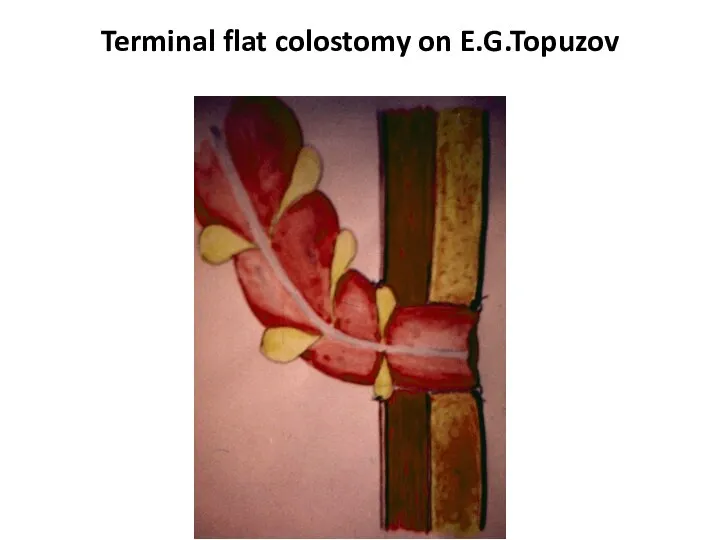
Слайд 45Terminal flat colostomy on E.G.Topuzov
Terminal flat colostomy on E.G.Topuzov
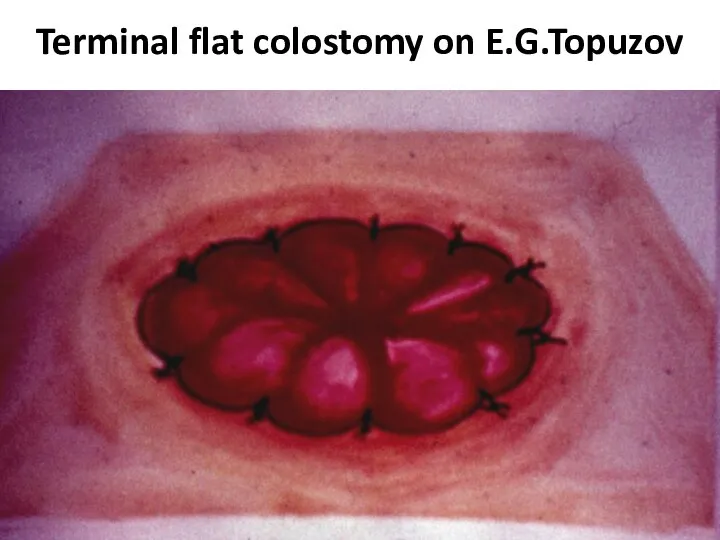
Слайд 46Terminal flat colostomy on E.G.Topuzov
Terminal flat colostomy on E.G.Topuzov
Слайд 47E.G.Topuzov's updating of Hartmann type operation
E.G.Topuzov's updating of Hartmann type operation
Слайд 48Double-barrelled colostomy
Double-barrelled colostomy
Слайд 49Colostomy formation places
Colostomy formation places
Слайд 50stenting
stenting
Слайд 51stenting
stenting

Слайд 52complications
The intestinal obstruction is most typical for a tu-mor localization in the
complications
The intestinal obstruction is most typical for a tu-mor localization in the
Слайд 53complications
The inflammation in tissues surrounding a tumour (up to phlegmon or abscess
complications
The inflammation in tissues surrounding a tumour (up to phlegmon or abscess
Слайд 54Question
Pain in the right ileal region, a tumour and a heat.
With what
Question
Pain in the right ileal region, a tumour and a heat.
With what
Слайд 55complications
Perforation of an intestine can be as in a zone of the
complications
Perforation of an intestine can be as in a zone of the
Слайд 56Question
At what colon can-cer complication Schetkin-Blumberg sign more often is defined?
Question
At what colon can-cer complication Schetkin-Blumberg sign more often is defined?
Слайд 57complications
Formation of fistulas at spreading at the nea-rest hollow organs (co-lo-small intestinal,
complications
Formation of fistulas at spreading at the nea-rest hollow organs (co-lo-small intestinal,
Слайд 58Cancer complication - fistula
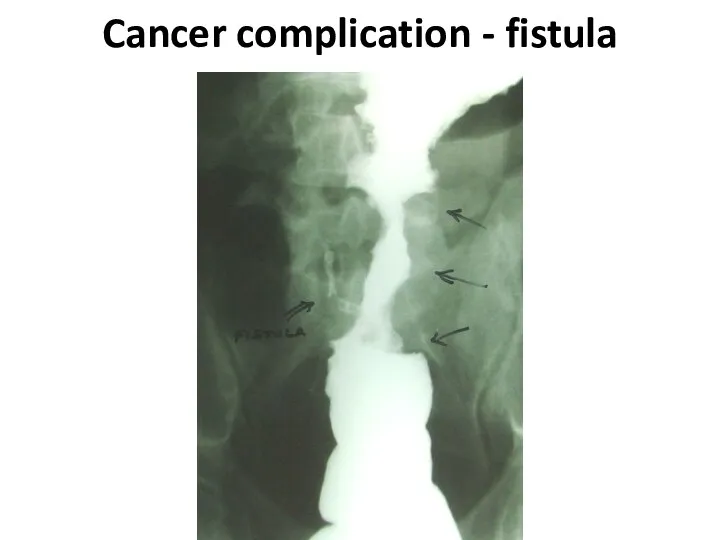
Cancer complication - fistula
Слайд 59Cancer complication - fistula
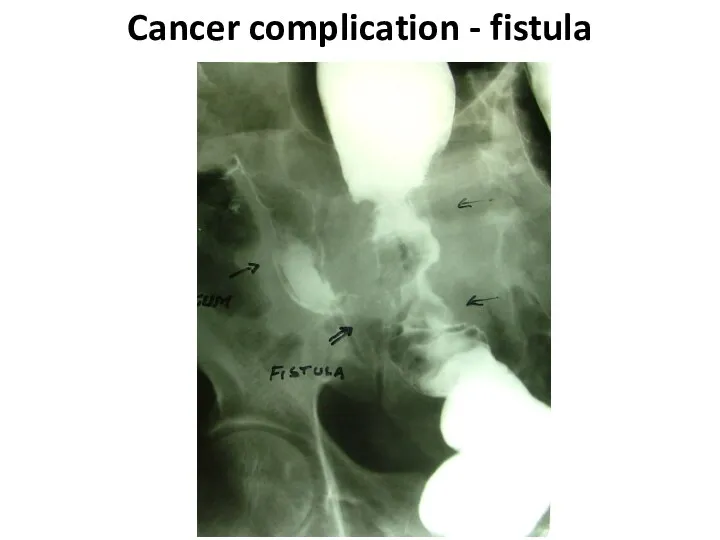
Cancer complication - fistula
Слайд 60Cancer complication - fistula
Cancer complication - fistula
Слайд 61complications
The intestinal bleeding happens, as a rule, insig-nificant. Sometimes it is shown
complications
The intestinal bleeding happens, as a rule, insig-nificant. Sometimes it is shown
Слайд 62Colon diseases
Colon diseases
Слайд 63Cancer on a background a polyposis
Cancer on a background a polyposis
Слайд 64Poliposis
Poliposis
Слайд 65Nonspecific colitises
1. Ulcerouse
2. Granulomatous (Crohn's disease)
3. Ischemic
Nonspecific colitises
1. Ulcerouse
2. Granulomatous (Crohn's disease)
3. Ischemic
Слайд 66«Drainpipe» sign
«Drainpipe» sign
Слайд 67colitis
colitis
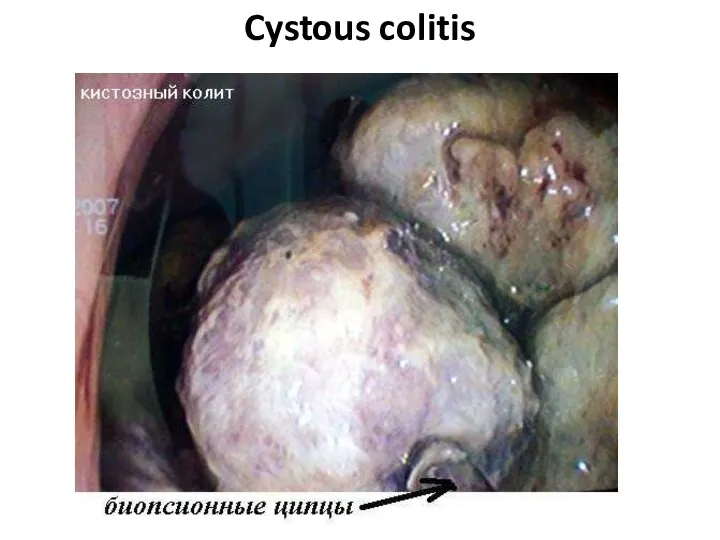
Слайд 68Cystous colitis
Cystous colitis
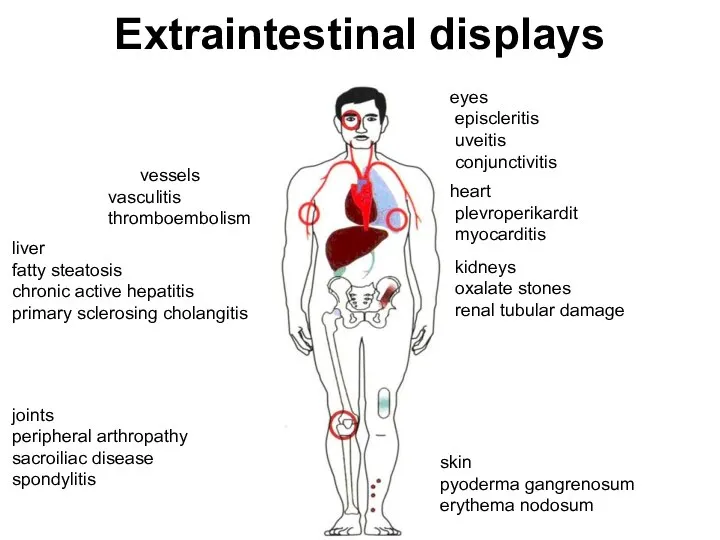
Слайд 69Extraintestinal displays
vessels
vasculitis
thromboembolism
liver
fatty steatosis
chronic active hepatitis
primary sclerosing
Extraintestinal displays
vessels
vasculitis
thromboembolism
liver
fatty steatosis
chronic active hepatitis
primary sclerosing
Слайд 70complications
Toxic megacolon
Perforation
Peritonitis
Intestinal obstruction
Bleedings
Abscesses
Fistulas
Infiltrates
complications
Toxic megacolon
Perforation
Peritonitis
Intestinal obstruction
Bleedings
Abscesses
Fistulas
Infiltrates
Слайд 71Indications to operation at ulcerouse colitis
Intestinal bleeding.
1. The frequency of bowel
Indications to operation at ulcerouse colitis
Intestinal bleeding.
1. The frequency of bowel
Слайд 72Pseudomembranous colitis
Pseudomembranous colitis
Слайд 73Polips
Hyperplastic
Tubular adenoma
Tubulary-villiferous adenoma
Villiferous adenoma
Polips
Hyperplastic
Tubular adenoma
Tubulary-villiferous adenoma
Villiferous adenoma
Слайд 74polips
polips
Слайд 75poliposis
poliposis
Слайд 76poliposis
poliposis
Слайд 77Congenital diseases
1. Hirshsprung disease
2. Megacolon
3. Dolichocolon
Congenital diseases
1. Hirshsprung disease
2. Megacolon
3. Dolichocolon
Слайд 78Hirshsprung disease
Hirshsprung disease

Слайд 79Differential diagnostics
1. Myxedema
2. Medicinal influences (morphinum and so forth)
5. Depressions
6. Schizophrenia
7.
Differential diagnostics
1. Myxedema
2. Medicinal influences (morphinum and so forth)
5. Depressions
6. Schizophrenia
7.
Слайд 80diverticuls
Diverticul
Diverticulosis
Diverticulitis
diverticuls
Diverticul
Diverticulosis
Diverticulitis
Слайд 81diverticul
diverticul
Слайд 83diverticulosis
diverticulosis
Слайд 84diverticulosis
diverticulosis
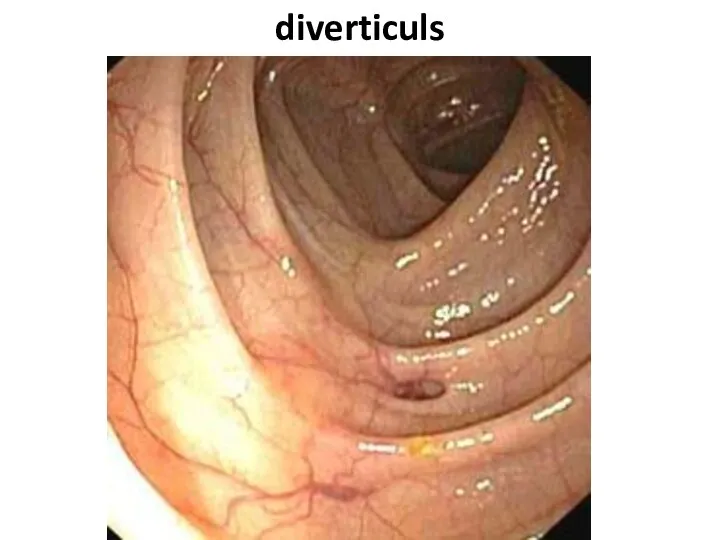
Слайд 85diverticuls
diverticuls
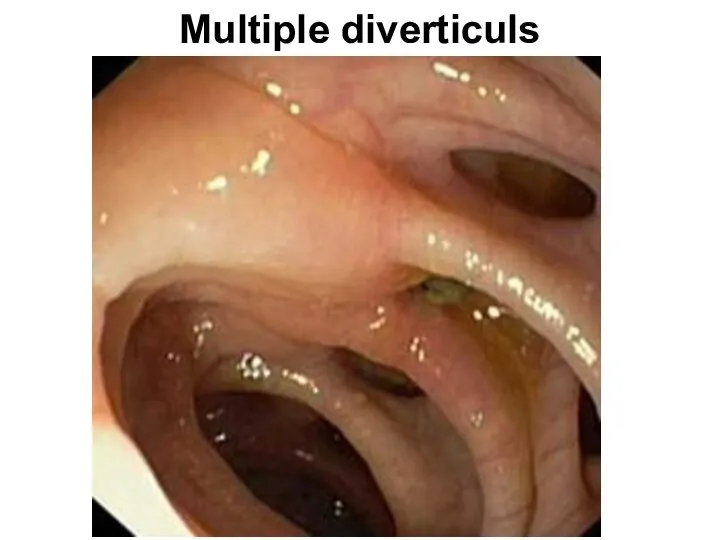
Слайд 86Multiple diverticuls
Multiple diverticuls
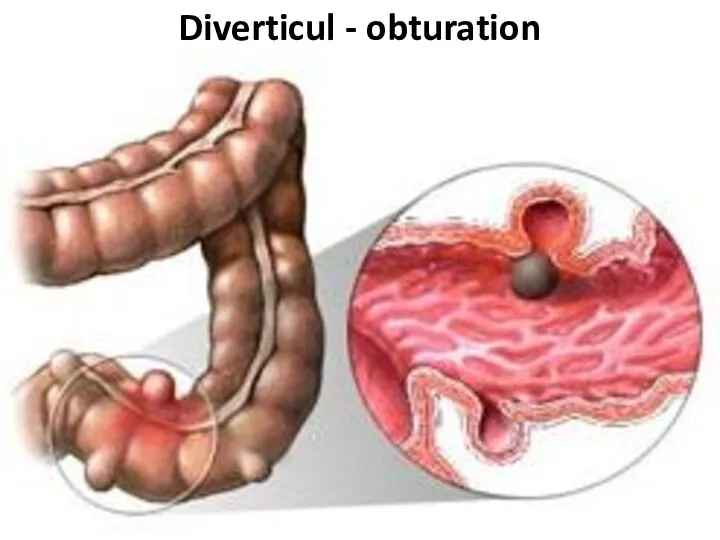
Слайд 87Diverticul - obturation
Diverticul - obturation
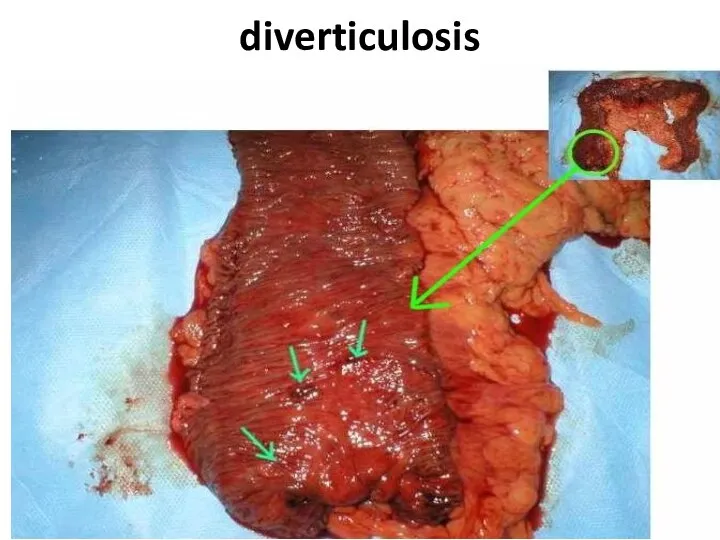
Слайд 88diverticulosis
diverticulosis
Слайд 89Fecal stone in a diverticulum
Fecal stone in a diverticulum

Слайд 90diverticulitis
diverticulitis
Слайд 91Clinical features
Acute diverticulitis is well nicknamed 'left-sided appendicitis'; an acute onset of
Clinical features
Acute diverticulitis is well nicknamed 'left-sided appendicitis'; an acute onset of
Слайд 92Clinical features
Chronic divertlcular disease exactly mimics the local clinical features of carcinoma
Clinical features
Chronic divertlcular disease exactly mimics the local clinical features of carcinoma
Слайд 93Diverticulitis
This results from infection of one or more divertlcula. An inflamed diverticulum
Diverticulitis
This results from infection of one or more divertlcula. An inflamed diverticulum
Слайд 94Diverticulitis
The Hinchey classification - proposed by Hinchey et al. in 1978[1] classifies
Diverticulitis
The Hinchey classification - proposed by Hinchey et al. in 1978[1] classifies
![Diverticulitis The Hinchey classification - proposed by Hinchey et al. in 1978[1]](/_ipx/f_webp&q_80&fit_contain&s_1440x1080/imagesDir/jpg/1165791/slide-93.jpg)
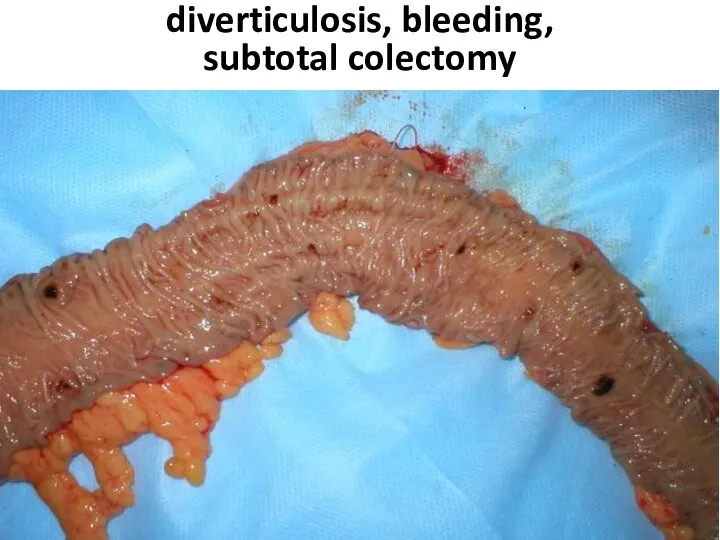
Слайд 95diverticulosis, bleeding,
subtotal colectomy
diverticulosis, bleeding,
subtotal colectomy

Слайд 96diverticulosis, bleeding,
subtotal colectomy
diverticulosis, bleeding,
subtotal colectomy
 Placenta accreta
Placenta accreta Победитель гранта Президента РФ. Социальный всеобуч. Предупреждение появления гипертонии
Победитель гранта Президента РФ. Социальный всеобуч. Предупреждение появления гипертонии Бинтовые повязки. Краткосрочные курсы
Бинтовые повязки. Краткосрочные курсы Топография мышц
Топография мышц Нарушение кровообращения - шок (С)
Нарушение кровообращения - шок (С) История развития психопатологии в России и зарубежных странах
История развития психопатологии в России и зарубежных странах Типичные переломы костей предплечья
Типичные переломы костей предплечья Пылевой бронхит
Пылевой бронхит Системная красная волчанка! (СКВ)
Системная красная волчанка! (СКВ) pathanat (1)
pathanat (1) Жүректің туа пайда болған ақаулары
Жүректің туа пайда болған ақаулары Клиническая информационная система нового поколения Дока+ и лечебно-диагностические процессы в больнице
Клиническая информационная система нового поколения Дока+ и лечебно-диагностические процессы в больнице Рацион питания
Рацион питания Кел ойнайық
Кел ойнайық Лечение ран
Лечение ран Острый лимфобластный лейкоз
Острый лимфобластный лейкоз Общая пропедевтика системы пищеварения
Общая пропедевтика системы пищеварения Самые опасные паразиты
Самые опасные паразиты Понятие шизофрении
Понятие шизофрении Вакансии. Курганская областная детская клиническая больница
Вакансии. Курганская областная детская клиническая больница Пищевые отравления
Пищевые отравления Нашақорлыққа - жол жоқ
Нашақорлыққа - жол жоқ Ингибиторы ренин-ангиотензин-альдостероновой системы (РААС)
Ингибиторы ренин-ангиотензин-альдостероновой системы (РААС) Нашақорлық - ми қыртысының созылмалы ауруы,ол ремиссия мен рецидивпен өтіп отырады
Нашақорлық - ми қыртысының созылмалы ауруы,ол ремиссия мен рецидивпен өтіп отырады БОС
БОС Использование приемов нейрофункциональной терапии в работе с детьми раннего возраста для развития артикуляционного аппарата
Использование приемов нейрофункциональной терапии в работе с детьми раннего возраста для развития артикуляционного аппарата Shiatsu
Shiatsu Храп и синдром обструктивного апноэ сна: этиология, патогенез, клиника, диагностика и лечение
Храп и синдром обструктивного апноэ сна: этиология, патогенез, клиника, диагностика и лечение